




The PKA Isoform That Refuses to Leave the Brain: Why PRKAR1B Quantification Is the Missing Variable in Neuroscience, Neuromuscular Disease, and Neuronal Tumor Work
If you've ever been told "PKA is PKA — just use a pan-anti-PKA antibody and move on," you've been given a half-truth that works for biochemistry but quietly sabotages neuroscience and neuromuscular biology. The cAMP-dependent protein kinase isn't one monolith — it's a family of tetramers (R₂C₂) that splits into Type I (RIα/RIβ + catalytic subunits) and Type II (RIIα/RIIβ + catalytic subunits), and the regulatory subunits determine everything: where the holo-enzyme lives inside the cell, how it responds to cAMP gradients at synapses, and which tissues survive without it. PRKAR1B (cAMP-dependent protein kinase type I-beta regulatory subunit, RIβ, UniProt: P31321, ~381 aa, observed ~47–49 kDa) is the brain-enriched, neuron-specific RI subunit that holds the catalytic subunits in check at postsynaptic densities, dendritic spines, and neuromuscular junctions — and when it drops, relocalizes, or gets co-opted by RNA toxicity, the consequences show up as cognitive deficits, synaptic plasticity collapse, and neuromuscular degeneration. The Human PRKAR1B ELISA Kit (KTE61151) from Abbkine is built to finally give you a calibrated, two-site sandwich ELISA readout of this neuron-specific scaffold — so you're measuring it like a quantitative variable, not a "brown band on a blot that sort of looks fainter."
PRKAR1B / RIβ in a Paragraph: The Brain's Specialized cAMP Gatekeeper
The canonical PKA tetramer is (Regulatory subunit)₂(Catalytic subunit)₂. In the basal state, the R subunits bind the catalytic subunits and keep them inactive by occupying their active sites; when cAMP rises, it binds the cAMP-binding (A-B-C) domains of the R subunit, causing a conformational release — and the free C subunit goes on to phosphorylate CREB, AMPA-receptor subunits, DARPP-32, voltage-gated channels, and metabolic enzymes.
Here's the critical split:
Subunit Expression What Happens When It's Gone
PRKAR1A / RIα Ubiquitous (all tissues) Embryonic lethal — essential for basic cAMP signaling everywhere
PRKAR1B / RIβ Brain-enriched (neurons > glia; striatum, hippocampus, cortex, cerebellum), skeletal muscle, some endocrine Viable, but mice show spatial learning deficits, reduced LTP, altered striatal dopamine signaling, and neuromuscular abnormalities
PRKAR2A / RIIα Broad (heart, brain) Compensated, but cardiac phenotypes emerge
PRKAR2B / RIIβ Brain, fat, pituitary Metabolic/behavioral phenotypes
PRKAR1B is not a redundant backup — it's the isoform that anchors PKA at neuronal structures via interactions with AKAPs (A-kinase anchoring proteins) and postsynaptic density scaffolds, creating local cAMP microdomains where the kinase phosphorylates substrates that diffuse-based signaling can't reach. That's why knocking it out produces specific hippocampal LTP suppression, Morris water maze deficits, and altered cocaine-conditioned place preference rather than global cAMP collapse.
Why You Need a Sandwich ELISA for PRKAR1B (And Why "Pan-PKA" blurs the biology)
Most labs detect PRKAR1B one of three ways:
- Western blot — fine for "is it there?" but limited for quantification across 30+ samples and prone to the densitometry debate.
- Anti-PRKAR1A (RIα) pan-RI antibody — this is the real trap: RIα and RIβ are ~40% identical in the cAMP-binding domains, so pan-antibodies can't tell you how much of your PKA signal is "ubiquitous RIα" (housekeeping) vs. "neuron-specific RIβ" (plasticity & disease).
- PRKAR1B sandwich ELISA — the clean solution: two epitopes, one target, absolute ng/mL from a recombinant standard curve.
The KTE61151 kit uses exactly this architecture:
- Microplate pre-coated with a capture antibody specific for human PRKAR1B/RIβ.
- Standards + samples (tissue homogenates, cell lysates, cell culture supernatants/lysates, other biological fluids) added → PRKAR1B binds.
- Wash → biotinylated anti-PRKAR1B detection antibody (different epitope) forms the sandwich.
- Streptavidin–HRP → TMB → color ∝ bound PRKAR1B.
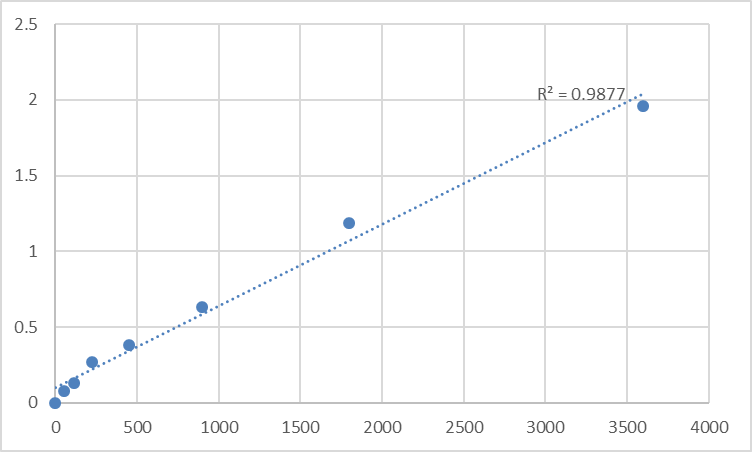
- Stop → read 450 nm → interpolate from the PRKAR1B standard curve.
