




The 52-Amino-Acid Heartbeat Micro-Peptide You Keep Measuring the Hard Way: Why a Dedicated PLN Sandwich ELISA Finally Makes Cardiac Calcium Cycle Work Quantifiable
Phospholamban (PLN) is the rarest kind of cardiac protein: a 52-amino-acid micro-peptide, an integral membrane pentamer (five transmembrane spans), and the sole endogenous brake on the heart's most important calcium pump — yet most labs still chase it exclusively with a ~6 kDa band on a 15% Tris-glycine gel and a densitometry prayer. That works if all you need is "present/absent." But the moment your experiment asks the real question — how much PLN is actually in this myocyte SR membrane prep, how did chronic β-agonist or SERCA-perturbation shift the total inhibitory pool, and can I normalize it to mg protein and put error bars on it? — the gel route starts fighting back. The Human Cardiac Phospholamban (PLN) ELISA Kit (KTE61205) from Abbkine is built for exactly that translational gap: a two-site sandwich ELISA that turns this famously small, hydrophobic, 5TM cardiac regulator into a plate-readable concentration (pg/mL) you can interpolate from a recombinant standard curve, run across tissue lysates, culture supernatants, serum, and plasma, and — crucially — trust enough to correlate with ±dP/dt_max, SERCA2a V_max, Ca²⁺ transients, and PLN phosphorylation state (Ser¹⁶/Thr¹⁷) in a single cohesive cardiac physiology story.
PLN in One Clean Paragraph: The Gatekeeper of Sarcoplasmic Reticulum Ca²⁺ Reuptake
PLN (UniProt: P26678, gene PLN, 52 aa, 6.1 kDa computed — runs ~22–25 kDa on SDS-PAGE due to anomalous migration from its hydrophobic, pentameric, SDS-resistant character) is anchored in the sarcoplasmic reticulum (SR) membrane of cardiac myocytes (and slow-twitch skeletal muscle) as a homopentamer whose N-terminal ~20 aa cytosolic domain is the functional business end. At low diastolic [Ca²⁺], the unphosphorylated N-domain binds and inhibits SERCA2a (30–50% tone), slowing Ca²⁺ reuptake into the SR → slower relaxation (↓ –dP/dt_max, ↑ τ). When β₁-adrenergic signaling fires, PKA phosphorylates PLN at Ser¹⁶ (and CaMKII at Thr¹⁷), the N-domain swings away, SERCA2a runs free, and the heart speeds up lusitropy (faster filling, shorter diastole) while the next systole lands a bigger Ca²⁺ release — a positive lusitropic + mild inotropic effect in one elegant switch.
Pathologically, PLN missense mutations (R14del, R9C, L39X, etc.) cause autosomal-dominant dilated cardiomyopathy (DCM) by either loss-of-inhibition (constitutive SERCA overdrive →能耗耗竭 → chamber dilation) or poisonous pentamer interference — and human genetics has repeatedly validated that this 52-aa peptide decides whether the left ventricle remodels or fails.
Why a Sandwich ELISA for PLN Is Tricky — And Why KTE61205 Is Explicitly Engineered for It
There are two immediate red flags any experienced cardiac biologist sees when someone says "PLN ELISA":
- 52 aa, 5TM hydrophobic peptide — there's almost no soluble domain; the only accessible linear epitopes for a sandwich pair live in the short cytosolic N-terminal tail (residues ~1–20, containing Ser¹⁶) and the tiny luminal/loop hinges.
- Pentameric/SDS-resistant behavior — PLN doesn't always run like a tidy globular protein; it needs detergent-solubilized membrane prep to release it into a state the antibody can see.
The kit solves this by using antibodies raised against recombinant human PLN (expressed in E. coli, so the full 52-aa sequence is presented in a soluble immunogenic context), then formatted into a pre-coated capture + biotinylated detection sandwich where both antibodies target accessible (typically N-terminal/loop) epitopes that survive proper lysis:
- Microplate is pre-coated with anti-PLN capture antibody.
- Standards (recombinant human PLN) and samples (serum, plasma, tissue homogenates, cell culture supernatants/lysates) added → PLN (or PLN-containing SR-membrane fragments/micelles) binds.
- Wash → biotinylated anti-PLN detection antibody (different epitope) → Streptavidin–HRP.
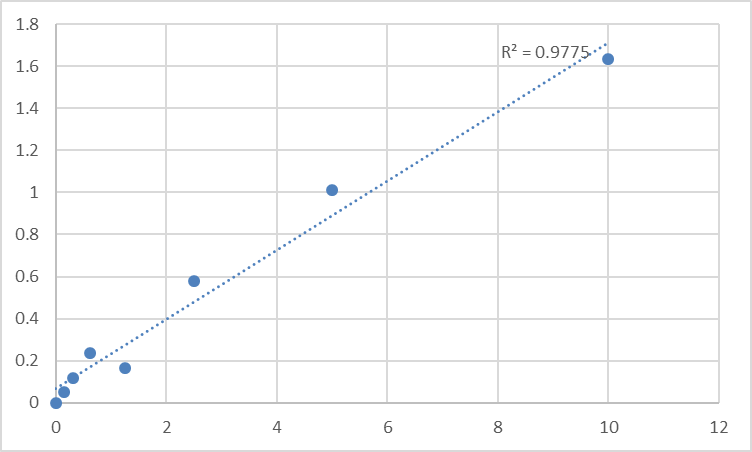
- TMB → stop → OD₄₅₀ → interpolate from the PLN standard curve.
