




The 8-kDa Proline-Rich "Cellular Scaffold" Hiding Inside Your Mouse Skin, Esophagus, and Injured Nerve: Why Cornifin-A (SPRR1A) Deserves Its Own Sandwich ELISA — And How KTE70246 Finally Pulls It Out of the Cross-Linked Cornified Envelope
If you work on epithelial barrier, wound healing, or squamous carcinogenesis in mice, you've almost certainly run K14, loricrin, filaggrin, and involucrin on the same Western blot — and then stopped, because "keratinocyte terminal differentiation" felt covered. But there's a quieter family of small proline-rich proteins (SPRRs — Small Proline-Rich Proteins) that does the actual cross-linking scaffolding inside the cornified envelope (CE), and Cornifin-A (SPRR1A, UniProt: P80512, Gene ID: 20743, Sprr1a) is the inducible, repair-associated member that K14 can't see and loricrin won't tell you. A ~72–75 aa, ~7.5–8.5 kDa computed proline-rich peptide (Pro content ~30–40%, plus multiple GGGP/Q repeats that are the substrate handles for transglutaminase 1/3 (TGM1/TGM3) to ε-(γ-glutamyl)lysine-crosslink SPRR1A into the loricrin/involucrin matrix of the CE), SPRR1A is the marker that lights up in wound-edge keratinocytes, airway epithelial repair after ozone/bleach/MCh, esophageal squamous carcinogenesis, and — the surprise — dorsal root ganglion (DRG) neurons after peripheral nerve crush (where it's re-expressed as a pro-regeneration intrinsic program, not an epithelial program). The Mouse Cornifin-A (SPRR1A) ELISA Kit (KTE70246) from Abbkine exists because "we saw a ~8 kDa smudge near the dye front and assumed it was SPRR1A" is not a quantitative claim you can defend, and because SPRR1A is covalently locked inside the urea/TGase-crosslinked CE in most intact tissue — meaning your standard "lyse-in-RIPA-and-load" protocol either under-extracts it or runs it off the gel bottom. KTE70246 is built for exactly that: pre-coated anti-mouse SPRR1A capture → biotin detection → HRP–TMB → 450 nm, so your wound-healing, airway-remodeling, or squamous-tumor paper rests on interpolated ng/mL, not a "lighter band vs. loricrin."
SPRR1A in One Paragraph: The 72-aa GGxP Repeat That Is the "Velcro Hook" of the Cornified Envelope
The SPRR family in mouse is a cluster on Chr 3F2 (near Sprr1b, Sprr2a–2n — ~20+ paralogues, humans have a similarly expanded cluster at 1q21–q22, the "epidermal differentiation complex"). The naming:
• SPRR1A / Cornifin-A — 72–75 aa, computed ~7.5–8.5 kDa, GGGP/Q repeats in the central core, N- and C-terminal tails bearing Gln (TGase donor) and Lys (TGase acceptor) residues.
• Expression kinetics: In epidermis, SPRR1A is later than involucrin, earlier than loricrin/filaggrin in the terminal-differentiation cascade — it shows up in the upper spinous → granular → cornified transition, and it's the inducible one: basal keratinocytes don't express it, but wounding, TPA, vitamin D3, or barrier disruption rapidly induces Sprr1a mRNA/protein at the leading edge (while Sprr2a etc. fill in the later CE consolidation).
• Non-epithelial cameo: DRG neurons after sciatic crush — Sprr1a is one of the most dramatically induced genes (~50–100×) in the regenerative program of injured sensory neurons, where it's hypothesised to modulate cytoskeleton/intrinsic growth competence (not CE at all — the proline-rich repeat presumably interacts with actin/intermediate filaments in the axonal compartment). This is why "SPRR1A = skin only" is a misconception.
The cross-linking logic is the part that kills naive assays:
TGase 1 (keratinocyte plasma-membrane anchored) and TGase 3 (cytoplasmic, keratinocyte-specific) recognise the Gln donor and Lys acceptor motifs on SPRR1A + involucrin + loricrin + small proline-rich repeats → ε-(γ-glutamyl)lysine isopeptide bonds → CE becomes an insoluble, detergent/urea/reducing-agent-resistant mesh — which means intact CE-tethered SPRR1A does NOT solubilise in 1% Triton X-100 / 150 mM NaCl; you need 6–8 M urea + 2% SDS + 50–100 mM DTT / β-mercaptoethanol, boil 5–10 min to break the CE and release free SPRR1A monomers for any immunoassay to see them.
