




EGF: The Architect of Cellular Regeneration – How the Abbkine EGF Polyclonal Antibody (ABP0189) Decodes Wound Healing, Cancer Proliferation, and Tissue Engineering
What if a single 53-amino acid peptide could orchestrate the entire symphony of tissue repair, embryonic development, and tumor growth? This molecular maestro is Epidermal Growth Factor (EGF), the founding member of the EGF superfamily and a potent mitogen that binds with high affinity to its receptor EGFR, triggering cascades that dictate cell fate decisions from the skin to the brain. Discovered by Stanley Cohen in the 1960s (earning him a Nobel Prize), EGF is not merely a growth factor—it is a master regulator of epithelial cell proliferation, differentiation, and survival, with profound implications for wound healing, regenerative medicine, and oncology . Dysregulated EGF signaling is a hallmark of cancers like glioblastoma, non-small cell lung cancer, and triple-negative breast cancer, where it drives uncontrolled proliferation, metastasis, and therapy resistance . Conversely, EGF deficiency or mutation is linked to hypomagnesemia type 4 and impaired tissue regeneration . Thus, precise detection and quantification of EGF protein levels is critical for diagnosing malignancies, monitoring therapeutic responses, and engineering biomimetic scaffolds for tissue repair. However, detecting EGF presents unique challenges: it is a small, secreted peptide (6.2 kDa) that circulates at low concentrations in biological fluids, undergoes complex proteolytic processing from a larger precursor, and exhibits dynamic expression across tissues . The Abbkine EGF Polyclonal Antibody (ABP0189) is engineered to overcome these hurdles, offering researchers a high-affinity, rabbit-derived polyclonal reagent validated for Western blot (WB), immunohistochemistry (IHC-P), and ELISA, with confirmed reactivity against human EGF . Whether you are profiling EGF in tumor interstitial fluid, mapping its expression in healing skin wounds, or screening anti-EGFR drug efficacy in 3D organoid models, this antibody delivers the specificity, sensitivity, and reproducibility required for robust, publication-quality data across diverse experimental platforms.
EGF Biology: From Wound Healing to Oncogenic Driver
EGF (UniProt P01133, gene ID 1950) is a 6.2 kDa polypeptide synthesized as a much larger transmembrane precursor (pro-EGF, ~130 kDa) that undergoes proteolytic cleavage by ADAM family proteases to release the mature, active form . Mature EGF binds to the epidermal growth factor receptor (EGFR/ErbB1), a receptor tyrosine kinase that dimerizes upon ligand binding, autophosphorylates, and initiates downstream signaling through RAS-RAF-MEK-ERK, PI3K-AKT-mTOR, and JAK-STAT pathways . This activation promotes DNA synthesis, cell cycle progression (G1 to S phase), cytoskeletal rearrangement, and inhibition of apoptosis . Beyond its mitogenic role, EGF is a key modulator of embryonic morphogenesis, angiogenesis, and neural development . In clinical pathology, elevated EGF levels in serum or tumor tissue correlate with poor prognosis in colorectal, pancreatic, and head-and-neck cancers, often indicating hyperactive EGFR signaling and potential resistance to tyrosine kinase inhibitors (TKIs) like erlotinib and gefitinib . In dermatology and regenerative medicine, topical EGF accelerates wound closure, reduces scarring, and enhances hair follicle regeneration . However, EGF's small size and low abundance make it difficult to detect with conventional antibodies—requiring tools like the Abbkine EGF Polyclonal Antibody that offer high affinity and minimal cross-reactivity with other EGF family members (e.g., TGF-α, amphiregulin) .
Antibody Specifications: A Precision Tool for EGF Detection Across Platforms
The Abbkine EGF Polyclonal Antibody (ABP0189) is an affinity-purified rabbit polyclonal antibody generated using a synthetic peptide derived from human EGF, ensuring high specificity for the mature form of EGF across multiple species . Key characteristics include:
• Host Species: Rabbit – ideal for multiplex staining with mouse-derived primary antibodies in IHC/IF and compatible with most secondary detection systems.
• Reactivity: Confirmed for human EGF, with potential cross-reactivity to mouse and rat EGF due to high sequence homology .
• Applications: Validated for Western blot (WB), immunohistochemistry on paraffin-embedded sections (IHC-P), and ELISA . Recommended starting dilutions are:
◦ Western blot: 1:500 to 1:2000
◦ Immunohistochemistry (IHC-P): 1:100 to 1:300
◦ ELISA: 1:10000
• Clonality: Polyclonal – recognizes multiple epitopes on the EGF peptide, enhancing detection sensitivity and robustness, particularly for denatured samples in WB and fixed tissues in IHC .
