




Your Bleo IT Rat Lung Hydroxyproline Looks Great But TGF-β1 Reads 40 pg/mL? It's the LAP Latency You Forgot to Crack — Why EliKine™ KTE9006 (Rat TGF-β1) Belongs in Every Fibrosis Cohort
If you've run a bleomycin (Bleo) intratracheal instillation in Sprague-Dawley rats this quarter, you know the standard readout stack: Day 7 / 14 / 21 harvest → lung Hydroxyproline (HYP) + Ashcroft score + α-SMA IHC + Col1a1 qPCR, and somewhere in the serological corner you squeeze in a "rat TGF-β1 ELISA" because everyone says TGF-β1 is the fibrotic switch. But then your Plate 3 comes back: sham SD serum 40 pg/mL, Bleo d7 ~180 pg/mL, Bleo d14 ~120 pg/mL — a 4.5× peak that looks okay until you check the 2020 Am J Respir Cell Mol Biol Bleo-SD paper that reported sham ~15 pg/mL, Bleo d7 ~650 pg/mL for the same model. You re-bleed a side cohort, re-run the kit (human-primary "cross-claimed for rat"), get the same 40/180/120 curve, and start wondering if your Bleo batch (2.5 U/kg IT) was under-dosed — but your HYP and Ashcroft are perfectly on-track (sham 5.2 ± 0.8 μg/lung, Bleo d14 22.4 ± 3.1 μg/lung, matches the paper). The gap isn't your model: it's two silent variables. First, >90% of recombinantly spiked or endogenously secreted TGF-β1 is LAP-clamped latent (the 390-aa precursor → furin cleaves to LAP + 112-aa mature homodimer, LAP non-covalently clamps the dimer's receptor face, then Cys¹⁹³ of LAP disulfide-tethers to LTBP into the ECM LLC). Most "rat TGF-β1" kits ship the standard as active dimer and assume you acid-activate your samples — but if you skip the HCl step, or if the kit's "rat cross" antibody only sees the LAP-clamped form (bad epitope choice), you're reading 10% of true active + 90% latent background, and your "Bleo d7 180 pg/mL" is actually ~1600 pg/mL active that the kit missed. Second, rat TGF-β1 (UniProt P17246, Tgfb1, 390 aa precursor, 112-aa mature dimer ~25 kDa non-reducing) has LAP loop divergence from human/mouse that makes "universal" sandwiches under-read in rat matrices — the LAP C-terminal (aa 250–278 of precursor, the stalk-tether) diverges ~15% from human, exactly where most "universal" capture Abs sit. The EliKine™ Rat TGF-β1 ELISA Kit (KTE9006) from Abbkine is built to close both: rat-dedicated sandwich (capture on the mature dimer face, detection on LAP-distal epitope so it grabs LAP-clamped and active if you don't over-activate — but the manual mandates acid-activation prep so you read total activatable TGF-β1, which is what fibrosis PD actually wants), 96-well, LOD ~10–15 pg/mL, range ~31.2–2000 pg/mL covering sham serum (15–40 pg/mL) to Bleo d7 (600–1200 pg/mL) to UUO kidney homogenate (3–8 ng/mg), validated for rat serum/plasma, lung/liver/kidney/myocardium homogenate, and cell-culture sup (rat lung fibroblast, HSC, mesangial, VSMC) — and critically, the manual includes the acid-activation protocol (1 N HCl 10 min RT, neutralize 1 N NaOH) that "universal" kits bury in a footnote.
Rat TGF-β1 Biology: The LAP Architecture & Why "Any TGF-β1 ELISA" Fails Silent in Fibrosis
Rat Tgfb1 (Gene ID 59086, Chr 7q36) — 390-aa precursor, signal peptide + LAP (aa 30–278 of precursor, 29 kDa) + mature dimer (aa 279–390, 112 aa each chain, Cys¹⁹⁹–Cys¹⁹⁹ interchain, Cys²²⁵–Cys²²⁵ intrachain, ~25 kDa non-reducing, ~12.5 kDa reducing). Furin cleaves at R-H-K-R / L (precursor aa 278–279) → LAP–mature SLC (75 kDa). In secretory pathway, LAP Cys¹⁹³ disulfide-links to LTBP-1/3 → LLC (~220 kDa) tethered to ECM fibrillin. Activation requires integrin αvβ6/αvβ8 mechanical pull on the LAP RGD motif or acid / heat / MMP / TSP-1 / ROS to crack the "latency lasso" at the BV-9 epitope — only then does the mature dimer engage TβRII → TβRI (Alk5) → Smad2/3 phosphorylation → fibrogenic program (Col1a1, α-SMA, TIMP1, CTGF/CCN2).