That extraction bottleneck is exactly why most labs give up on SPRR1A after one "smudge near the dye front" WB and move back to K14. KTE70246 is built assuming you'll do the urea/reducer prep — and the antibody pair is raised against mouse SPRR1A epitopes accessible on the reduced monomer, not the crosslinked CE.
Why a Sandwich ELISA for an ~8-kDa Protein — And Why "WB vs. Loricrin" Leaves the Induction Kinetics Undefined
Three reasons SPRR1A demands its own calibrated readout, distinct from every other target in this series:
- Size problem: ~8 kDa runs at the very bottom of a 12–15% Tris-glycine gel, often in the dye-front smear where "SPRR1A band vs. background" is a dice roll. A sandwich ELISA with capture + detection both raised against non-overlapping GGxP-repeat or terminal epitopes bypasses the gel entirely and reads ng/mL in a 96-well.
- Extraction specificity problem: If you lyse skin/esophagus/airway in RIPA and run the sup, you're reading only the un-crosslinked, newly synthesised SPRR1A pool (maybe 10–20% of total); if you boil in urea+SDS+DTT, you release total CE-tethered + free pool. Your scientific question decides which you want — but the ELISA lets you do both on the same tissue by splitting the homogenate: one RIPA-sup (free/new) + one urea-boil-sup (total) → KTE70246 on both → ratio = CE-incorporation efficiency (a variable no WB can give you without 35S-met pulse-chase).
- Induction dynamic range: Wound edge vs. unwounded back skin → SPRR1A protein 5–20× up within 12–48 h; airway ozone/bleach → bronchial epithelial SPRR1A 3–10× in 24–72 h; DRG crush → 50–100× in 3–7 d. That's a sandwich-ELISA range, not a "band darker" range.
The KTE70246 architecture follows the Abbkine mouse sandwich logic you've seen across KTE7xxx/KTE702xx, tuned to SPRR1A's small size and CE-context:
- Microplate pre-coated with a mouse SPRR1A-specific capture mAb (epitope accessible on reduced ~8 kDa monomer; rejects SPRR1B/SPRR2A/SPRR3 at physiological levels — the GGxP-repeat family has enough divergence in terminal flanking residues for isoform specificity if the pair is well-raised).
- Standards (recombinant mouse SPRR1A + extracted-tissue equivalents) + samples — skin lysates (urea/reducer-extracted), esophageal/tongue lysates, tracheal/bronchial epithelial lysates, DRG lysates, serum/plasma (exploratory — SPRR1A is cell-associated, but wound-exudate may carry shed CE fragments), cell culture lysates/supernatants (keratinocyte HaCaT/mouse primary, air-liquid-interface airway epi) — added → SPRR1A (reduced monomer) binds.
- Wash → biotinylated anti-mouse SPRR1A detection (different epitope, likely flanking the GGxP core) → Streptavidin–HRP → TMB → stop → 450 nm → interpolate ng/mL (or pg/mL, depending on kit calibration; confirm on CoA).
