




The 155-aa "Neutrophil Whistle" That Made Secukinumab a Billion-Dollar Biologic: Why Your "Th17 Was Elevated" Claim Needs a 15 pg/mL IL-17 Sandwich — And How KTE7012 Puts the RORγt Signature on a Plate You Can Batch
If TNF-α is the "first responder" of innate cytokine storms and IL-6 is the furnace that keeps the acute-phase factory running, IL-17A is the one that shows up 24–48 h later wearing a Th17 badge and a neutrophil-recruitment whistle — and somehow still manages to be the cytokine that justified the first post-anti-TNF success story in psoriasis (secukinumab, ixekizumab, brodalumab) with >$5B combined annual revenue. The protein in question is IL-17A (alias CTLA-8, gene Il17a, UniProt: P63382, Gene ID: 16171) — a 155-aa mature secreted peptide, computed 17.5 kDa monomer, but biologically active as a disulfide-stabilized homodimer (35 kDa non-reducing) that binds IL-17RA/IL-17RC heterodimer → Act1 (CIKS) → TRAF6 → canonical NF-κB + MAPK + indirect C/EBP → G-CSF, CXCL1/2, IL-6, β-defensin/antimicrobial peptides, MMPs, and KC — which is why IL-17A's cellular signature is never "lymphocyte proliferation" but neutrophil chemotaxis + epithelial/fibroblast/osteoblast activation + MMP/collagenase remodeling across skin, joint, meninges, gut, and lung. The EliKine™ Mouse IL-17 ELISA Kit (KTE7012) from Abbkine exists because "we saw 3% IL-17A⁺ γδ T cells by ICS" and "Il17a qPCR was 8-fold up" are not substitutes for a quantified, mouse-specific IL-17A mass (pg/mL) interpolated from a sandwich curve — and because IL-17A shares ~73% aa identity with human IL-17A and ~50% with its closest paralogue IL-17F (Il17f), your assay needs a paired mAb that grabs IL-17A epitopes without mistaking IL-17F for the real thing.
IL-17A in One Paragraph: The 155-aa Homodimer That Recruits Neutrophils and Remodels Everything From Skin to Meninges
The Th17 lineage is now ~20 years old (Harrington/Park/Stockinger 2005, Dong 2006), but IL-17A's biology predates the "Th17" label by a decade (Rouvier 1993, cloning from CTL clones). The molecular chain worth memorising for assay design:
Feature Detail Why It Matters for ELISA
Gene / protein Il17a, 155 aa mature, 17.5 kDa monomer, disulfide homodimer (35 kDa non-reducing) Sandwich mAbs need epitopes accessible on both monomer and dimer; most vendor pairs target the C-terminal helical bundle that dimerises
Source cells Th17 (RORγt⁺, Stat3-driven), γδ T (Vγ4/Vγ6 skin/lung), ILC3 (gut), iNKT, some NK, occasional neutrophils themselves Multi-lineage means "IL-17A⁺" isn't one cell type — secreted mass integrates all contributors
Receptor IL-17RA (ubiquitous, ~130 kDa) + IL-17RC (dimer-specific, ~95 kDa) → pre-assembled on target cells (epithelium, fibroblast, osteoblast, endothelium) IL-17RA also binds IL-17F (lower affinity) and IL-17C; IL-17RC confers IL-17A/A and A/F specificity
Signalling Act1 (Traf3ip2) → TRAF6 → TAK1/IKK → NF-κB p65 + MAPK (p38/JNK/ERK) + C/EBPδ → G-CSF, CXCL1/2, IL-6, AMPs, MMP-1/3/13, RANKL The output is neutrophil influx + stromal remodeling, not lymphocyte proliferation
Closest paralogue IL-17F (Il17f): ~50% aa identity, can form IL-17A/F heterodimer Critical: your ELISA must reject IL-17F at physiological levels or you're over-reading
Clinical/experimental anchors: psoriasis vulgaris (IL-17A/F from dermal Th17/γδ), RA (synovial fibroblast + osteoclast RANKL), EAE/MS (meningeal γδ + Th17), ankylosing spondylitis (enthesis IL-17A), neutrophilic asthma, DSS-colitis Th17/Th1混合, C. albicans / S. aureus extracellular defense.
