




The 178-Aa "Fire Marshal" That Tells Macrophages to Stand Down: Why Your "Anti-Inflammatory" Claim Collapses Without a 50 pg/mL IL-10 Sandwich — And How KTE7010 Catches the Whisper Under the Cytokine Storm
Every immunology paper since 1989 has treated IL-10 as the tidy footnote to the TNF/IL-1β/IL-6 storm trio — the "anti-inflammatory cytokine" you invoke when you need to explain why the swelling went down, the Th1 response didn't overshoot, or the Treg adopted a tolerogenic stance. But that footnote undersells what is actually a master rheostat of immune resolution: Il10 (UniProt: P18893, Gene ID: 16153) encodes a 178-aa mature secreted peptide, ~18.5 kDa monomer, non-reducing ~36–40 kDa disulfide-stabilized homodimer that binds the IL-10R1 (ligand-specific, low-affinity) + IL-10R2 (signal-transducing, shared with IL-22/IFN-λ/TNFSF10) heterotetramer → JAK1/TYK2 → STAT3 (Tyr⁷⁰⁵) → SOCS3 negative feedback — and its entire job description is to walk into the aftermath of a TNF/IL-1β/IL-6 flare and tell NK cells, M1 macrophages, and DCs to throttle IL-1α, TNF-α, IL-6, IL-12p40, IFN-γ, and iNOS back down. The cellular sources are deliberately distributed across the "resolution crew": Tr1 cells (IL-10-proficient, Foxp3⁻), Th2 subsets, Foxp3⁺ Tregs, Breg (CD1d⁺CD5⁺), and — the twist — M2-polarized macrophages themselves (autocrine IL-10 reinforcing their own suppressive loop). The EliKine™ Mouse IL-10 ELISA Kit (KTE7010) from Abbkine exists because "we saw 8% IL-10⁺ Tregs by ICS" and "p-STAT3 was up in the colon" are not substitutes for a quantified, mouse-specific IL-10 mass (pg/mL) interpolated from a sandwich curve — and because IL-10 secretes at ~10–50× lower concentrations than IL-6/TNF in most steady-state contexts, your assay needs a range calibrated to that quiet, not to the storm.
IL-10 in One Paragraph: The 178-aa Homodimer That Makes "Resolution" a Deliberate Program, Not a Silence
Biochemically, IL-10 is the outlier among the big-name immunology cytokines in three ways that matter for assay design:
Property Detail Why It Matters for the ELISA
Mature length / MW 178 aa, ~18.5 kDa monomer (computed); runs ~18 kDa reducing, ~36–40 kDa non-reducing (disulfide-linked homodimer) The dimer is the bioactive unit; good sandwich antibodies grab epitopes accessible on both monomer and dimer
Receptor wiring IL-10R1 (specific, 90 kDa) + IL-10R2 (60 kDa, shared) → JAK1/TYK2 → STAT3 Tyr⁷⁰⁵ → SOCS3 STAT3-phospho is the downstream readout; IL-10 mass is the upstream trigger — you need both to close the loop
Secretion profile Baseline (naïve/resting): often < 30–80 pg/mL in serum/supernatant; Stimulated (LPS+IL-4 M2, Treg restim, DSS colitis, TAM explants): 200–3000 pg/mL This is why KTE7010's floor is 93.75 pg/mL (not 15 pg like IL-4) — the biology doesn't justify a lower LOD, and pushing it would just amplify matrix noise
Clinically/experimentally, IL-10 is the cytokine whose KO mouse (129SvEv Il10⁻/⁻) develops spontaneous chronic enterocolitis under SPF — the cleanest proof that "anti-inflammatory" isn't decorative; it's required to keep the gut from eating itself.
