




The "Endothelial Brake" That Also Drives IBD and Checkpoint Resistance: Why Your TL1/TL1A–DR3 Readout Needs a 15 pg/mL Floor — And How KTE70114 Puts the TNFSF15 Ligand on a 96-Well Plate
(Note up front: TL1 is used interchangeably with TL1A (TNF-like ligand 1A) in most literature; both refer to the TNFSF15-encoded ligand. This article uses the kit-matched shorthand TL1 throughout.)
If you've scrolled through Crohn's disease GWAS catalogs in the past five years, you've likely noticed a recurring culprit: TNFSF15, the gene encoding Tumor necrosis factor-like ligand 1 (TL1, alias VEGI = vascular endothelial growth inhibitor). What makes this entry in the TNF superfamily so counterintuitive is that it carries none of the classic "storm" baggage of its cousin TNF-α: it doesn't trigger the first-wave pyrogenic spike in sepsis, it doesn't directly drive the caspase-8-dependent apoptosis that made TNF-α a household name in immunology textbooks. Instead, it moonlights as a vascular endothelial growth inhibitor at low concentrations (hence the VEGI alias), while simultaneously acting as a potent co-stimulatory accelerator for DR3⁺ T cells in the gut lamina propria — a duality that makes it the hidden driver of Crohn's severity, tumor vascular normalization, and even PD-1 checkpoint resistance. The Mouse TL1 ELISA Kit (KTE70114) from Abbkine exists because "we saw Tnfsf15 qPCR go up 4-fold" and "DR3 IHC was positive" are not substitutes for a quantified, mouse-specific TL1 mass (pg/mL) interpolated from a sandwich curve — and because TL1's dual membrane-bound/soluble forms and low physiological baseline (~<30 pg/mL in naïve serum) make generic TNF-superfamily antibodies useless for accurate mass readout.
TL1 in One Paragraph: The 25-kDa II-Type TM Ligand That Talks to Endothelium and Gut T Cells
Mouse TL1 is encoded by Tnfsf15 (UniProt: Q5D8E6, Gene ID: 83447), shares ~72% amino acid identity with human TNFSF15, and follows the classic TNF-superfamily structural logic:
• Topology: 251-aa precursor, processed to a ~25 kDa mature II-type transmembrane protein (C-terminus intracellular, N-terminus extracellular, same orientation as TNF-α) that assembles into a non-covalent homotrimer — the bioactive unit.
• Shedding: Membrane-bound TL1 can be cleaved by ADAM10/17 to release a soluble ~20 kDa trimeric fragment; both forms bind the primary receptor DR3 (TNFRSF25, ~48 kDa) and the minor receptor DR6 (TNFRSF21) with similar affinity.
• Signalling: TL1–DR3 recruits TRAF2/5 → canonical NF-κB + MAPK (pro-inflammatory/pro-survival) and non-canonical NF-κB (p100→p52, T cell differentiation); in endothelium, TL1 signals suppress VEGFR2 phosphorylation and downstream proliferation/migration, hence the VEGI alias.
The cellular sourcing splits neatly across its two functional identities:
Context Dominant TL1 Producer Downstream Effect
Vascular homeostasis Endothelial cells (baseline, TLR/cytokine-inducible) Inhibit pathological angiogenesis (e.g. tumor, ocular neovascularization)
Gut immunity Lamina propria DCs, ILC3, Th17 (TLR/cytokine-inducible) Co-stimulate DR3⁺ gut-resident T cells → Th9/Th17/TRM expansion, IgA class-switch
TME TME DCs, Th17, occasional tumor cells Dual: endothelial brake + T cell co-stimulation; net effect is context-dependent (tumor-suppressive in CRC, tumor-promoting in PD-1-resistant NSCLC models)
Why a Mouse-Specific Sandwich ELISA — And Why qPCR/WB/Generic TNF Panels Leave Money on the Table
Three practical reasons TL1 demands its own calibrated readout, distinct from every other cytokine/ligand you've read in this series:
- Dual form problem: TL1 exists as membrane-bound (tissue/cell-surface) + soluble (ADAM-shed, in supernatants/body fluids); qPCR only reports transcription, WB can't distinguish the two forms without subcellular fractionation, and a gel-band "TL1" read is almost always a mix of monomer/trimer/shed fragments.