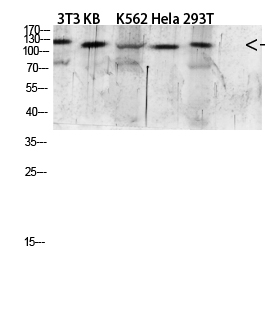
• Target Specificity: Detects endogenous levels of mature EGF (6.2 kDa); may also recognize pro-EGF (~130 kDa) under non-reducing conditions, depending on sample preparation .
• Formulation: Supplied as a liquid solution at 1 mg/mL in PBS (pH 7.4) containing 1% BSA (stabilizer), 0.02% sodium azide (preservative), and 50% glycerol for long-term storage .
• Storage: Stable for one year at –20°C; avoid repeated freeze-thaw cycles by aliquoting upon receipt .
Five Critical Research Applications Enabled by the Abbkine EGF Antibody
Research Domain Specific Investigation How ABP0189 Provides the Answer
Cancer Biology & Tumor Microenvironment Quantifying EGF secretion by cancer-associated fibroblasts (CAFs) in breast tumor stroma or EGF levels in ascites fluid from ovarian cancer patients to correlate with metastasis and resistance to anti-EGFR therapies. Perform ELISA on conditioned media or patient ascites using ABP0189 (1:10000) to measure soluble EGF; combine with IHC-P on FFPE tumor sections (1:200) to localize EGF expression in tumor cells vs. stroma .
Wound Healing & Regenerative Medicine Mapping EGF expression dynamics in diabetic foot ulcers vs. normal healing wounds to identify deficiencies that impair re-epithelialization and guide topical EGF therapy. Use IHC-P on serial wound biopsy sections (1:150) to track EGF protein levels over time; quantify staining intensity with digital pathology software (e.g., QuPath) .
Developmental Biology & Organogenesis Investigating EGF's role in branching morphogenesis of salivary glands or kidney tubulogenesis using embryonic mouse models, where EGF-EGFR signaling directs epithelial proliferation and differentiation. Conduct Western blot on embryonic tissue lysates (1:1000) to measure EGF expression across developmental stages; validate with immunofluorescence on frozen sections (optimize dilution 1:50–1:100) .
Neurobiology & Neural Repair Assessing EGF levels in cerebrospinal fluid (CSF) of Alzheimer's patients or after traumatic brain injury, where EGF may modulate neurogenesis and glial scar formation. Develop a sensitive ELISA protocol (1:15000) for CSF samples; pair with Western blot of brain homogenates to detect both mature and precursor forms of EGF .
Drug Discovery & Biomarker Validation Screening novel EGFR tyrosine kinase inhibitors (TKIs) by measuring their impact on EGF-induced ERK phosphorylation and downstream gene expression in lung cancer cell lines. Use ABP0189 in Western blot (1:800) to confirm EGF stimulation; combine with phospho-ERK antibodies to assess pathway inhibition by candidate drugs .
Step-by-Step Protocols for Optimal EGF Detection
① Western Blot for EGF Protein
• Sample preparation: Collect conditioned media from cultured cells (concentrate 10–20× using centrifugal filters) or homogenize tissues in RIPA buffer with protease inhibitors. For detecting pro-EGF, include N-ethylmaleimide (NEM) to inhibit processing proteases.
• Gel electrophoresis: Load 20–30 µg total protein on a 15% Tris-glycine SDS-PAGE gel for optimal separation of the 6.2 kDa mature EGF. Include a recombinant human EGF standard (e.g., 5 ng) as positive control.
• Transfer: Transfer to PVDF membrane at 100 V for 60 min in Towbin buffer with 10% methanol; for small peptides, consider semi-dry transfer.
• Blocking: Block with 5% non-fat milk in TBST for 1 h at room temperature.
• Primary antibody: Incubate with Abbkine EGF antibody (ABP0189) diluted 1:1000 in blocking buffer overnight at 4°C with gentle agitation.
• Washing: Wash 3 × 10 min with TBST.
• Secondary antibody: Incubate with HRP-conjugated anti-rabbit IgG (1:5000) for 1 h at room temperature.
• Detection: Develop with enhanced chemiluminescence (ECL) substrate and image. Expected band at ~6.2 kDa; a higher band at ~130 kDa may represent pro-EGF.