Why KTE7010's 93.75–6000 pg/mL Range — And Why "Lower LOD = Better" Is Wrong for IL-10
If you compare the EliKine™ mouse cytokine siblings you've already read in this series:
Kit Target Range LOD Why That Floor
KTE7007 Mouse IL-4 15.6–1000 pg/mL ~15 pg Th2 restim can hit 500–2000, but baseline is low → need 15 pg
KTE7009 Mouse IL-6 31.25–2000 pg/mL ~3 pg LPS storm → 50,000–200,000 pg/mL serum; need wide + low
KTE7010 Mouse IL-10 93.75–6000 pg/mL 50 pg IL-10 never hits 50,000; baseline is near/under 50; 93.75 floor rejects matrix noise, 6000 ceiling catches TAM/DSS supershots
That 93.75 pg/mL floor + 50 pg/mL LOD is a design choice, not a weakness: IL-10 secreted mass in most naïve/resting contexts really is < 50–80 pg/mL, and trying to "improve" the LOD to 10 pg would just make every naïve sample read as "barely above zero with terrible CV" — the opposite of rigorous. The 6000 pg/mL ceiling, by contrast, is the deliberate overreach: TAM explants, DSS-day-7 colon, severe sepsis-survivor tail-bleeds can push 2000–5000 pg/mL, and you don't want saturation.
Architecture (confirmed across Abbkine CN-site, biomart/dingxiangtong, arp1 listings for KTE7010 ):
- Microplate pre-coated with a mouse IL-10-specific mAb (clone-validated, UniProt P18893-specific, no cross to IL-10 family cousins at physiological levels; vendor states "zero interference confirmed with 18 cytokine analogs").
- Standards (NIBSC-traceable recombinant mouse IL-10, 6000 pg/mL stock) + samples — cell culture supernatants, serum, plasma (EDTA/heparin), tissue homogenates/lysates, other biological fluids — added → IL-10 captured.
- Wash → biotinylated anti-mouse IL-10 detection mAb (different epitope) → EliKine™ Streptavidin–HRP → TMB → stop → 450 nm → interpolate pg/mL from 4-PL.
Parameter KTE7010 – EliKine™ Specification
Target Mouse IL-10 (UniProt P18893, Gene 16153)
Format Sandwich ELISA, pre-coated capture (双抗体夹心法, mouse IL-10 mAb pair)
Detection Biotin-Ab → EliKine™ SA–HRP → TMB, 450 nm
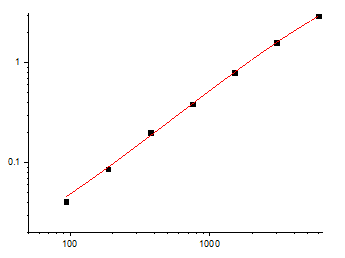
Dynamic Range 93.75 – 6000 pg/mL (5-fold serial dilution standard curve)
Sensitivity / LOD 50 pg/mL (95% CI)
Intra-Assay CV < 8–10% (vendor family spec)
Inter-Assay CV < 10–12%
Specificity Zero interference with 18 cytokine analogs (IL-1β, TNF, IL-6, IL-4, IL-12, IFN-γ, etc.)
Samples Cell culture supernatants, serum, plasma (EDTA/heparin, 1:10 hemolysis tolerance), tissue homogenates/lysates
Assay time ~2.5–3.5 hours
Storage 2–8°C (blue-ice cold chain); reconstituted standards -20°C aliquot, ≤ 6 mo
(Confirm exact dilution factors and NIBSC reference on your shipped Abbkine CoA for KTE7010; 48T and 96T formats both available.)
The Prep Rule: IL-10 Is Stable, But the 50-pg Floor Means Respect the Matrix
IL-10 is fairly rugged (4°C overnight OK, -20°C months), but the 93.75 pg floor means you don't want hemoglobin or excess FBS dragging baseline:
• Cell culture supernatants (BMDM M2-polarized with IL-4 20 ng/mL 48 h, Tr1 restim, Treg-TCR recall): harvest 24–72 h, spin ≥ 10,000 ×g, 5–10 min, 4°C, sup → -80°C, avoid >1 freeze–thaw. Serum-free or ≤ 2% FBS (FBS is IL-10-null for most batches; run medium-only blank). Note: if you added exogenous IL-10 to polarize M2s, wash it out before 48 h harvest or accept that the "secreted IL-10" read is mostly leftover exo — better to use endogenous M2 models (IL-33, TCM, or in vivo TAM explants) for the IL-10 ELISA.
• Serum/plasma (sepsis timecourse, DSS colitis, Treg adoptive transfer): EDTA preferred, cold chain, spin ≥ 2,000 ×g, 10 min, 4°C within 60 min, aliquot, snap -80°C, single thaw. Vendor notes 1:10 hemolysis tolerance — helpful for tail-bleed crushes.