Per the documented protocol, the standard series works out to a range of roughly 31.25 – 2000 pg/mL (lyophilized standard reconstituted to 2000 pg/mL, serial-diluted), with a practical LOD around ~15–31 pg/mL — exactly the sensitivity tier needed for tissue-level/cell-system PLN work.
The Workflow You'll Actually Run (Lysate & Tissue Version)
Critical rule upfront: because PLN is SR-membrane–embedded, whole-cell lysate in mild nonionic detergent is your friend; crude 600 × g spins often undercount it.
- Homogenize fresh/frozen LV or atrial tissue in cold buffer (50–100 mM Tris, pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100 or NP-40, protease/phosphatase inhibitors).
- Clarify at 12,000–16,000 ×g, 4°C, 15 min → keep supernatant (SR-membrane microsomes + detergent-solubilized PLN pentamers).
- BCA the same final lysate → your denominator will be pg or ng PLN / mg total protein.
- Dilute lysate into kit universal diluent (often 1:1 or 1:2 pre-dilution is advised to cut matrix effects).
- Add 100 µL sample/standard per well → incubate 37°C ~60 min (per the standard KTE61205 protocol).
- Add biotinylated detection Ab → 37°C ~60 min → wash.
- Add SA–HRP → 37°C ~30 min → wash → TMB 15 min (dark, 37°C) → stop → read 450 nm.
Performance Snapshot You'll Put in Your Methods Section
Parameter Specification (KTE61205 family)
Target Human Cardiac Phospholamban / PLN (UniProt P26678, Gene ID 5350)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → SA–HRP → TMB, 450 nm
Standard range 31.25 – 2000 pg/mL (reconstituted 2000 pg/mL stock)
Sensitivity / LOD ~15–31 pg/mL
Specificity No significant cross-reactivity with analogues (validated per batch)
Samples Serum, plasma, tissue homogenates, cell culture supernatants/lysates
Assay time ~2.5–3.5 hours typical (per protocol steps)
Status For Research Use Only; not for clinical diagnosis
(Confirm exact reagent volumes, incubation times, and lot-specific recovery on the shipped Abbkine datasheet.)
Where Quantifying PLN Protein Actually Moves the Cardiac Paper
- β-Adrenergic signaling, lusitropy & heart failure models
Isoproterenol infusion, ISO wean, β-blocker rescue, or PDE4 inhibition — the classic prediction is "PLN Ser¹⁶ phosphorylation ↑ → relaxation accelerates." But total PLN pool size also shifts in chronic hypertrophy/aging (adaptive down-/de-regulation), and that's the number a gel can't give you cleanly. KTE61205 gives you ng/mg so the relaxation phenotype has a stoichiometric anchor.
- DCM-causing PLN mutations (R14del & family) in engineered models
iPSC-cardiomyocytes, AAV-SERCA/PLN gene-editing, or transgenic mouse-tissue lysates: show % mutant PLN protein retained (or mis-pentamerized) as a calibrated number, not a guess.
- SERCA2a-targeted therapies & calcium-cycle drug screens
If you're testing IST/calcium-sensitizer, istaroxime analogs, or adenoviral/SERCA2a gene-therapy corrections, PLN abundance is the counter-reading that explains why Ca²⁺ transients changed (SERCA brake position), not just that they changed.
- Ischemia–reperfusion, cardioplegia & SR integrity
Harsh ischemic hits can degrade SR membranes and alter PLN oligomeric state; quantifying PLN in tissue fractions (SR-enriched vs. cytosolic) helps you separate "pump regulation" from "structural membrane loss."
- Skeletal muscle & slow-twitch fiber work (where PLN also resides)
Slow-twitch/cardiac-type fibers carry PLN/SERCA2a; if your project bridges cardiac and skeletal calcium handling (e.g., Duchenne-related cardiomyopathy models), the ELISA scales cleanly across muscle types.
A Final Prep Warning Worth Printing on Your Bench
PLN is 5TM, hydrophobic, and pentameric — treat it like a membrane protein, not a cytokine.
• Don't boil-and-load your way out of the problem before the ELISA (over-boiling can aggregate the pentamer in some detergents).
• Keep detergent in the lysis at a minimum effective level (0.5–1% Triton X-100 is common) so PLN stays soluble-micellar.
• Phosphatase inhibitors matter if you plan to also run pSer¹⁶/pThr¹⁷ Western alongside — but the ELISA reads total PLN mass, so inhibition of phosphatases is mainly to protect your parallel blot, not the ELISA capture (though dephosphorylation can subtly alter conformation/epitope exposure in N-tail-directed antibodies).
The Bottom Line
PLN is only 52 amino acids, but it governs whether your left ventricle relaxes on time or drowns in its own calcium — and that makes it one of the highest-leverage micro-peptides in cardiovascular biology. Measuring it by densitometry alone leaves the most important number in your SR-calcium story as a "looks darker" guess. The Human Cardiac Phospholamban (PLN) ELISA Kit — KTE61205 from Abbkine gives you the right architecture to fix that: pre-coated capture → biotin detection → HRP–TMB → 450 nm → interpolated pg/mL, over a 31–2000 pg/mL standard curve, in a 2.5–3.5 h workflow that fits inside a real lab day and produces the kind of plate-read, normalized data that actually survives peer review.
Product Reference: KTE61205 – Human Cardiac Phospholamban (PLN) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-cardiac-phospholamban-pln-elisa-kit-kte61205/
(For Research Use Only; not for diagnostic procedures in humans.)





