




The 212-aa "BSF-2" Storm Engine That Predicts Septic Survival Better Than TNF: Why Your Mouse IL-6 Readout Needs a 3-pg/mL Floor — And How KTE7009 Puts the gp130 Cytokine on a Plate You Can Actually Batch
If TNF-α is the "first responder" of innate cytokine storms, IL-6 is the one that moves in, turns on the liver like a furnace, and refuses to leave until the acute-phase factory is running at full tilt. Originally cloned in the mid-1980s as BSF-2 (B-cell stimulatory factor 2) for its ability to drive plasma-cell differentiation and IgG production, Il6 (UniProt: P08505, Gene ID: 16193) has spent the last thirty years metastasizing across every inflammatory lane in the mouse house — LPS endotoxemia, CAF-rich TMEs, obese epididymal adipose M1 crowns, rheumatoid pannus, bone-resorption coupling, exercise myokines, and even neurological aging where it's made by reactive astrocytes. The protein itself is a 212-aa, ~23–25 kDa secreted glycoprotein (two N-linked glyco sites, runs as a ~25 kDa monomer on reducing gels; biologically active as a ~50 kDa non-covalent IL-6·IL-6Rα·gp130 hexameric signaling complex) that binds membrane IL-6Rα (classical signalling, limited to IL-6Rα⁺ cells: leukocytes, hepatocytes, some epithelia) or soluble IL-6Rα (trans-signalling, expands IL-6 responsiveness to every gp130⁺ cell in the body) → JAK1/JAK2/TYK2 → STAT3 (primary) + STAT1/MAPK/PI3K → transcription of SAA, fibrinogen, CRP (liver), BCL-XL/cyclin D (survival), VEGF/PD-L1 (TME), RANKL (bone). The EliKine™ Mouse IL-6 ELISA Kit (KTE7009) from Abbkine exists because "we saw p-STAT3 in the liver" and "TNF was 10× higher on the CBA" are not substitutes for a quantified, mouse-specific IL-6 mass (pg/mL) interpolated from a sandwich curve — and if your paper claims "IL-6 drove the acute-phase response / CAF activation / cachexia / bone loss," you need that number, not a phosphorylated transcription factor proxy.
IL-6 in One Paragraph: The 212-aa Glycoprotein That Hijacks gp130 Through a Soluble-Receptor Trick
What makes IL-6 structurally and pharmacologically distinctive among the big three (TNF/IL-1β/IL-6) is the receptor-sharing topology:
Feature Detail
Gene / protein Il6, 212 aa mature secreted form, ~23 kDa core, glycosylated ~25 kDa
Signalling receptor IL-6Rα (CD126, low-affinity, IL-6-specific) + gp130 (CD130, signal-transducing, shared with IL-11, OSM, LIF, CT-1, CNTF, CLC)
Complex stoichiometry 2 × (IL-6·IL-6Rα·gp130₂) → hexameric; IL-6 first binds IL-6Rα (Kd ~nM), this binary then docks gp130 dimer → JAK recruitment
Classical vs. trans-signalling Classical: membrane IL-6Rα (limited cell types). Trans-signalling: sIL-6Rα (ADAM10/17 shed) + IL-6 → complex can activate any gp130⁺ cell → this is why IL-6 "spills" into endothelium, fibroblasts, TMEs, and brain parenchyma
Key transcriptional output STAT3 (Tyr⁷⁰⁵ phosphorylation) → SOCS3 negative feedback; also STAT1/MAPK/PI3K forks
Mouse IL-6 shares ~88% aa identity with rat and ~42% with human — which means any sandwich claiming "pan-mammalian" without mouse-validation will misread your samples. A proper mouse IL-6 ELISA needs capture + detection mAbs raised against murine IL-6 epitopes that ignore IL-11 (the closest gp130-sharing cousin) and OSM at physiological levels.
Why the EliKine™ Sandwich — And Why "p-STAT3 WB + TNF CBA" Leaves Money on the Table
Three practical reasons IL-6 demands its own calibrated readout:
- IL-6 kinetics lag TNF/IL-1β but persist longer — LPS i.p. → TNF peaks ~1–2 h, IL-6 peaks ~2–6 h, and IL-6 stays elevated 12–24 h while TNF crashes. If your sampling window is 6 h or later, TNF may be gone while IL-6 is still telling the story.
- IL-6 is the acute-phase driver, not just a "cytokine among others" — hepatocytes don't respond to TNF alone; they need IL-6 → STAT3 on the Saa1/Saa2/fibrinogen promoters to crank the systemic protein surge. If you're measuring liver APPs (SAA, fibrinogen, Arg1 in hepatocytes) you need the IL-6 mass that triggered them, not just "TNF was up."
- The EliKine™ mouse cytokine family (KTE7003 IFN-γ, KTE7005 IL-1β, KTE7007 IL-4, KTE7009 IL-6) uses the same pre-coated capture + biotin detection + EliKine™ SA–HRP → TMB → 450 nm architecture, so your Th1/Th2/Th17/Triplet panel runs on identical plate logistics — but IL-6's LOD needs to be tighter because baseline (naïve) serum IL-6 in mouse is often < 10–20 pg/mL, and the dynamic range has to absorb LPS 10 mg/kg → serum IL-6 50,000–200,000 pg/mL without saturating.