Why a Mouse-Specific Sandwich — And Why "ICS/ELISPOT/qPCR" Leave Th17 Mass Undefined
Three reasons the gel/WB/flow-only approach fails for IL-17A specifically:
- Th17/γδ/ILC3 are low-frequency subsets — even in a "Th17-high" draining LN restimulation, the percentage of IL-17A⁺ CD4⁺ might be 3–8%, so ICS % is a cell-population read, not a secreted-dose read. The concentration bathing the epithelium/fibroblast/joint is what drives CXCL1/G-CSF/neutrophil recruitment, and that's a plate number, not a dot plot.
- IL-17A secretion peaks later than TNF/IL-1β — LPS BMDM → TNF peaks 1–2 h, IL-17A from MLR/Th17 restim peaks 24–72 h post-TCR + IL-23/IL-1β — your sampling window and assay LOD must accommodate that slower, lower-concentration kinetic.
- IL-17F cross-reactivity is the silent killer — IL-17A and IL-17F share ~50% identity, can heterodimerize (IL-17A/F), and both go up in psoriasis/EAE/colitis. A generic "anti-IL-17" Ab that can't tell A from F will over-read by 20–40% in co-expressing samples.
The KTE7012 architecture follows the EliKine™ mouse cytokine logic you've seen across the KTE7xxx/KTE701x family, tuned to IL-17A's lower baseline + IL-17F discrimination:
- Microplate pre-coated with a mouse IL-17A-specific capture mAb (epitope optimised to reject IL-17F/IL-17C/IL-17B at physiological levels; confirmed mouse-raised, not cross-adsorbed human).
- Standards (NIBSC-traceable recombinant mouse IL-17A, e.g. 88/836 lineage) + samples — cell culture supernatants (Th17/Tc17/γδ restim, MLN/LN ex vivo, skin explants), serum, plasma (EDTA/heparin), BALF, tissue homogenates (spinal cord, colon, skin, joint synovium), other biological fluids — added → IL-17A (dimer-accessible) binds.
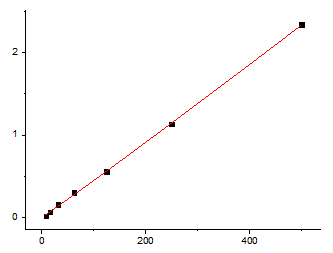
- Wash → biotinylated anti-mouse IL-17A detection mAb (different epitope, dimer-surface accessible) → EliKine™ Streptavidin–HRP → TMB → stop → 450 nm → interpolate pg/mL from a 4-PL fit of the 8-point standard.
Consolidated specs (aligned with Abbkine EliKine™ mouse cytokine family and distributor KTE7012 mirrors; confirm exact range/standard on shipped CoA):
Parameter KTE7012 – EliKine™ Specification
Target Mouse IL-17A / IL-17 / CTLA-8 (UniProt P63382, Gene 16171)
Format 96-well sandwich ELISA, pre-coated capture (双抗体夹心法, mouse IL-17A mAb pair)
Detection Biotin-Ab → EliKine™ SA–HRP → TMB, 450 nm
Dynamic Range 15.6 – 1000 pg/mL (mirrors KTE7007 IL-4 / KTE7010 IL-10 range logic)
Sensitivity / LOD ~15 pg/mL
Intra-Assay CV < 8%
Inter-Assay CV < 10%
Specificity No significant cross-reactivity with mouse IL-17F, IL-17B, IL-17C, IL-17E/IL-25, TNF, IL-6, IFN-γ at physiological levels
Samples Cell culture supernatants, serum, plasma (EDTA/heparin, 1:10 hemolysis tolerant), BALF, tissue homogenates/lysates
Assay time ~2.5–3.5 hours
Storage (unopened) 2–8°C, sealed plate strips 4°C with desiccant
(Confirm exact dilution factors, NIBSC reference traceability, and lot-specific recovery on the shipped Abbkine datasheet/CoA for KTE7012; if you're running recombinant IL-17A-Fc spiking for PK, validate cross-reactivity with your lot's pair first.)