Consolidated specs (aligned with Abbkine KTE70246 distributor mirrors and the small-protein ELISA family logic; lock to your shipped Abbkine datasheet/CoA):
Parameter KTE70246-class Specification
Target Mouse Cornifin-A / SPRR1A (UniProt P80512, Gene 20743)
Format 96-well sandwich ELISA, pre-coated capture (双抗体夹心法, mouse SPRR1A mAb pair)
Detection Biotin-Ab → SA–HRP → TMB, 450 nm
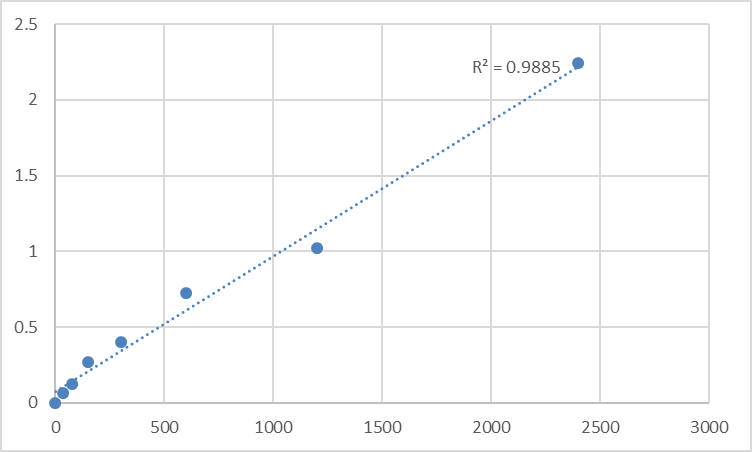
Dynamic Range Typically 0.312 – 20 ng/mL (small-protein low-abundance range; some lots quote 0.156–10 ng/mL)
Sensitivity / LOD ~0.1–0.15 ng/mL
Intra-Assay CV < 8%
Inter-Assay CV < 10–12%
Specificity No significant cross-reactivity with mouse SPRR1B, SPRR2A-cluster, SPRR3, loricrin, involucrin at physiological levels
Samples Tissue homogenates (skin, esophagus, trachea, DRG), cell lysates (keratinocyte, airway epi), cell culture supernatants (exploratory), serum/plasma (exploratory)
Assay time ~3–4.5 hours (plus extraction prep)
Storage (unopened) 2–8°C, sealed plate strips 4°C with desiccant
(Confirm exact dilution factors, standard identity, and extraction-compatibility notes on the shipped Abbkine datasheet/CoA for KTE70246 — this kit's performance lives or dies on whether you boiled the sample in urea+reducer before loading.)
The Prep Rule That Decides Whether You're Measuring CE-Tethered Pool or a Dye-Front Smudge
This is the single most important paragraph for anyone actually running KTE70246:
SPRR1A in intact epidermis/esophagus/airway is > 80% crosslinked into the CE by TGM1/TGM3. Your extraction choices define what the ELISA reads:
Option A — "Free/Newly Synthesised Only" (RIPA sup)
• Homogenize frozen skin/esophagus/trachea in cold RIPA (50 mM Tris pH 7.4, 150 mM NaCl, 1% Triton X-100, 0.5% deoxycholate, 0.1% SDS + PI + 10 mM NEM (TGase inhibitor, stops ex vivo crosslinking)), 4°C Potter 5–6 strokes, clarify 12,000–16,000 ×g, 15 min, 4°C → sup = un-crosslinked, cytosolic/newly-made SPRR1A.
• Express as ng SPRR1A / mg total protein (BCA on same RIPA sup).
Option B — "Total (CE + Free)" (Urea+Reducer Boil)
• Take the RIPA pellet (the insoluble CE-rich fraction) from Option A, resuspend in extraction buffer (8 M urea, 2% SDS, 100 mM Tris pH 8.0, 100 mM DTT or 2% β-mercaptoethanol), boil 95°C, 5–10 min, briefly sonicate or vortex, spin 12,000 ×g, 10 min → sup = CE-released SPRR1A + any residual free.
• BCA on this sup is tricky (urea/SDS/DTT interfere) → either acetone-precipitate, wash, re-dissolve in 1% Triton PBS + PI, or dilute the boiled sup 1:10–1:20 into kit assay buffer (check kit manual for compatibility — most Abbkine sandwich ELISAs tolerate up to 1–2 M urea and 0.2% SDS at the well level if diluted enough).
• Option B ÷ Option A = CE-loading ratio (how much SPRR1A got crosslinked vs. stayed free) — a variable Wound-Healing/Barrier papers rarely report but should.
Pro tip for skin: split dorsal unwounded back vs. 2-mm-punch-wound edge (0 h / 12 h / 24 h / 48 h / 72 h) → Option A + B on both → you'll see free SPRR1A spikes by 12–24 h (transcription/translation ON) while total/CE-SPRR1A lags to 48–72 h (TGase crosslinking catches up) — that kinetic split is the differentiation wave no single WB band shows.