Typical specs for this kit family (always confirm against your lot's CoA):
Parameter Typical KTE61151-class spec
Target Human PRKAR1B / RIβ (UniProt P31321, Gene ID 5578)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → SA-HRP → TMB, 450 nm
Dynamic Range 0.156 – 10 ng/mL
Sensitivity / LOD ~0.05–0.09 ng/mL
Intra-Assay CV < 7–8%
Inter-Assay CV < 10%
Samples Tissue homogenates (brain, muscle), cell lysates, culture supernatants, other biological fluids
Assay time ~3–5 hours
Where Quantifying PRKAR1B Actually Changes the Story
- Synaptic Plasticity, Learning & Memory Research
PRKAR1B knockout mice have normal basal transmission but impaired hippocampal CA1 LTP and poor spatial learning — exactly the phenotypes that demand a protein-level readout when you're testing psychiatric drug candidates, CREB-pathway modulators, PDE inhibitors, or antidepressant regimens. ELISA-quantified RIβ in hippocampal/cortical lysates (normalized to total protein or NeuN) gives you the scaffold abundance that explains why PKA-compartmentalization changed.
- Myotonic Dystrophy Type 1 (DM1) & RNA Toxicity
This is arguably the most clinically specific hook: DM1 is caused by a CUG expansion in DMPK RNA that sequesters CUGBP1/ETR-3 splicing regulators, which in turn alters splicing of PRKAR1B (among many transcripts). Aberrant splicing produces truncated, nonfunctional RIβ, disrupting PKA anchoring at the neuromuscular junction — contributing to the myotonia and muscle wasting that define the disease. Quantifying PRKAR1B protein (and potentially distinguishing splice isoforms with a smart antibody/epitope strategy) in muscle biopsies or myoblast lysates turns a splicing-story into a structural signaling deficit.
- Neurodevelopmental & Psychiatric Neuroscience
PRKAR1B has been implicated (in candidate and GWAS-follow-up) in schizophrenia-relevant pathways, dopaminergic signaling modulation in striatum, and substance-use disorder plasticity. Measuring RIβ protein alongside pCREB, DARPP-32 Thr34, and BDNF gives you a "local PKA-scaffold" axis that a generic pKA substrate blot can't resolve.
- Neuronal Tumor / Neuroblastoma Work
Some neuronal tumors and medulloblastoma-associated lines modulate PKA-RI isoforms as part of differentiation and growth-control circuits; PRKAR1B levels can shift with neuronal vs. glial commitment and differentiation protocols in iPSC-derived neuronal cultures — worth tracking when your readout is "did this cell mature?"
- Skeletal Muscle & Neuromuscular Junction Biology
Because RIβ is also present in skeletal muscle (NMJ postsynaptic region), quantifying it in muscle lysates from myasthenia, congenital myopathy, or denervation/reinnervation models adds a cAMP-signaling scaffold variable to your AChR-cluster and MuSK/Dok-7 panel.
- CRISPR/AAV Validation
Knocking PRKAR1B in/out or rescuing a DM1-splice defect? Report % RIβ protein remaining/rescued ± SEM from a calibrated curve, normalized to mg total protein (BCA) and, ideally, to a neuronal marker (NeuN/β-III-tubulin in co-cultures).
A Minimal Prep Blueprint (Brain & Muscle Benefit from Homogenate Care)
• For brain: rapid dissection on wet ice → cold homogenization in Tris/ sucrose or RIPA + protease/phosphatase inhibitors → centrifuge to clarify (post-nuclear → often 12,000–16,000 ×g for soluble + light-particulate fraction; keep both if you want membrane-associated RIβ, since PKA-RI complexes associate with AKAP scaffolds).
• For muscle: finely mince in liquid N₂ / cold buffer, homogenize, treat similarly.
• BCA the same lysate → express as ng PRKAR1B / mg total protein.
• Warm reagents to RT ≥ 30 min, protect TMB, stop uniformly, read 450 nm promptly, and run the full standard curve on every plate — cAMP-binding protein prep is sensitive to dilution and freeze–thaw, and the curve is your insurance.
The Bottom Line
PRKAR1B/RIβ is the PKA regulatory subunit that chose a side: the brain, the synapse, and the neuromuscular junction. It's not interchangeable with the ubiquitous RIα, and treating it like a "minor isoform" means missing the compartmentalized cAMP signaling that actually drives learning, synaptic refinement, and neuromuscular integrity. The Human PRKAR1B ELISA Kit (KTE61151) from Abbkine gives you the right tool to measure it: pre-coated capture → biotin detection → HRP–TMB → 450 nm → ng/mL, in a ~3–5 hour workflow that scales from a hippocampal-punch time-course to a muscle-biopsy cohort — so your cAMP story rests on a number you can defend, not a densitometry guess.
Product Reference: KTE61151 – Human cAMP-dependent protein kinase type I-beta regulatory subunit (PRKAR1B) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-camp-dependent-protein-kinase-type-i-beta-regulatory-subunit-prkar1b-elisa-kit-kte61151/
(For Research Use Only; not for diagnostic procedures in humans.)