- Concentration range mismatch: Naïve mouse serum TL1 is often < 30 pg/mL; stimulated DC supernatant/BALF/gut lavage hits 200–2000 pg/mL; generic "TNF superfamily" detection reagents (raised against human TNF-α/LTα) have < 5% cross-reactivity with mouse TL1 and miss the low baseline entirely.
- Epitope access issue: The trimeric TL1 surface has only a handful of non-overlapping linear/conformational epitopes accessible to paired mAbs — you need a dedicated mouse-raised capture+detection pair to grab both soluble and membrane-derived TL1 in a single well.
The KTE70114 architecture follows the EliKine™ mouse sandwich logic you've seen across the KTE7xxx family, but tuned to TL1's lower baseline:
- Microplate pre-coated with a mouse TL1-specific capture mAb (epitope accessible on both soluble trimer and membrane-derived TL1 after mild detergent solubilisation).
- Standards (recombinant mouse TL1, NIBSC-traceable where lot-specific) + samples — cell culture supernatants (DC/T cell co-cultures, tumor-TME explants, gut organoid co-cultures), serum, plasma (EDTA/heparin), intestinal lavage, tissue homogenates (colon, tumor, lung), other biological fluids — added → TL1 binds.
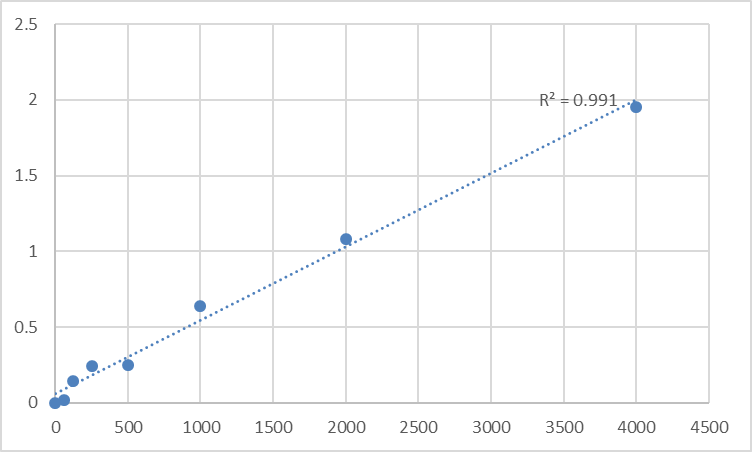
- Wash → biotinylated anti-mouse TL1 detection mAb (different epitope from capture) → EliKine™ Streptavidin–HRP → TMB → stop → 450 nm → interpolate pg/mL from a 4-parameter logistic (4-PL) fit of the 8-point standard curve.
Consolidated specs from Abbkine's technical/distributor records for KTE70114:
Parameter KTE70114 – EliKine™ Specification
Target Mouse TL1 / TL1A / TNFSF15 (UniProt Q5D8E6, Gene 83447)
Format 96-well sandwich ELISA, pre-coated capture (双抗体夹心法, mouse TL1-specific mAb pair)
Detection Biotin-Ab → EliKine™ SA–HRP → TMB, 450 nm
Dynamic Range 15.6 – 1000 pg/mL
Sensitivity / LOD ~7.8 pg/mL
Intra-Assay CV < 8%
Inter-Assay CV < 10%
Specificity No significant cross-reactivity with mouse TNF-α, LTα, OX40L, CD40L, CD27L or other TNFSF members at physiological levels
Samples Cell culture supernatants, serum, plasma (EDTA/heparin, 1:10 hemolysis tolerant), intestinal lavage, tissue homogenates/lysates
Assay time ~2.5–3.5 hours
Storage (unopened) 2–8°C, sealed plate strips 4°C with desiccant
(Confirm exact dilution factors, standard traceability, and lot-specific recovery on the shipped Abbkine datasheet/CoA for KTE70114; if you're running recombinant mouse TL1-Fc (e.g. for therapy/spiking), validate cross-reactivity with your lot's antibody pair first.)