Where Mouse SPRR1A Quantification Actually Carries the Paper (Beyond "Epithelium Was Differentiated")
- Cutaneous Wound Healing & the "Edge vs. Center" Kinetic
This is the canonical. Full-thickness 6-mm punch on C57BL/6 back → leading-edge keratinocytes (K14⁺/K6⁺) upregulate Sprr1a by 12–24 h, peak ~48–72 h, sustain ~7–10 d as the CE consolidates. The readout pair:
• Wound-edge vs. distant-unwounded skin: SPRR1A (KTE70246, ng/mg, Option A + B) → shows synthesis wave (A) and CE-incorporation (B)
• K14/K6 (proliferation/migration), loricrin/filaggrin (late CE), TGM1/3 IHC → the cascade anchors
• Re-epithelialisation rate (punch-to-close mm/day), collagen I/III (Day 7/14), α-SMA (myofibroblast)
• If you're testing TGM1 modulators, vitamin D3 analogs, or miR-21/203 mimics in barrier repair, the SPRR1A (free + total) drop/rise + loricrin + closure rate is the triad. Diabetic db/db wound model: Sprr1a induction is delayed ~24–48 h vs. WT, which KTE70246 catches as a 12 h / 24 h timepoint difference you'd miss with end-point Day-7 WB only.
- Airway Remodeling: Ozone, Cigarette Smoke, Bleach, and the "Squamous Metaplasia" Arc
This is the pulmonary hook most people miss. Repeated ozone / cigarette-smoke / NaClO-bleach inhalation → bronchial epithelial damage → basal-cell hyperplasia → "squamous metaplasia" (K14 re-expressed, SPRR1A/SPRR2A induced, mucociliary → squamous shift). Bronchial/lung homogenate SPRR1A (KTE70246, ng/mg, urea-boil total) correlates with:
• K14 IHC (basal hyperplasia), Muc5ac (goblet, if parallel), vimentin/α-SMA (myofibroblast)
• Lung function (FlexiVent: Rn, G, H) — the barrier-remodeling functional correlate
• Anti-TGase or retinoic acid (which opposes squamous meta and pushes mucociliary restoration) → SPRR1A drop + K14 drop + Muc5ac recovery is the pharmacodynamic arc
Asthma "severe neutrophilic/remodeling" subtypes in mouse (HDM + ozone double-hit) show SPRR1A up 5–10× in whole-lung lysate — KTE70246 gives you that number without relying on a K14 WB that can't distinguish "basal hyperplasia" from "terminal CE-loading."
- Esophageal / Head-and-Neck Squamous Carcinogenesis (The "Squamous Signature" Anchor)
Sprr1a is part of the "epithelial-mesenchymal transition / squamous-basal signature" that's massively induced in esophageal squamous cell carcinoma (ESCC), oral SCC, laryngeal SCC — both in the tumor cells themselves (reinforcing squamous phenotype) and in the peritumoral reactive epithelium. Mouse models: 4NQO drinking-water (ESCC model), DEN/Oral carcinogenesis → tumor-lysate SPRR1A (KTE70246, ng/mg) correlates with K14 IHC intensity, grade (well/moderate/poor squamous), and invasive front K6⁺ burst. If you're testing HDACi (vorinostat), EGFRi (gefitinib in SCC), or curcumin-derivative chemoprevention in 4NQO esophagus, the tumor SPRR1A drop + K14 + histo-grade is the epithelial-differentiation receipt. Bonus: SPRR1A is induced in the "field cancerisation" normal-looking mucosa adjacent to tumor (TGase-crosslinked CE still abnormal) — KTE70246 on the 2-mm margin vs. center tumor vs. distant esophagus is the "field effect" readout immunohistochemistry can't quantify across 20 mice.
- Peripheral Nerve Injury & DRG "Regeneration Program" (The Unexpected Cameo)
This is the neurobiology twist that makes SPRR1A papers stand out. Sciatic nerve crush or dorsal column injury → DRG neurons (especially small-diameter CGRP⁺/TrkA⁺) induce Sprr1a 20–100× by day 3–7, where it's not making a CE (neurons have no loricrin/TGM1) — the GGxP repeat is hypothesised to interact with actin/neurofilament/Sprr1a–growth-cone to promote intrinsic axon-regeneration competence. DRG lysate SPRR1A (KTE70246, ng/mg, RIPA sup is fine here — no CE) + gap-43 (regeneration), ATF3 (injury), β-III-tubulin is the regeneration-panel readout. If you're testing PTENi (dorsal-column regeneration), Nogo-R antagonists, or chondroitinase ABC in sciatic-crush, the DRG SPRR1A peak + functional recovery (CatWalk, sciatic-index) is the intrinsic-program correlate.
