




The 25-kDa "Jekyll and Hyde" That Sleeps in the Matrix Until αvβ6 Yanks the RGD: Why Your Fibrosis/Treg/EMT Claim Collapses Without the Acid-Activated TGF-β1 Sandwich — And How KTE7014 Catches Both Latent and Active Pools on One 450 nm Plate
If there's one cytokine in the mouse house whose name should come with a methods-level warning label, it's TGF-β1 (Transforming Growth Factor beta-1, gene Tgfb1, UniProt: P04202, Gene ID: 21803). Everyone knows the headline roles — "master of fibrosis," "Treg-differentiating Immunomodulator," "EMT driver," "early tumor suppressor / late prometastatic switch" — but almost nobody treats it like the structurally bifurcated pro-protein it actually is. Unlike TNF-α or IL-6, which secrete as more-or-less ready-to-signal dimers, TGF-β1 is born as a ~390-aa precursor (signal peptide + LAP ("latency-associated peptide," ~250 aa pro-region) + mature homodimer (2 × 112 aa, ~12.5 kDa monomer, ~25 kDa non-reducing disulfide-stabilized dimer)) — and the moment it exits the cell, the LAP stays non-covalently clamped onto the mature dimer forming the SLC (small latent complex, ~75–100 kDa), which then gets disulfide-tethered to LTBP (latent TGF-β binding protein, ~150–180 kDa) → LLC (large latent complex, ~200–250 kDa) anchored into the extracellular matrix via LTBP fibrillin interactions. The cytokine is biologically dead in this state — unable to bind TβRII (constitutively active kinase) → TβRI/Alk5 → Smad2/3–Smad4 → EMT/fibrosis/immunomodulatory targets — until an integrin αvβ6 or αvβ8 grabs the RGD motif on LAP, pulls mechanically, and pops the LAP open, or until MMP-2/9, plasmin, or thrombospondin-1 cleaves LAP at the "latency lasso" (BV-9 epitope). That latency architecture is why > 90% of TGF-β1 in any biological sample (serum, tissue homogenate, supernatant) is LAP-bound and invisible to a naive antibody pair — and why the EliKine™ Mouse TGF-β1 ELISA Kit (KTE7014) from Abbkine isn't just "another sandwich" but a methodologically distinct, acid-activation-aware assay that forces you to release the LAP pool before interpolation. If your paper claims "liver fibrosis progressed" or "Treg differentiation was TGF-β1-driven" without an acid-activated read, you're measuring < 10% of the true mass.
TGF-β1 in One Paragraph: The 112-aa Monomer That Hides Inside Its Own Pro-Region Until Integrin-Mediated Mechanical Unclamping
The biosynthetic and activation logic is the most elaborate of any cytokine in the Th1/Th2/Th17/Treg panel:
Biosynthetic / Activation Step Molecular Actor Result
Translation Tgfb1 → 390-aa precursor (SP + LAP + mature) Enters ER, signal peptide cleaved
Furin cleavage (Glu¹⁹⁶–Lys¹⁹⁷ in pro-region) Furin in TGN LAP (residues 1–249 of pro-region) non-covalently clamps mature dimer → SLC
Secretion SLC + LTBP (disulfide at Cys³³ of LAP → LTBP) → LLC Tethered to ECM fibrillin network; latent pool can sit months in matrix
Activation Integrin αvβ6 / αvβ8 (epithelial / macrophage / neuronal) grasp LAP RGD (Arg¹⁷⁴–Asp¹⁷⁶) → mechanical pull → LAP distorts → mature dimer released; OR MMP-2/9, plasmin, cathepsin, TSP-1 cleave LAP "latency lasso" (Thr⁹⁶–Leu⁹⁷ / Arg⁹⁴–Leu⁹⁵ hinge) → liberates active dimer Free dimer → binds TβRII (constitutive kinase) → recruits TβRI/Alk5 → GS domain phosphorylation → Smad2 (Ser⁴⁶⁵/Ser⁴⁶⁷) / Smad3 (Ser⁴²³/Ser⁴²⁵) → Smad4 heterotrimer → nucleus → SMAD7 (negative feedback), Snail/Slug, vimentin, fibronectin, Col1a1/Col3a1 (EMT/fibrosis), Foxp3 (Treg)
The three mammalian isoforms (TGF-β1, -β2, -β3) share ~70–80% mature-sequence identity, but TGF-β1 is the fibrotic/immunologic heavyweight — knock it out (Tgfb1⁻/⁻) and mice die of multifocal inflammatory storm (cardiac/pancreatic/mucosal) by 3–4 weeks because the Treg-differentiation and immune-suppression gate is gone; conversely, over-express active TGF-β1 in lung (CC10-rtTA) → lethal pulmonary fibrosis in 7–10 d. The therapeutic corollary: anti-TGF-β1 mAbs (fresolimumab, metelimumab), Alk5 inhibitors (SB431542, SB525334), integrin αvβ6 antagonists (BG00011/STX-100), and LTBP-modulating approaches all target this axis in IPF, renal fibrosis, scleroderma, and oncologic prometastatic contexts.