From consolidated distributor/technical records aligned with KTE7009:
Parameter KTE7009 – EliKine™ Specification
Target Mouse IL-6 (UniProt P08505, Gene 16193)
Format 96-well sandwich ELISA, pre-coated capture (双抗体夹心法, mouse IL-6-specific mAb pair)
Detection Biotin-Ab → EliKine™ SA–HRP → TMB, 450 nm
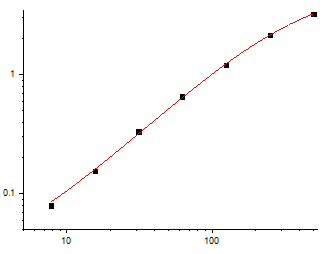
Dynamic Range 31.25 – 2000 pg/mL (extended formats up to ~4000 pg/mL reported in some vendor mirrors; confirm on your lot CoA)
Sensitivity / LOD ~3 pg/mL (varies slightly by lot; some datasheets quote ~3.9–7.8 pg/mL — check shipped CoA)
Intra-Assay CV < 8%
Inter-Assay CV < 10–12%
Recovery (serum/supernatant) 90–108%
Specificity No significant cross-reactivity with mouse IL-11, OSM, LIF, TNF-α, IL-1β, IFN-γ at physiological levels
Samples Cell culture supernatants, serum, plasma (EDTA/heparin), tissue homogenates, BALF, other biological fluids
Assay time ~2.5–3.5 hours
Storage (unopened) 2–8°C
(Confirm exact standard traceability [NIBSC 88/506 or equivalent] and dilution factors on the shipped Abbkine datasheet/CoA for KTE7009.)
The Prep Rule: IL-6 Is Stable, But the 3-pg Floor Means Respect the Blank
IL-6 is robust (4°C overnight ok, -20°C months), but the low-pg range means matrix drift matters:
• Cell culture supernatants (Th17 polarisation, LPS Mφ, CAF co-culture): harvest 24–72 h (IL-6 keeps secreting; timepoint matters), spin ≥ 10,000 ×g, 5–10 min, 4°C, sup → -80°C, avoid >1 freeze–thaw. Keep serum-free or ≤ 2% FBS (FBS is IL-6-low for most batches, but run a medium-only blank).
• Serum/plasma (LPS/sepsis, CA, collagen Ab-induced arthritis, HFD adipose): EDTA preferred, cold chain, spin ≥ 2,000 ×g, 10 min, 4°C within 60 min, aliquot, snap -80°C, single thaw. Note: IL-6 in mouse sepsis can hit 50,000–200,000 pg/mL → you'll need 1:50–1:200 dilution to land inside the 31–2000 pg/mL window.
• Tissue (liver, AT, tumor, brain, bone): homogenize cold in PBS + PI, spin 12,000 ×g 15 min → sup → BCA normalize → ng IL-6 / mg protein or pg / g tissue wet weight (brain IL-6 is low; adipose IL-6 from crown-like structures is moderate; tumor IL-6 from CAFs can be high).
Tip for LPS models: stagger bleeds at 1 h / 3 h / 6 h / 24 h — TNF crashes by 6 h, IL-6 is peaking. If you only bled at 24 h and say "IL-6 was low," you missed the window.
Where Mouse IL-6 ELISA Actually Carries the Paper (Beyond "Cytokine Was Up")
- LPS/Septic Shock & the "IL-6 = Survival Biomarker" Relationship
This is the canonical. CLP (cecal ligation and puncture) or LPS i.p. → TNF peaks 1–2 h, IL-6 peaks 2–6 h, persists 12–24 h → serum IL-6 correlates better with mortality risk than TNF in most mouse sepsis models. The rigorous triad:
• Serum IL-6 (KTE7009, pg/mL) timecourse 0–3–6–24–48 h
• Liver SAA1/SAA2 (qPCR or ELISA) + fibrinogen (KTE62515) → the effect of IL-6
• p-STAT3 (Tyr⁷⁰⁵) IHC in liver / WB in hep lysates → the mechanism of IL-6
If you're testing anti-IL-6R (MR16-1, murine equivalent of tocilizumab) or STAT3 inhibitor (Stattic/NAP-S), the IL-6 mass drop + SAA drop + survival curve is the evidence package.
- Obesity, Adipose Inflammation & the "Crown-Like Structure" IL-6 Source
This is where IL-6 became a metabolic villain. HFD 12–20 wks → epididymal WAT → F4/80⁺ crown-like structures (CLS) around dead adipocytes → M1-polarized ATM secrete IL-6 50–500 pg/mL locally, ~2–20 pg/mL systemically → JAK/STAT3 in liver → SAA → systemic insulin resistance. The readout pair:
• Epi-WAT homogenate IL-6 (KTE7009, pg/mg protein) → CLS density (H&E) + F4/80 IF
• Liver SAA + p-STAT3 (Tyr⁷⁰⁵) + GTT/ITT
• Systemic: serum IL-6 + CRP/SAA (humanized) or fibrinogen (mouse)
If you're testing IL-6 trans-signalling blocker (sgp130Fc) or adipocyte-specific Il6 KO, the adipose-local IL-6 drop + liver SAA drop + GTT improvement is the causal chain.