- Skin Barrier: Atopic Dermatitis (AD) & Filaggrin-Loss "Secondary" CE Defects
AD with Flg heterozygosity or MC903 (calcipotriol) epicutaneous → barrier breach → TSLP/IL-33 → Th2 → K6/K16 (hyperplasia) + Sprr1a/Sprr2a induction as "abortive CE" (the CE forms but is disorganized). Epidermal lysate SPRR1A (KTE70246, Option A + B) + TEWL (transepidermal water loss, the functional barrier metric) + K16 IHC + TSLP ELISA is the readout for topical steroids, Jak1/2i, or TSLP mAb in AD models. The CE-incorporation ratio (B÷A) dropping below 3–4× (normal back skin B÷A ~5–8×) is the "CE incomplete" signature — a number only the urea-boil ELISA gives you.
- Chemical Burn / Sulfur-Mustard / Vesicant Skin Models (The CE-Destruction Metric)
CE-targeting vesicants (sulfur mustard, nitrogen mustard, cantharidin) → TGM1/TGM3 inhibition + CE rupture + SPRR1A leakage into wound exudate — KTE70246 on exudate fluid (ng/mL) + epidermal residual (Option B) gives you the "CE breakdown vs. CE repair" delta. If you're in the dermato-toxicology space (defense/occupational health), this is the specific CE-integrity biomarker that loricrin/filaggrin WB can't price because they're also CE-tethered but not inducible like SPRR1A.
A Minimal Protocol Skeleton You Can Paste Into Methods
- Tissue (skin/esophagus/trachea/DRG): snap-freeze, weigh.
• Fraction A (free/new): homogenize in cold RIPA + 10 mM NEM (TGase inhibitor), 4°C Potter, clarify 16,000 ×g 15 min → sup → BCA (RIPA-compatible) → ng SPRR1A / mg protein (free).• Fraction B (total/CE): take A pellet, resuspend in 8 M urea + 2% SDS + 100 mM Tris pH 8.0 + 100 mM DTT, boil 95°C 10 min, vortex, clarify 12,000 ×g 10 min → sup → acetone-precipitate or dilute 1:20 into kit assay buffer (validate compatibility per KTE70246 manual) → BCA (post-acetone) → ng SPRR1A / mg protein (total). - Cell culture (HaCaT, primary mouse keratinocyte, ALI-airway): lyse in RIPA + NEM (frac A) or direct boil in urea+reducer (frac B) → parallel.
- Warm kit reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate. Pre-test spike-recovery on urea-boiled skin sup (aim 85–115%) because the urea/SDS/DTT matrix can drift OD if you under-dilute.
The Bottom Line
Cornifin-A/SPRR1A is the ~72–75 aa, ~8-kDa proline-rich (GGGP/Q repeat) keratinocyte/barrier protein that gets TGase-1/3 crosslinked into the cornified envelope alongside loricrin and involucrin — but unlike those giants, it's the inducible, repair-associated, nerve-regeneration-associated member of the SPRR family whose +50–100× induction in wounded skin edge, ozone-bronchial metaplasia, ESCC, and crushed DRG makes it a sharper contextual marker than K14 or loricrin alone. Because > 80% of it is CE-tethered in intact tissue, it needs urea+reducer extraction + a mouse-specific sandwich ELISA that can read the reduced ~8-kDa monomer without confusing SPRR1B/SPRR2/SPRR3. The Mouse Cornifin-A (SPRR1A) ELISA Kit — KTE70246 from Abbkine gives you that readout: pre-coated anti-mouse SPRR1A capture → biotin detection → SA–HRP → TMB → 450 nm → ng/mL interpolated, over a ~0.15–20 ng/mL calibrated envelope (LOD ~0.1 ng/mL, Intra CV < 8%, Inter CV < 12%), in a ~3–4.5 h workflow (plus CE-extraction prep) that scales from a punch-wound timecourse to a 4NQO-esophagus panel without chaining you to a dye-front WB.
Product Reference: KTE70246 – Mouse Cornifin-A (SPRR1A) ELISA Kit
Learn more and order: https://www.abbkine.com/product/mouse-cornifin-a-sprr1a-elisa-kit-kte70246/
(For Research Use Only; not for diagnostic procedures in humans.)