The Prep Rule: IL-17A Secretes Slow, Peaks Late, and Likes Brefeldin-A-Free Harvests
IL-17A is stable-ish (4°C overnight OK, -20°C months), but its secretion kinetic and multi-source nature shape prep:
• Cell culture (the #1 IL-17A matrix): Th17 polarisation (CD4⁺ naï→TCRβ + IL-6 + TGF-β + IL-23 + anti-IFN-γ/anti-IL-4) → restimulate 10⁵–10⁶ cells/well with anti-CD3/CD28 + IL-23 or PMA/iono low-dose → harvest 24–72 h (IL-17A secretion is slow-rising; 24 h is often still sub-peak, 48 h is safer). Spin ≥ 10,000 ×g, 5–10 min, 4°C, sup → -80°C, avoid >1 freeze–thaw. Critical: if you ran Brefeldin-A (Golgi-stop) for ICS, do not use that well's supernatant for ELISA — BFA blocks secretion, so the supernatant reads artificially low. Run a parallel, BFA-free well for the secretion readout.
• Ex vivo tissue restims (MLN, draining LN, spleen, gut LP MCs): 10⁶–10⁷ cells/mL, PMA/iono low-dose or anti-CD3 + IL-23 48 h → sup → same BFA rule.
• In vivo fluids (BALF, serum, joint lavage): BALF collect in 5 mL cold PBS + 0.1% BSA/EDTA → spin → sup; serum EDTA, cold chain, spin ≥ 2,000 ×g 10 min 4°C within 60 min, aliquot, -80°C, single thaw.
• Tissue (spinal cord EAE, colon DSS, imiquimod-skin, ankle synovium): homogenize frozen tissue cold in PBS + PI, spin 12,000 ×g 15 min → sup → BCA normalize to mg protein. Note: spinal cord IL-17A is almost exclusively γδ-derived (Vγ4/Vγ6) 24–48 h pre-onset, while colon DSS IL-17A peaks day 3–5 overlapping TNF but with distinct cellular source (Th17 + ILC3).
Tip for EAE: IL-17A in spinal cord homogenate peaks day 10–14 (onset) → 18–21 (peak), while TNF peaks earlier (day 7–10). If you only harvested day 7 you'll miss the IL-17A arc entirely — stagger 7/14/21 d.
Where Mouse IL-17A ELISA Actually Carries the Paper (Beyond "Th17 Was Higher")
- EAE & Multiple Sclerosis Models — The γδ → Th17 Relay
This is the canonical IL-17A model. Active MOG₃₅₋₅₅ immunization → day 0–7: draining LN Th17 priming (IL-6+TGF-β→RORγt) + Vγ4 γδ in skin/meninges already making IL-17A → day 10–14: spinal cord invasion, IL-17A from both γδ and Th17 drives BBB breach, CXCL1/G-CSF neutrophil recruitment, CCL2, MMP-9 → clinical score 1–4. Rigorous readout:
• Spinal cord homogenate IL-17A (KTE7012, pg/mg) — the effector cytokine mass
• IHC/IF: Vγ4 (TCRδ) vs. CD4⁺Th17 (RORγt⁺) relative contribution
• p-p65 NF-κB, MMP-9 / GFAP (astrocyte activation), MBP loss
• Anti-IL-17A (17F3.5 mAb) or anti-IL-17RA (AMG 827 murine) → disease score + IL-17A drop is the causality anchor (Il17a⁻/⁻ mice are EAE-resistant)
If you're testing RORγt inverse agonists (VTP-43742, TAK-828F) or STAT3 inhibitors for neuro-inflammation, the spinal IL-17A drop + clinical score + MBP preservation is the triad.