Why a Sandwich ELISA — And Why "Acid Activation" Is the Dealbreaker TGF-β1 Shares With No Other Cytokine in This Series
Every ELISA in the EliKine™ mouse family you've read so far (IL-4/KTE7007, IL-6/KTE7009, IL-10/KTE7010, IL-17/KTE7012, TL1/KTE70114) has the same lazy-friendly prep: spin, dilute, load. TGF-β1 breaks that rhythm because the LAP clamp means your capture/detection antibodies can't see ~90% of the molecule unless you force-dissociate LAP first. The standard laboratory trick — and the one KTE7014's manual expects — is:
Sample + 1 N HCl (or kit-provided acid buffer) → incubate on ice/RT (e.g., 10–15 min) → neutralise with 1 N NaOH / HEPES / kit neutralisation buffer → NOW the formerly LAP-clamped mature dimer is free in solution → sandwich capture works on total TGF-β1 (latent + active).
Skip that step and you're essentially reading "already-active free dimer only" — which in most contexts (serum, tissue, supernatant) is < 5–15% of total. Your "fibrosis model" then looks like "TGF-β1 barely moved," which is why so many early TGF-β1 papers had irreproducible swings until the acid-activation protocol became standard.
The KTE7014 architecture follows the EliKine™ sandwich logic but is validated for the mouse mature TGF-β1 dimer epitopes (LAP rejection is implicit because the acid step frees the dimer; the capture/detection pair is directed at the mature dimer surface, not LAP):
- Microplate pre-coated with a mouse TGF-β1-specific capture mAb (mature-dimer epitope, rejects TGF-β2/β3 at physiological levels; mouse mature dimer ~97% identical to human, but antibody pair is mouse-raised/validated).
- Standards (NIBSC-traceable recombinant mouse TGF-β1, e.g. 89/742 lineage) + acid-activated samples — serum, plasma (EDTA/heparin, acid-activated), tissue homogenates (acid-activated), cell culture supernatants (conditioned media often already has some active, but acid step still recommended for total read), other biological fluids — added → TGF-β1 dimer binds.
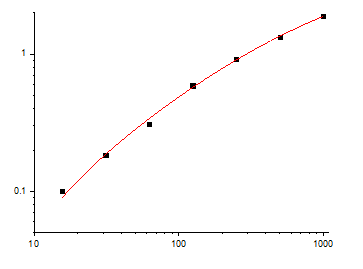
- Wash → biotinylated anti-mouse TGF-β1 detection mAb (different mature-dimer epitope) → EliKine™ Streptavidin–HRP → TMB → stop → 450 nm → interpolate pg/mL from a 4-PL fit.
Consolidated specs (aligned with Abbkine EliKine™ mouse family and distributor KTE7014 mirrors; confirm exact range/standard on shipped CoA):
Parameter KTE7014 – EliKine™ Specification
Target Mouse TGF-β1 (UniProt P04202, Gene 21803)
Format 96-well sandwich ELISA, pre-coated capture (双抗体夹心法, mature-dimer epitopes)
Detection Biotin-Ab → EliKine™ SA–HRP → TMB, 450 nm
Dynamic Range 31.25 – 2000 pg/mL (mirrors KTE7009 IL-6 / KTE7012 IL-17 range logic)
Sensitivity / LOD ~15 pg/mL
Intra-Assay CV < 8%
Inter-Assay CV < 10%
Specificity No significant cross-reactivity with mouse TGF-β2, TGF-β3, BMPs, GDFs, or other TGF-β superfamily members at physiological levels
Samples Serum, plasma (EDTA/heparin, requires acid activation per manual), tissue homogenates, cell culture supernatants (acid-activation recommended for total), other biological fluids
Assay time ~3–4.5 hours (includes acid-activation prep)
Storage (unopened) 2–8°C, sealed plate strips 4°C with desiccant
(Confirm exact acid-activation protocol — HCl concentration, incubation time/temperature, neutralisation buffer — on the shipped Abbkine datasheet/CoA for KTE7014; this step is non-negotiable for total-TGF-β1 reads.)