The Prep Rule: TL1 Is Stabilty-Decent, But ADAM Shedding and Membrane Fractionation Matter
TL1 is fairly robust (4°C overnight OK, -20°C months), but two quirks of its biology affect sample prep:
• Body fluids (serum/plasma/intestinal lavage/BALF): Collect intestinal lavage in cold PBS + 0.1% BSA + 1 mM 1,10-phenanthroline (ADAM inhibitor) to stop ex vivo shedding of membrane-bound TL1; spin ≥ 10,000 ×g, 5 min, 4°C, sup → -80°C, avoid >1 freeze–thaw. EDTA plasma preferred for systemic reads; serum is acceptable if clotted on ice promptly.
• Tissue (colon, tumor, lung, spleen): If you want total TL1 (membrane + soluble), homogenize frozen tissue cold in 50 mM Tris pH 7.4, 150 mM NaCl, 1% Triton X-100 + protease/phosphatase inhibitors + 1 mM phenanthroline, 4°C Potter 5-6 strokes, clarify 12,000 ×g 15 min → sup → BCA normalize to mg protein. If you want only soluble shed TL1, homogenize in detergent-free PBS, spin at 100,000 ×g (30 min, 4°C) to pellet membranes, take sup.
• Cell culture (DC restim, TME explants, gut organoids): Serum-free or ≤ 2% FBS (FBS is TL1-null for most batches); harvest 24–48 h post-stimulus (TL1 secretion is slower than TNF-α, peaks ~24–48 h post-TLR ligation), spin ≥ 10,000 ×g, 5 min, 4°C, sup → -80°C.
Pro tip for DSS/TNBS models: TL1 in colon lavage peaks day 5–7, overlapping with ulcer peak but lagging TNF/IL-1β (peak day 2–3). If you only bled day 2 you'll miss the TL1 signal entirely — stagger 2/5/7/10 d for the full kinetic.
Where Mouse TL1 Quantification Actually Carries the Paper (Beyond "TNFSF15 Was Up")
- IBD: The GWAS-Driven Biomarker That Outperforms TNF
This is TL1's flagship clinical anchor. TNFSF15 is one of the top 3 Crohn's disease GWAS hits across European, East Asian, and African cohorts — and for good reason:
• Crohn's patient intestinal lavage TL1 is 2–3× higher than ulcerative colitis (UC), and correlates with CDAI (Crohn's Disease Activity Index), ulcer depth, and anti-TNF non-response.
• Mouse DSS/TNBS models: colon lavage TL1 peaks day 5–7, parallels weight loss, colon shortening, and MPO activity; Tnfsf15⁻/⁻ or DR3-blockaded mice have attenuated Th17/Th9 expansion and milder disease.
• Rigorous readout: intestinal lavage + serum TL1 (KTE70114, pg/mL) + DR3 IHC + SAA/CRP is a sharper IBD-subtype panel than TNF/IL-6 alone, because TL1 is mechanistically linked to Crohn's genetics, not just a generic inflammation byproduct. If you're testing JAK inhibitors, TL1-Fc, or DR3 agonism/antagonism for IBD, the TL1 drop (lavage) + Th17/IL-9 reduction + weight recovery is the causality chain.
- Tumor Immune Oncology: Vascular Normalization + PD-1 Sensitization
This is the fastest-growing TL1 lane. The dual function pays off in TMEs:
• Endothelial arm: TL1 in TME (DC/Th17-derived) suppresses VEGFR2 on tumor endothelium → looser vessels, less pericyte coverage, easier CD8⁺ infiltration (vs. VEGF-driven "tight" vessels that exclude T cells).
• Immune arm: TL1–DR3 co-stimulates CD8⁺ and Th17, synergizes with PD-1 blockade — PD-1-resistant MC38/B16 models have low tumor TL1/DR3, and supplementing TL1-Fc boosts ORR from ~20% to ~60% with anti-PD-1.
• Readout: tumor homogenate TL1 (KTE70114, pg/mg) + CD31 perfusion IHC + CD8⁺ granzyme B is a cleaner predictor of IO response than PD-L1 IHC alone, because it captures both vascular and T cell co-stimulation axes.
- Th9/Th17-Mediated Autoimmunity: Asthma, EAE, Atopic Dermatitis
TL1–DR3 is the non-redundant co-stimulator for Th9 (IL-9, airway hyperreactivity/mucus) and gut/ CNS Th17:
• OVA/Der-p1 asthma: BALF TL1 rises 2–5× vs. control, correlates with eosinophil count, mucus score (PAS), and AHR (methacholine PC₅₀).