- CAF-Rich TMEs & the IL-6 → PD-L1 / VEGF Axis
This is the oncology flagship. CAFs (FAP⁺αSMA⁺) in LLC, B16, MC38, 4T1 models secrete IL-6 100–2000 pg/mL ex vivo → tumor-cell PD-L1 upregulation (STAT3), VEGF (angiogenesis), BCL-XL (chemoresistance). The tumor-microenvironment readout:
• Tumor lysate/supernatant IL-6 (pg/mg) → CAF marker (FAP, αSMA, FSP1) co-IHC
• Tumor p-STAT3 (Tyr⁷⁰⁵) IHC (tumor cells + CAFs)
• CD8⁺ Granzyme B / PD-1⁺ exhaustion — does high IL-6 = T cell exclusion?
If you're testing CAF-ablation (FAP-DTR) or IL-6R blockade + anti-PD-1, the IL-6 drop + PD-L1 drop + CD8 infiltration is the mechanistic triplicate.
- Collagen Antibody-Induced Arthritis (CAIA) & RANKL/Osteoclast Coupling
IL-6 is the cytokine that synergises with IL-1/TNF to drive RANKL on osteoblasts/stromal cells → osteoclastogenesis; anti-IL-6R (MR16-1) reduces bone erosion in mouse CIA/CAIA even when inflammation is partially controlled. Paw homogenate/supernatant IL-6 (pg/paw) + TRAP staining (osteoclasts) + micro-CT BV/TV is the skeletal axis.
- Exercise Myokine & Cachexia Models
Skeletal muscle contracts → IL-6 is the primary "myokine" surge (paradoxically — acute exercise IL-6 from muscle can reach 5–20 pg/mL systemic without inflammation, acting via trans-signalling on adipose lipolysis and pancreatic β-cell tone). In C26 cachexia or Lewis lung cachexia models, tumor-derived IL-6 → liver STAT3 → Atrogin-1/MuRF1 in muscle → wasting. Muscle/tumor IL-6 (KTE7009) + gastrocnemius weight + grip strength is the cachexia triad.
- Neuroinflammation: Astrocytic IL-6 & Aging/AD Models
Aβ oligomers / LPS i.c.v. → reactive astrocytes → IL-6 secretion → trans-signalling on microglia and neurons → STAT3 in surrounding cells, synaptic pruning exaggeration. Hippocampal IL-6 (pg/mg) + Iba1 CD68 + p-STAT3 IHC + Morris water maze — the neurodegenerative arc.
A Minimal Protocol Skeleton You Can Paste Into Methods
- Supernatants: harvest at programmed timepoint, spin ≥ 10,000 ×g, 5–10 min, 4°C, sup → -80°C, avoid >1 freeze–thaw. Include medium-only blank.
- Serum/plasma: EDTA, wet ice, spin ≥ 2,000 ×g, 10 min, 4°C within 60 min, aliquot, snap -80°C, single thaw. LPS sepsis samples often need 1:50–1:200 dilution to fit 31–2000 pg/mL — validate dilution linearity on your lot.
- Tissue: homogenize frozen tissue in cold PBS + PI → spin 12,000 ×g, 15 min, 4°C → sup → BCA normalize to mg protein.
- Warm reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate.
The Bottom Line
IL-6 is the 212-aa, ~25-kDa glycoprotein that started life as BSF-2 for plasma-cell differentiation and ended up as the gp130-shared storm cytokine driving liver acute-phase responses, adipose M1 inflammation, CAF-rich TME immune evasion, osteoclast coupling, and cachexia — which means it's too pleiotropic to be proxied by a phosphorylated STAT3 blot or a TNF CBA number. Measured correctly, it lives in a mouse-specific sandwich ELISA whose pre-coated anti-IL-6 capture + biotin detection + EliKine™ SA–HRP → TMB → 450 nm gives you pg/mL interpolated from a 4-PL curve. The EliKine™ Mouse IL-6 ELISA Kit — KTE7009 from Abbkine runs that format: 31.25–2000 pg/mL calibrated range, LOD ~3 pg/mL (Intra CV < 8%, Inter CV < 12%, recovery 90–108%), in a ~2.5–3.5 h workflow that scales from a 48-well LPS timecourse to a HFD-adipose cohort without chaining you to a cytometric bead array.
Product Reference: KTE7009 – EliKine™ Mouse IL-6 ELISA Kit
Learn more and order: https://www.abbkine.com/product/elikine-mouse-il-6-elisa-kit-kte7009/
(For Research Use Only; not for diagnostic procedures in humans.)