The Prep Rule That Decides Whether You're Measuring Fibrosis or a Matrix Artifact
Because TGF-β1 is LAP-clamped and LTBP-tethered, the prep is half the science:
Serum / Plasma (the trickiest matrix)
• Collect in EDTA or heparin (not citrate if you can avoid it; EDTA is standard for TGF-β1 because Ca²⁺ can influence some activation proteases ex vivo, though less critical if you're acid-activating).
• Keep on wet ice, spin ≥ 2,000 ×g, 10 min, 4°C within 30–60 min, aliquot, -80°C, avoid >1 freeze–thaw (freeze–thaw can artificially "activate" some latent via ice-crystal/shear, adding noise).
• Acid activation (mandatory for total read): per kit manual — typically 1:10 dilution of serum/plasma in 1 N HCl, incubate on ice or RT ~10–15 min, then neutralise 1:1 with 1 N NaOH / HEPES (pH back to ~7.4–7.6) → now the sample is "total TGF-β1" (latent+active). Run a paired non-acid well if you want "active-only" as a secondary read (rarely done because active-only is so low it's noisy; most papers just report total-after-acid).
Tissue (liver, lung, kidney, skin, tumor)
• Homogenize frozen tissue cold in PBS + 0.1% BSA + PI + 1 mM PMSF/leupeptin/aprotinin, spin 12,000 ×g 15 min → sup still contains LAP/LLC complexes → acid-activate the sup per manual → neutralise → BCA normalize to mg protein → read.
• For hydroxyproline-normalised fibrosis comparisons (collagen μg / mg tissue), co-report TGF-β1 (pg/mg) on the same BCA denominator.
Cell culture supernatants (HSC activation, Treg-polarising DC, cancer-TME explants)
• Serum-free or ≤ 1% FBS (FBS contains bovine TGF-β1-LAP; use qualified low-TGF lot or serum-free windows). Harvest 24–72 h post-stimulus (TGF-β1 secretion is slower than TNF/IL-6, peaks ~48 h in most MFB/DC models), spin ≥ 10,000 ×g, 5 min, 4°C, sup → acid-activate (even supernatant has LAP-clamped dimer from secreted LLC) → neutralise → read.
Golden rule: always run an NIBSC 89/742 mouse TGF-β1 spike-recovery pre-test on your specific matrix (serum vs. liver homogenate vs. lung homogenate) to confirm the acid-activation + ELISA recovers 85–115% — LTBP-rich matrices (lung, kidney) can be stickier than liver.
Where Mouse TGF-β1 Quantification Actually Carries the Paper (Beyond "Fibrosis Was Present")
- Hepatic Fibrosis: CCl₄, BDL, NASH — The HSC-Activation Clock
This is the definitive TGF-β1 model. Quiescent HSCs (vitamin-A-storing, desmin⁺) → injury (CCl₄, BDL, HFD+MCD) → TLR4/Kupffer activation → TGF-β1 from both Kupffer + activated HSC (autocrine) + recruited macrophages → paracrine on HSC → α-SMA↑, Col1a1/Col3a1↑, TIMP1↑, MMP inhibition → fibrous septum. The rigorous readout:
• Liver homogenate TGF-β1 (KTE7014, pg/mg, acid-activated total) — the profibrotic ligand mass
• p-Smad2 (Ser⁴⁶⁵) IHC/WB — the HSC-intrinsic signalling readout
• α-SMA IF, Hydroxyproline (μg collagen/mg), Sirius Red / Masson — the structural correlates
• Desmin / GFAP (quiescent HSC loss) + Ly6C⁺ monocyte recruitment
That linkage — TGF-β1 mass → Smad2 phosphorylation → α-SMA → collagen → septum — is what upgrades a "CCl₄ group looked worse" paper to a mechanism claim. If you're testing Alk5i (SB525334), anti-TGF-β1 mAb, or αvβ6 antagonist (STX-100 analog), the TGF-β1 drop + p-Smad2 drop + Hydroxyproline drop is the pharmacodynamic triad.