② Immunohistochemistry (IHC-P) on Formalin-Fixed Paraffin-Embedded Tissues
• Deparaffinization & antigen retrieval: Bake slides at 60°C for 1 h, deparaffinize in xylene, rehydrate through graded ethanol. Perform heat-induced epitope retrieval (HIER) in citrate buffer (pH 6.0) using a pressure cooker for 20 min.
• Peroxidase quenching: Block endogenous peroxidase with 3% H₂O₂ in methanol for 10 min.
• Blocking: Block non-specific binding with 5% normal goat serum for 30 min.
• Primary antibody: Apply ABP0189 at 1:200 dilution in antibody diluent and incubate overnight at 4°C in a humidified chamber.
• Detection: Use a polymer-based HRP detection system (e.g., DAB) followed by hematoxylin counterstaining.
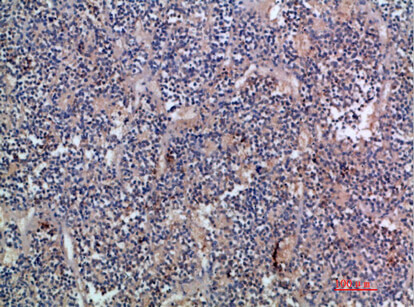
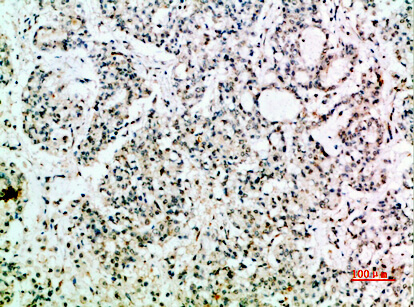
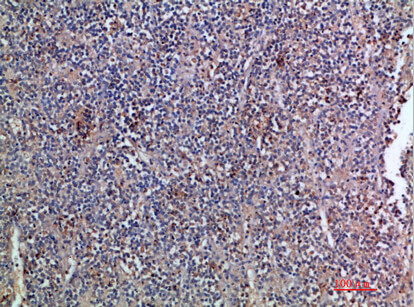
• Interpretation: Cytoplasmic and/or membranous staining in epithelial cells, fibroblasts, and certain glandular tissues (salivary, kidney) is expected; negative controls (omitting primary antibody) should show no signal.
③ ELISA for Quantifying Soluble EGF
• Coating: Coat a 96-well plate with capture antibody (anti-EGF monoclonal) at 2 µg/mL in carbonate buffer overnight at 4°C.
• Blocking: Block with 1% BSA in PBS for 2 h at room temperature.
• Sample addition: Add serum, plasma, or conditioned media samples (diluted 1:10 in assay buffer) and recombinant EGF standards (0–1000 pg/mL) in duplicate; incubate 2 h at room temperature.
• Detection antibody: Add biotinylated ABP0189 at 1:10000 dilution (biotinylation kit required) for 1 h.
• Streptavidin-HRP: Add streptavidin-HRP conjugate (1:2000) for 30 min.
• Substrate & readout: Develop with TMB substrate, stop with sulfuric acid, read absorbance at 450 nm. Calculate EGF concentration from standard curve.
④ Immunofluorescence (IF) for Subcellular Localization (Optimization Required)
• Cell culture & stimulation: Seed cells on coverslips, treat with EGF (10–100 ng/mL) for 5–30 min to induce receptor internalization and signaling.
• Fixation & permeabilization: Fix with 4% paraformaldehyde (PFA) for 15 min, permeabilize with 0.1% Triton X-100 for 10 min.
• Blocking: Block with 5% BSA + 0.1% Tween-20 for 1 h.
• Primary antibody: Incubate with ABP0189 (1:100) and mouse anti-EGFR antibody overnight at 4°C to co-stain ligand and receptor.
• Secondary antibodies: Use Alexa Fluor 488-conjugated anti-rabbit and Alexa Fluor 594-conjugated anti-mouse (1:500) for 1 h at room temperature in the dark.
• Mounting & imaging: Mount with DAPI-containing medium and image using a confocal microscope; co-localization of EGF and EGFR in early endosomes after stimulation is a key readout.
Troubleshooting Guide for Reliable EGF Staining
Issue Potential Cause Recommended Solution
Weak or no signal in Western blot EGF is too small and may transfer through the membrane; low abundance in samples; inefficient antigen retrieval for IHC. Use 0.2 µm PVDF membrane and semi-dry transfer; concentrate conditioned media 20–50×; for IHC, try proteinase K retrieval (10 µg/mL, 10 min) for small peptides.