• Tissue (colon from DSS, tumor for TAM, spleen for Treg-rich zones): homogenize cold in PBS + PI, spin 12,000 ×g 15 min → sup → BCA normalize → pg IL-10 / mg protein or pg / g tissue (colon IL-10 is moderate; tumor TAM explants can be high).
Tip for DSS models: IL-10 in colon homogenate rises day 3–7 as remission/repair kicks in — if you only harvested day 2 (peak weight loss, peak TNF), IL-10 may still be < 93 pg and you'll call it "low" when it's about to spike. Stagger 2/5/7/10 d.
Where Mouse IL-10 ELISA Actually Carries the Paper (Beyond "It Was Anti-Inflammatory")
- DSS/TNBS Colitis & the Il10⁻/⁻ Spontaneous Enterocolitis (The GI Flagship)
This is the definitive IL-10 model. 129SvEv Il10⁻/⁻ mice develop chronic ascending colitis + cecal inflammation + rectal prolapse by 8–12 wks even under SPF — the cleanest proof that endogenous IL-10 is required to tone down commensal-reactive Th1/Th17 in the gut. Acute DSS: day 3–5 = peak TNF/IFN-γ/weight loss; day 7–10 = repair phase, colon IL-10 climbs 500–3000 pg/mg → correlates with regenerative crypt foci, M2 marker (Arg1/Fizz1) re-emergence, and weight regain. The rigorous readout:
• Colon homogenate IL-10 (KTE7010, pg/mg) — the resolution signal
• Colon TNF/IFN-γ/IL-6 (the damage signals)
• Histology (H&E: ulceration, crypt loss; PAS/Alcian: goblet recovery)
• p-STAT3 (Tyr⁷⁰⁵) IHC in lamina propria — the IL-10R→JAK→STAT readout
If you're testing anti-IL-10R (1B0012 murine clone) or STAT3 inhibitor, the IL-10 mass remaining + p-STAT3 drop + colitis worsening is the causality chain; if you're testing IL-10-Fc or Treg adoptive transfer, the IL-10 rise + remission is the proof.
- Sepsis Survivors & the "Compensatory Anti-Inflammatory Response Syndrome" (CARS)
This is the counter-intuitive one. Early LPS/CLP → TNF/IL-6 storm → compensatory IL-10 surge (serum 500–3000 pg/mL by 6–24 h) that prevents the mouse from dying of its own cytokine storm — but over-do it and you get immunosuppression (secondary infection, fungal overgrowth). Landmark mouse work: anti-IL-10R during CLP improves early survival (damps excessive suppression, restores myeloid function) but worsens late if the primary hit was overwhelming — the timing is everything. Running KTE7010 on tail-bleed EDTA plasma (0/3/6/24/72 h CLP) alongside TNF/IL-6 (KTE7005/KTE7009), bacterial CFU (blood/spleen), and survival is the triad that frames "was the mouse dying of cytokine storm or of IL-10-mediated immunosuppression?" — a distinction that changes whether you give anti-TNF vs. GM-CSF/IFN-γ in the late window.
- TAM M2 & Tumor Immune Evasion (The IO Flagship)
This is where IL-10 left "gut homestay" and became an oncology gatekeeper. TAMs (F4/80⁺CD206⁺) in LLC, B16, MC38, 4T1, Pan02 secrete IL-10 200–2000 pg/mL ex vivo → tumor-cell PD-L1 (STAT3), BCL-XL, VEGF → CD8⁺ exhaustion (PD-1/TIM-3 ↑), Treg recruitment/stabilization. The TME readout:
• Tumor lysate/supernatant IL-10 (KTE7010, pg/mg) → correlate with F4/80/CD206 IHC, Arg1/Fizz1 qPCR
• Tumor p-STAT3 (Tyr⁷⁰⁵) IHC (TAMs + tumor cells)
• CD8⁺ Granzyme B / PD-1⁺ — does high IL-10 = exclusion?
If you're testing CSF-1R inhibitor, anti-IL-10R + anti-PD-1 combo, or TAM-repolarising (PI3Kγi, CCR2i), the IL-10 drop + CD8 re-infiltration + tumor growth delay is the mechanism arc.