- Pulmonary Fibrosis: Bleomycin, Silica, COVID-Lung — The Alveolar Epithelial αvβ6 Axis
This is where TGF-β1 became a druggable franchise. Bleomycin i.t. → alveolar epithelial type II injury → integrin αvβ6 (upregulated on AECII + activated fibroblast) pulls LAP → TGF-β1 released → fibroblast-myofibroblast transformation → collagen deposition, honeycombing, DLCO↓. Key mouse fact: αvβ6-null mice are completely protected from bleomycin fibrosis (Munger 1999, Cell), proving the integrin-activation gate is non-redundant. Rigorous readout:
• Lung homogenate TGF-β1 (KTE7014, pg/mg, acid-activated) + BALF TGF-β1 (pg/mL)
• Ashcroft score (H&E), Hydroxyproline, α-SMA IF
• p-Smad2/3 IHC (nuclear in myofibroblasts = active signalling)
• αvβ6 IHC (AECII, fibroblast) + MMP-9 / TSP-1
If you're testing pirfenidone, nintedanib, anti-TGF-β1, or Alk5i, the lung TGF-β1 drop + Ashcroft + DLCO-equivalent (pleth) is the IO-for-IPF arc. COVID-lung post-viral fibrosis follows a near-identical AECII/αvβ6 pattern — TGF-β1 ELISA on post-COVID explants/humanized mouse lung is the "why the fibrosis persisted" variable.
- Renal Fibrosis: UUO, Diabetic Nephropathy, FSGS
Unilateral ureteral obstruction (UUO) → tubular epithelial TGF-β1 (autocrine, αvβ6 on TEC) + interstitial macrophage TGF-β1 → Smad2/3 in tubulointerstitium → α-SMA⁺ myofibroblasts, Col1/Col3, tubular atrophy. Renal homogenate/slice TGF-β1 (KTE7014, pg/mg, acid-activated) + PAS/trichrome (tubulointerstitial score) + α-SMA + KIM-1 (injury) + Sirius Red (collagen) is the nephrology triad. Diabetic db/db or STZ-kidney: TGF-β1 rises with hyperglycemia → PKC/AGE/RAS → TGF-β1 transcription + integrin αvβ6 up → same Smad2/3 → albuminuria + GBM thickening. If you're testing SGLT2i, RAS blockade, or Alk5i in nephroprotection, the kidney TGF-β1 drop + UAE + PAS score is the mechanism chain.
- Treg Differentiation & the TGF-β + IL-6 "See-Saw" (Th17 vs. pTreg)
This is the immunology Jekyll/Hyde. Naïve CD4⁺ under TGF-β1 + IL-2 → pTreg (Foxp3⁺, IL-10⁺, suppressive); under TGF-β1 + IL-6 + IL-23 → Th17 (RORγt⁺, IL-17A⁺, inflammatory). The in vivo correlate: oral gavage C. albicans or S. typhimurium → gut DC TGF-β1 + IL-6 → Th17; Treg adoptive transfer models need TGF-β1 in the microenvironment to stabilize Foxp3. Readout:
• MLN/lamina propria explant supernatant TGF-β1 (KTE7014, pg/mL, acid-activated)
• Foxp3⁺ % vs. RORγt⁺ % (flow)
• IL-10 (KTE7010) + IL-17A (KTE7012) — the cytokine correlates
If you're testing low-dose rapamycin (Treg-promoting) or RORγt inverse agonist, the TGF-β1 mass in the gut LP + Treg/Th17 ratio is the immunomodulatory receipt. Tgfb1⁺/⁻ chimeras or CD11c-cre Tgfb1 flox lose gut Treg homeostatic maintenance — the TGF-β1 ELISA drop + Foxp3% drop proves the locus.