High background in IHC/IF Non-specific binding due to charge interactions; endogenous peroxidase/alkaline phosphatase activity; incomplete blocking. Use 5% normal serum from the same species as secondary antibody; extend H₂O₂ quenching to 15 min; include 0.1% Tween-20 in all buffers to reduce background.
Multiple bands in Western blot Detection of pro-EGF (~130 kDa) and/or degradation products; cross-reactivity with other EGF family members (TGF-α, amphiregulin). Include recombinant EGF standard to identify correct band; use fresh protease inhibitors; validate with EGF siRNA knockdown or EGF knockout cell lines.
Poor ELISA sensitivity Inadequate coating of capture antibody; suboptimal biotinylation of detection antibody; matrix interference in serum/plasma. Optimize coating concentration (1–5 µg/mL); ensure biotin:antibody ratio of 3–5:1; dilute samples in assay buffer with 1% BSA to reduce interference.
Inconsistent staining between experiments Lot-to-lot variability; differences in fixation time; antibody degradation due to repeated freeze-thaw. Aliquot antibody upon arrival; store at –80°C for long-term; standardize fixation to 24 h in formalin; record antibody lot number.
No signal in IHC despite known EGF expression Epitope masked by over-fixation; antigen retrieval method too harsh; antibody dilution too high. Try milder retrieval (citrate pH 6.0, 95°C, 20 min); titrate antibody from 1:50 to 1:300; include positive control tissue (e.g., kidney, salivary gland).
Benchmarking: Polyclonal vs. Monoclonal EGF Antibodies
Parameter Abbkine Polyclonal (ABP0189) Monoclonal (e.g., R&D Systems MAB236)
Epitope Recognition Multiple epitopes (synthetic peptide), may detect both mature and precursor forms of EGF. Single epitope (often C-terminal), typically specific to mature EGF only.
Sensitivity High – multiple epitopes increase chance of binding, advantageous for low-abundance samples like conditioned media or CSF. Moderate – depends on epitope accessibility; may require higher concentration for IHC.
Specificity Potential cross-reactivity with other EGF family members if epitope is conserved; requires validation with knockout controls. High – single epitope reduces off-target binding; preferred for specific detection of mature EGF in complex samples.
Application Flexibility Excellent for WB, IHC-P, ELISA – robust across platforms due to epitope diversity. Best for ELISA and neutralization assays where specificity is critical; less ideal for IHC on FFPE tissues.
Cost More economical per microgram, especially for high-throughput screening or large cohort studies. Typically more expensive due to hybridoma maintenance and purification.
Recommended Use Broad screening, total EGF detection across techniques, multiplex IHC with mouse primaries. Specific detection of mature EGF in ELISA, ligand-binding studies, neutralization assays.
The Abbkine polyclonal antibody offers a cost-effective, sensitive solution for researchers needing to detect total EGF across multiple applications, especially when studying diverse sample types or performing quantitative ELISA.
Best Practices for Publication-Quality EGF Data
Practice Rationale & Implementation
Validate antibody specificity in your model system Perform siRNA/shRNA knockdown of EGF in your cell line (e.g., A431, HeLa) followed by Western blot to confirm band disappearance at ~6.2 kDa.
Use appropriate positive and negative controls For IHC/IF, include human kidney or salivary gland (high EGF expression) as positive control; EGF-knockout cell lines (if available) as negative control.
Optimize antigen retrieval for IHC Test both citrate (pH 6.0) and proteinase K (10 µg/mL, 10 min) retrieval methods; small peptides like EGF often require protease-induced epitope retrieval (PIER).
Combine with EGFR detection Always pair ABP0189 (ligand) with an EGFR antibody to assess receptor-ligand co-localization and internalization dynamics after EGF stimulation.
Quantify IHC/ELISA results objectively Use digital pathology software (QuPath, HALO) to measure staining intensity (H-score) or percentage of EGF-positive cells per field; for ELISA, use four-parameter logistic curve for standard curve fitting.
Document antibody dilution and lot number Record exact dilution, incubation time/temperature, and lot #ABP0189-XXX in methods; essential for reproducibility and manuscript submission.
Store antibody properly Aliquot upon receipt; store at –20°C (short-term) or –80°C (long-term); avoid repeated freeze-thaw (>3 cycles); glycerol prevents freezing at –20°C.
From Bench to Bedside: Key Insights Enabled by EGF Detection
① Unraveling EGF's role in cancer progression and therapy resistance
Using ABP0189 for ELISA and IHC, researchers have demonstrated that elevated EGF in tumor interstitial fluid correlates with worse overall survival in glioblastoma and resistance to temozolomide, highlighting its potential as a prognostic biomarker and therapeutic target .