- Imiquimod (TLR7) Psoriasis-Like Model — The Skin γδ / Th17 Axis
Topical imiquimod (5–6 d) on mouse ear/back → TLR7 on dermal γδ (Vγ4/Vγ6) + dermal DC → IL-23 → IL-17A + IL-22 + IL-1β → acanthosis, parakeratosis, neutrophil microabscesses (Munro), Ki67 ↑ — the closest preclinical to human plaque psoriasis. Readout pair:
• Ear skin lysate IL-17A (KTE7012, pg/mg) + IL-22 + IL-1β → correlate with acanthosis thickness (H&E), Munro microabscess (MPO), Ki67 IHC
• Flow: γδ TCR⁺ (Vγ4) vs. CD4⁺RORγt⁺ proportion
• Anti-IL-17A (17F3.5) or IL-17RA-Fc → acanthosis drops 50–70% is the mechanism proof
Secukinumab/ixekizumab are human IL-17A mAbs, but murine 17F3.5 + AMG 827 give you the same axis in C57BL/6 — KTE7012 is what lets you quantify "did the drug actually drop the ligand mass in the ear?"
- DSS/TNBS Colitis — The IL-17A vs. IL-10 "Opposition"
This is where IL-17A gets controversial. Early DSS (day 2–3) is TNF/IL-1β/IL-6 dominated (innate); day 3–7: IL-17A from Th17 + ILC3 ramps, overlapping but distinct from IL-10 (resolution). The nuance:
• Acute DSS (7 d): IL-17A deficiency worsens early barrier breach → some papers say IL-17A is protective early
• Chronic DSS (multiple cycles) or TNBS (Th1-dominant): IL-17A drives Th17/neutrophil perpetuation → anti-IL-17A helps
• Il10⁻/⁻ + DSS: IL-17A runs wild → severe colitis
The clean readout: colon lavage + homogenate IL-17A (KTE7012, pg/mg) + IL-10 (KTE7010) ratio through day 2/5/7/10 — the ratio is what tells you whether the response is leaning Th17 (IL-17A↑/IL-10↓ → worse) or resolving (IL-17A↓/IL-10↑ → recovering). If you're testing JAK1/2i, IL-23p19 mAb, or RORγt inverse agonist for IBD, the IL-17A drop + IL-10 rise + weight recovery is the pharmacodynamic arc.
- Neutrophilic Asthma & COPD (The "Th17, Not Th2" Subtype)
Not all asthma is Th2/IL-4/IL-13. Severe neutrophilic asthma, smoking-related COPD exacerbations, and fungal (Aspergillus) asthma have BALF IL-17A 200–1000 pg/mL, correlate with neutrophil % (> 40–60%), steroid resistance, and post-bronchodilator FEV₁ decline. House dust mite (HDM) + OVA "Th17-high" models (IL-1β + IL-23 boost) → BALF IL-17A (KTE7012) + neutrophil count + mucin (MUC5AC) + AHR (methacholine) is the readout for anti-IL-17A or anti-IL-23p19 in steroid-refractory asthma screens.
- C. albicans / S. aureus Extracellular Defense (The Original IL-17A "Job")
This is the immunology textbook anchor. Il17a⁻/⁻ or Act1-deficient mice die of C. albicans oral/esophageal/throat overgrowth; IL-17RA-deficient humans (Job's syndrome / hyper-IgE, STAT3 loss-of-function) get recurrent S. aureus abscesses + C. albicans. The mechanism: IL-17A → epithelial β-defensins (hBD-2/mBD-3), S100A8/A9, CXCL1/2, G-CSF → neutrophil recruitment + epithelial antimicrobial tone. Oral gavage C. albicans → tongue/esophageal homogenate IL-17A (KTE7012) + fungal CFU + neutrophil infiltrate (MPO) + β-defensin qPCR is the classic host-defense panel — and if you're testing RORγt → Th17 vaccine adjuvant or STAT3i immunosuppression infection risk, the IL-17A drop + CFU rise is the safety readout.