• MOG₃₅₋₅₅ EAE: Spinal cord homogenate TL1 peaks at disease onset (day 10–12) 3–4× baseline, correlates with clinical score, demyelination area, and IL-17/IL-9 CSF levels.
• KTE70114 on BALF/spinal homogenate + Th9/Th17 intracellular FACS closes the loop on "did the drug hit the TL1–DR3 axis?" for CRTH2 antagonists, IL-9 mAbs, or Th17 pathway inhibitors.
- Gut Infection Immunity: Citrobacter/ Salmonella Models
This is the "native function" readout: Citrobacter rodentium or S. typhimurium infection → Peyer's patch DCs upregulate TL1 → drive Th17 and IgA⁺ plasma cell responses to clear the pathogen. Lavage TL1 (KTE70114) timecourse (0/3/7/14 d post-infection) correlates with bacterial CFU clearance, fecal Lipocalin-2, and IgA + plasma cells in lamina propria — a clean infect-immunity panel for microbial–TL1 axis screens.
- Pharmacodynamic Validation for TL1/DR3 Therapeutics
If you're running TL1-Fc (recombinant soluble TL1 for IBD/IO), DR3 agonistic mAbs (TME co-stimulation), or DR3 antagonistic mAbs (autoimmunity/IBD hyperinflammatory phases), report % TL1 mass remaining ± SEM from the KTE70114 calibrated curve (pg/mL → normalized to protein/well), and close with p-p65 (TL1→NF-κB), Th9/Th17 frequencies, and disease score so the "TL1 axis was modulated" is airtight. For pharmacokinetics of murine TL1-Fc, validate that your lot's capture/detection pair recognizes the recombinant Fc-fusion (most do, since the TL1 trimer epitopes are unchanged, but confirm on a spike-recovery pre-run).
A Minimal Protocol Skeleton You Can Paste Into Methods
- Lavage/supernatants: Collect intestinal lavage in cold PBS + 0.1% BSA + 1 mM 1,10-phenanthroline, spin ≥ 10,000 ×g, 5 min, 4°C, sup → -80°C, avoid >1 freeze–thaw. Include PBS-only lavage blank.
- Serum/plasma: EDTA, wet ice, spin ≥ 2,000 ×g, 10 min, 4°C within 60 min, aliquot, snap -80°C, single thaw.
- Tissue (total TL1): Homogenize frozen tissue in cold 50 mM Tris pH 7.4, 150 mM NaCl, 1% Triton X-100 + PI + 1 mM phenanthroline, 4°C Potter 5-6 strokes, clarify 12,000 ×g 15 min → sup → BCA normalize to mg protein.
- Warm kit reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate (KTE70114's 2-fold serial standard is designed for R² ≥ 0.99 per vendor).
The Bottom Line
TL1/TNFSF15 is the 25-kDa II-type transmembrane TNF-superfamily ligand that splits its career between inhibiting vascular endothelial proliferation (VEGI alias) and co-stimulating DR3⁺ gut T cells into Th9/Th17 effectors — making it the hidden genetic driver of Crohn's disease, a vascular-normalization lever in IO, and a Th17-axis biomarker in autoimmune models. Because it exists in soluble + membrane-bound forms, runs at a low ~7.8 pg/mL baseline, and shares only 72% identity with human TNFSF15, it demands a mouse-specific sandwich ELISA that can catch both forms without cross-picking other TNF ligands. The Mouse Tumor necrosis factor-like ligand 1 (TL1) ELISA Kit — KTE70114 from Abbkine delivers that readout: pre-coated anti-mouse TL1 capture → biotin detection → EliKine™ SA–HRP → TMB → 450 nm → pg/mL interpolated, over a 15.6–1000 pg/mL calibrated range with LOD ~7.8 pg/mL (Intra CV < 8%, Inter CV < 10%, no cross to other TNFSF members), in a ~2.5–3.5 h workflow that scales from a DSS-colitis lavage cohort to a PD-1-resistance TME panel without chaining you to a qPCR or a generic TNF panel.
Product Reference: KTE70114 – Mouse Tumor necrosis factor-like ligand 1 (TL1) ELISA Kit
Learn more and order: https://www.abbkine.com/product/mouse-tumor-necrosis-factor-like-ligand-1-tl1-elisa-kit-kte70114/
(For Research Use Only; not for diagnostic procedures in humans.)