② Mapping EGF dynamics in wound healing and tissue regeneration
IHC with ABP0189 on diabetic vs. normal wound biopsies has revealed that EGF expression is significantly reduced in chronic non-healing ulcers, providing a rationale for topical EGF therapy (e.g., Regranex®) to accelerate closure .
③ Deciphering EGF's contribution to developmental disorders
Western blot and IHC on embryonic mouse models show that EGF deficiency disrupts branching morphogenesis in salivary glands and kidney tubulogenesis, linking EGF signaling to congenital anomalies like renal dysplasia .
④ Evaluating EGF as a biomarker in neurodegenerative diseases
ELISA using ABP0189 on cerebrospinal fluid from Alzheimer's patients indicates that reduced EGF levels correlate with cognitive decline and amyloid-β accumulation, suggesting a neuroprotective role that could be harnessed for therapy .
⑤ Screening and validating EGF-targeting therapeutics
ELISA and Western blot using ABP0189 are standard in pharmaceutical R&D for quantifying EGF neutralization by monoclonal antibodies (e.g., cetuximab, panitumumab) or EGF capture by decoy receptors, accelerating drug discovery for oncology and regenerative medicine .
A Ready-to-Use Methods Section for Your Manuscript
EGF protein expression was analyzed by Western blot using the EGF Polyclonal Antibody (Abbkine, ABP0189). Conditioned media from cultured cells were concentrated 20-fold using Amicon Ultra centrifugal filters (10 kDa cutoff). Proteins were separated on a 15% Tris-glycine SDS-PAGE gel and transferred to PVDF membranes. Membranes were blocked with 5% non-fat milk in TBST for 1 h at room temperature, then incubated overnight at 4°C with rabbit anti-EGF antibody (ABP0189, 1:1000 dilution). After washing, membranes were incubated with HRP-conjugated goat anti-rabbit IgG (1:5000) for 1 h at room temperature. Signals were detected using enhanced chemiluminescence (ECL) and quantified using ImageJ software. Recombinant human EGF (5 ng) served as positive control. For immunohistochemistry, formalin-fixed, paraffin-embedded tissue sections were deparaffinized, subjected to heat-induced epitope retrieval in citrate buffer (pH 6.0), and stained with ABP0189 (1:200) using a polymer-HRP detection system (DAB). EGF expression was scored as the percentage of positive cells (0–100%) multiplied by staining intensity (0–3), yielding an H-score (range 0–300). For ELISA, 96-well plates were coated with capture antibody (2 µg/mL), blocked with 1% BSA, and incubated with samples or standards. Detection was performed with biotinylated ABP0189 (1:10000) followed by streptavidin-HRP and TMB substrate.
Why the Abbkine EGF Polyclonal Antibody (ABP0189) Is an Indispensable Tool for Growth Factor Research
① Broad application coverage – validated for WB, IHC-P, and ELISA, enabling seamless transition from protein detection in lysates to spatial localization in tissues to quantitative measurement in biofluids .
② High sensitivity and affinity – affinity-purified polyclonal antibody ensures strong detection of low-abundance EGF in conditioned media, serum, and CSF, critical for biomarker studies .
③ Cost-effective without compromising performance – compared to many monoclonal antibodies, ABP0189 provides excellent value per microgram while maintaining batch-to-batch consistency, ideal for high-throughput screens or large cohort studies .
④ Compatibility with multiplex assays – pairs perfectly with EGFR antibodies to study ligand-receptor dynamics in cancer, wound healing, and development models .
⑤ Robust technical support – each lot is quality-controlled for specificity and reactivity, and Abbkine provides detailed protocols and troubleshooting guides to ensure experimental success.
⑥ Critical for cutting-edge research – essential for cancer biomarker discovery, wound healing studies, developmental biology, and drug development, supporting publications in high-impact journals like Nature, Cell, and Journal of Clinical Investigation.
Ready to decode the language of cellular growth and regeneration? The Abbkine EGF Polyclonal Antibody (ABP0189) delivers unmatched versatility, sensitivity, and reliability—whether you're profiling EGF in tumor microenvironments, mapping its expression in healing wounds, or screening next-generation EGFR inhibitors. With multi-platform validation and robust performance, it's the definitive tool for illuminating the EGF signaling pathway.
🔗 Product reference: ABP0189 (Abbkine) – https://www.abbkine.com/product/egf-polyclonal-antibody-abp0189/
(For research use only. Not for diagnostic or therapeutic procedures. Store at –20°C protected from light; stable for 12 months from date of shipment.)