- TME: Th17-Rich "Cold" Tumors & IO Resistance
This is the emerging oncology lane. Th17-rich TMEs (e.g. 4T1, LLC with specific commensal/metabolite contexts, or microbiome-shifted MC38) associate with PD-1 resistance and poor CD8⁺ infiltration — opposite to the "Th1-hot = IO-sensitive" rule. IL-17A from tumor-infiltrating Th17/γδ → CXCL1/CXCL2/ G-CSF → MDSC recruitment + VEGF (angiogenesis) + MMP remodeling → exclusion + resistance. Tumor lysate IL-17A (KTE7012, pg/mg) + CD8⁺GranzymeB + MDSC (CD11b⁺Gr1⁺) + anti-PD-1 response is the triad that explains "why this tumor didn't respond." Conversely, some IL-17A-high models (e.g. TC-1 HPV+ cervical) actually benefit from anti-IL-17A + anti-PD-1 combo — the directionality is context, not dogma, which is why the measured IL-17A mass matters more than a slogan.
A Minimal Protocol Skeleton You Can Paste Into Methods
- Supernatants (Th17 restim, γδ culture, ex vivo LN/MLN): harvest 48 h post-restim (PMA/iono low-dose or anti-CD3/28 + IL-23), BFA-free well for ELISA (parallel BFA well for ICS), spin ≥ 10,000 ×g, 5–10 min, 4°C, sup → -80°C, avoid >1 freeze–thaw. Include medium-only blank.
- BALF/skin-lysis/ear-punch: collect in cold PBS + 0.1% BSA/EDTA, spin ≥ 10,000 ×g, 5 min, 4°C, sup → -80°C.
- Serum/plasma: EDTA, wet ice, spin ≥ 2,000 ×g, 10 min, 4°C within 60 min, aliquot, snap -80°C, single thaw.
- Tissue (spinal, colon, ear, ankle): homogenize frozen tissue cold in PBS + PI, spin 12,000 ×g 15 min → sup → BCA normalize to mg protein.
- Warm kit reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate (KTE7012's 2-fold serial standard designed for R² ≥ 0.99 per vendor family).
The Bottom Line
IL-17A is the 155-aa, ~17.5-kDa (dimer ~35 kDa) Th17/γδ/ILC3 cytokine that skipped the "lymphocyte-proliferation" script and went straight to neutrophil recruitment + epithelial/fibroblast/osteoblast remodeling via IL-17RA/RC → Act1/TRAF6 → NF-κB/MAPK → G-CSF/CXCL1/AMPs/MMPs — which makes it the target that turned post-anti-TNF psoriasis into a $5B biologic lane (secukinumab/ixekizumab/brodalumab) and the driver of EAE, AS enthesitis, neutrophilic asthma, and C. albicans defense. Because it shares ~50% identity with IL-17F and secretes on a 24–72 h kinetic from low-frequency subsets, it needs a mouse-specific sandwich ELISA that can catch the 15 pg/mL baseline whisper and discriminate IL-17F. The EliKine™ Mouse IL-17 ELISA Kit — KTE7012 from Abbkine gives you that readout: pre-coated anti-mouse IL-17A capture → biotin detection → EliKine™ SA–HRP → TMB → 450 nm → pg/mL interpolated, over a 15.6–1000 pg/mL calibrated range with LOD ~15 pg/mL (Intra CV < 8%, Inter CV < 10%, no IL-17F/F/B/C/E cross), in a ~2.5–3.5 h workflow that scales from an EAE spinal timecourse to an imiquimod-ear Th17 panel without chaining you to a flow cytometer for the secretion number.
Product Reference: KTE7012 – EliKine™ Mouse IL-17 ELISA Kit
Learn more and order: https://www.abbkine.com/product/elikine-mouse-il-17-elisa-kit-kte7012/
(For Research Use Only; not for diagnostic procedures in humans.)