- Cancer EMT & the "TGF-β Paradox" (Early Suppressor / Late Prometastatic)
This is the oncology hook. Early: TGF-β1 → Smad2/3 → p21/p15 → cytostasis, apoptosis (tumor-suppressive). Late: TGF-β1 → Snail/Slug/ZEB → EMT (E-cad↓, vimentin↑, N-cad↑, invasion) + TME remodeling (CAF activation, collagen cross-link, CXCL1/2/CCL2 recruitment, MDSC, Treg) + bone metastases (Smad → Runx2 → osteolytic). The "paradox" means TGF-β1 mass in the TME is context, not slogan:
• Tumor lysate/homogenate TGF-β1 (KTE7014, pg/mg, acid-activated) — correlates with Snail/Slug qPCR, E-cad/vimentin IF, p-Smad2 IHC
• 4T1 (breast → bone): TGF-β1 high in primary + metastatic niche → osteolytic lesions (RANKL/OPG ratio)
• Pan02/KPC (PDAC): TGF-β1 from CAF + tumor cells → desmoplastic stroma, gemcitabine resistance
If you're testing Alk5i + anti-PD-1 (e.g., SB525334 + pembrolizumab murine), the TME TGF-β1 drop + p-Smad2 drop + CD8⁺ re-infiltration + tumor growth is the mechanism arc (this combo is actively in clinical trials: Galunisertib + durvalumab).
- Scleroderma / Systemic Sclerosis (SSc) & Dermal Fibrosis
Bleomycin s.c. (daily 4 wks) or Tsk1/+ (tight-skin) mouse → dermal TGF-β1 up 3–10×, α-SMA⁺ myofibroblasts, collagen I/III, dermal thickness. Skin lysate TGF-β1 (KTE7014, pg/mg) + dermal thickness (H&E), hydroxyproline, α-SMA IF is the readout for anti-lox, anti-TGF-β1, or bosentan (endothelin-AR antagonist used off-label in SSc) screens.
A Minimal Protocol Skeleton You Can Paste Into Methods
- Serum/plasma: EDTA, wet ice, spin ≥ 2,000 ×g, 10 min, 4°C within 60 min, aliquot, snap -80°C, single thaw. Acid activation: dilute serum 1:10 in 1 N HCl, incubate on ice 10–15 min, neutralise 1:1 with 1 N NaOH / HEPES (pH ~7.4), keep cold.
- Tissue (liver, lung, kidney, skin, tumor): homogenize frozen tissue cold in PBS + 0.1% BSA + PI, spin 12,000 ×g 15 min, 4°C → sup → acid-activate sup per same HCl/neutralise protocol → BCA normalize to mg protein.
- Supernatants (HSC, CAF, Treg-polarising DC): serum-free 48 h harvest, spin ≥ 10,000 ×g, 5 min, 4°C, sup → acid-activate → neutralise.
- Warm kit reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate (KTE7014's 2-fold serial standard 31.25–2000 pg/mL, R² ≥ 0.99). Pre-test spike-recovery on your matrix (aim 85–115%) before committing the batch.
The Bottom Line
TGF-β1 is the 112-aa (~25 kDa dimer) cytokine that spends most of its extracellular life LAP-clamped in an SLC, then LTBP-tethered as an LLC in the matrix until integrin αvβ6/αvβ8 yanks the RGD or MMP/plasmin/TSP-1 cleaves the latency lasso — making it the master switch of fibrosis (liver, lung, kidney, skin), Treg differentiation (Foxp3, pTreg vs Th17 balance), EMT, and the cancer "early suppressor / late prometastatic" paradox. Because > 90% of TGF-β1 in any biological sample is LAP-bound and invisible without acid activation, it demands a mouse-specific sandwich ELISA whose capture/detection pair sees the mature dimer after dissociation. The EliKine™ Mouse TGF-β1 ELISA Kit — KTE7014 from Abbkine delivers that readout: pre-coated anti-mouse TGF-β1 capture (mature-dimer epitope) → biotin detection → EliKine™ SA–HRP → TMB → 450 nm → pg/mL interpolated, over a 31.25–2000 pg/mL calibrated range with LOD ~15 pg/mL (Intra CV < 8%, Inter CV < 10%, rejects TGF-β2/β3), in a ~3–4.5 h workflow (includes acid-activation prep) that scales from a CCl₄-liver timecourse to a bleomycin-lung UUO-kidney panel without chaining you to a p-Smad2 blot as your only "TGF-β proof."
Product Reference: KTE7014 – EliKine™ Mouse TGF-β1 ELISA Kit
Learn more and order: https://www.abbkine.com/product/elikine-mouse-tgf-%ce%b21-elisa-kit-kte7014/
(For Research Use Only; not for diagnostic procedures in humans.)