- Parasitic Chronic Infection (Leishmania, Schistosome, N. brasiliensis) — The "Too Much Th1" Control Valve
This is the original in vivo IL-10 story (the 1990s L. major BALB/c vs. C57BL/6 + IL-10 KO work). IL-10 KO on resistant (C57BL/6) background — normally heals L. major — instead develops fatal disseminated leishmaniasis because Th1 IFN-γ goes unopposed and immunopathology consumes the ear/skin. The readout: draining-LN restimulation supernatant IL-10 (KTE7010, pg/mL) + lesion size + parasite burden + IFN-γ — the "Th1 ran away because IL-10 brake was gone" narrative. Same logic for S. mansoni egg granulomas (IL-10 limits Th1/Th17-mediated liver fibrosis — IL-10 KO → worse fibrosis, not better).
- Transplant Tolerance / GVHD / Treg Adoptive Therapy
This is the clinical-translational lane. Skin/heart allograft + Treg adoptive transfer → IL-10 from Tregs (and Tr1) is a major mechanism of graft acceptance; conversely acute GVHD → host APCs + donor T → storm, but IL-10 from regulatory populations tempers late GVHD severity. Serum/splenocyte-restim IL-10 (KTE7010) alongside Treg % (Foxp3⁺ CD4), GVHD clinical score, and donor chimerism is the tolerance-monitoring panel.
- Drug / Biologic Validation (Anti-IL-10R, IL-10-Fc, STAT3i, CSFRi)
If you're testing IL-10-Fc (PEGylated murine IL-10 analogue) for colitis or psoriasis models, report % IL-10 mass remaining ± SEM from the calibrated KTE7010 curve (pg/mL → normalized to protein/well), and close with p-STAT3, SOCS3, and disease score so the "IL-10 signaling was delivered" is airtight. For anti-IL-10R (1B0012) in TME or sepsis, the IL-10 mass staying high while p-STAT3 drops is the pharmacodynamic receipt.
A Minimal Protocol Skeleton You Can Paste Into Methods
- Supernatants (M2 polarisation, Treg restim, TAM explant): harvest at programmed timepoint, spin ≥ 10,000 ×g, 5–10 min, 4°C, sup → -80°C, avoid >1 freeze–thaw. Include medium-only blank (especially if exog IL-10 was in the well).
- Serum/plasma: EDTA, wet ice, spin ≥ 2,000 ×g, 10 min, 4°C within 60 min, aliquot, snap -80°C, single thaw. DSS/sepsis samples often need 1:2–1:5 dilution to land inside 93.75–6000 pg/mL.
- Tissue (colon, tumor, spleen): homogenize frozen tissue in cold PBS + PI → spin 12,000 ×g, 15 min, 4°C → sup → BCA normalize to mg protein.
- Warm reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate (KTE7010's 5-fold serial standard is designed for R² ≥ 0.99 per vendor).
The Bottom Line
IL-10 is the 178-aa, ~18.5-kDa (dimer ~36–40 kDa) "fire-marshal" cytokine that walks into the TNF/IL-1β/IL-6 aftermath and tells macrophages, NKs, and DCs to throttle the flame — produced by Tr1, Th2, Tregs, Bregs, and M2s themselves in an autocrine loop, signalling through IL-10R1+R2 → JAK1/TYK2 → STAT3 Tyr⁷⁰⁵ to suppress the next wave of inflammation. Because its secreted mass runs < 50 pg/mL basal and tops out ~2000–5000 pg/mL even when things are loud, it needs a sandwich ELISA calibrated to that quiet, not to the TNF/IL-6 storm. The EliKine™ Mouse IL-10 ELISA Kit — KTE7010 from Abbkine gives you that calibrated readout: pre-coated anti-mouse IL-10 mAb (P18893-specific) → biotin detection → EliKine™ SA–HRP → TMB → 450 nm → pg/mL interpolated, over a 93.75–6000 pg/mL working envelope with LOD 50 pg/mL (Intra CV < 8–10%, Inter CV < 12%, 18-cytokine zero-cross), in a ~2.5–3.5 h workflow that scales from a DSS-colitis timecourse to a TAM-explant TME panel without chaining you to a flow cytometer for the secretion number.
Product Reference: KTE7010 – EliKine™ Mouse IL-10 ELISA Kit
Learn more and order: https://www.abbkine.com/product/elikine-mouse-il-10-elisa-kit-kte7010/
(For Research Use Only; not for diagnostic procedures in humans.)