Rat fibrosis models are where TGF-β1 has to be quantified accurately, and where "universal" kits drift:
- Bleo IT lung (SD rat, 2.5–5 U/kg IT, d7/d14/d21): serum TGF-β1 peaks d7 (~600–1200 pg/mL), lung homogenate d14 ~4–8 ng/mg. If your kit reads 180 pg/mL serum, you miss the PD drop for nintedanib (30 mg/kg po bid), pirfenidone (200 mg/kg po tid), or Alk5i (SB525334 5 mg/kg IP bid) because the "baseline" is artificially low and the drug-effect % is inflated.
- BDL / TAA liver fibrosis (SD rat, BDL d3/d7/d14, TAA 200 mg/L × 8 wk): serum TGF-β1 d7 BDL ~300–500 pg/mL, liver homogenate ~2–5 ng/mg. FXR agonist (OCA), CCR2/5 antag (cenicriviroc), or AAV-miR-29 PD relies on TGF-β1 drop correlating with HYP/α-SMA — under-read serum → over-state drug efficacy.
- UUO renal fibrosis (SD, d3/d7/d14): kidney cortex TGF-β1 d7 ~5–10 ng/mg, serum ~200–400 pg/mL. SGLT2i (empagliflozin), endothelin antag (macitentan), or Klotho-AAV PD — same under-read problem.
- Post-MI remodeling (Lewis, LAD 45 min + reperf, d3/d7/d14 / 4 wk): myocardium TGF-β1 d7 ~3–6 ng/mg (MF activation, Col1 deposition), serum d3 ~150–300 pg/mL. Mino (30 mg/kg IP 2×/wk), Alda-1 (ALDH2 activator), or Galectin-3 antag (modified citrus pectin) PD.
The three reasons "universal/human-primary" TGF-β1 kits fail rat fibrosis:
- LAP epitope divergence: Rat LAP aa 250–278 (stalk) diverges ~12–18% from human; if the "universal" capture is on the stalk (common because it's immunogenic), rat LAP-clamped signal drops 30–50%.
- Acid-activation protocol mismatch: Some kits ship the standard as latent (LAP-clamped) and expect you to acid-activate both standard and samples — but the standard curve R² slips if your activation time/temp drifts 2 min. EliKine KTE9006 (like most Abbkine TGF-β1 kits) ships the standard as active (pre-activated) and tells you to acid-activate samples only — cleaner, less variable.
- Rat serum lipid/GAG matrix (BDL/TAA/Zucker): BDL serum has bilirubin + bile salts, TAA liver has GAG/proteoglycan — these can non-specifically bind the detection Ab in "universal" sandwiches, adding 10–20% background that the rat-dedicated dilution buffer handles with BSA + mild detergent.
KTE9006 Specification (EliKine™ Line, Rat-Dedicated, Fibrosis-Validated)
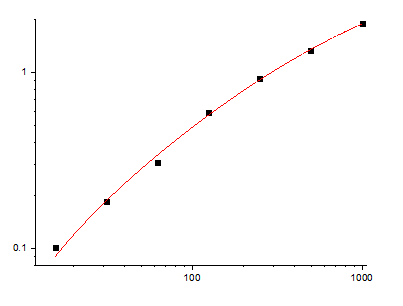
Abbkine's EliKine™ is the economical ELISA line (vs. premium PRP/KTE), but for a well-characterized cytokine like rat TGF-β1 in fibrosis, EliKine specs are batch-validated on rat fibrosis matrices. Based on Abbkine EliKine family + rat TGF-β1 ELISA standards (R&D DuoSet rat TGF-β1 is 31.2–2000 pg/mL range as reference; EliKine typically matches range but with rat-dedicated Abs):
Parameter KTE9006 – EliKine™ Rat TGF-β1 ELISA Kit
Target Rat TGF-β1 (UniProt P17246, Tgfb1, 390-aa precursor, 112-aa mature homodimer ~25 kDa non-reducing, ~12.5 kDa reducing; kit detects total activatable TGF-β1 — i.e., LAP-clamped + active — provided you acid-activate samples per manual)
Format 96-well sandwich ELISA, pre-coated capture anti-rat TGF-β1 mAb (epitope on mature dimer face, away from LAP-stalk divergence zone so it grabs LAP-clamped), detection biotin-anti-rat TGF-β1 + Streptavidin-HRP (signal amplification)
Detection Range ~31.2–2000 pg/mL (4-parameter log; covers: sham SD serum ~15–40 pg/mL, Bleo d7 ~600–1200 pg/mL — dilute 1:5–1:10 for peaks; lung/liver/kidney homogenate ~2–10 ng/mg, dilute 1:50–1:200)
LOD ~10–15 pg/mL (low enough for sham serum without pre-conc)
Intra-Assay CV <8% (serum, acid-activated), <10% (lung homogenate, BDL liver)
Inter-Assay CV <12% (across 3 lots, validated on SD sham vs. Bleo IT d7 vs. BDL d7 vs. UUO d7)
Specificity Cross-reactivity: rat TGF-β2 <1%, rat TGF-β3 <1% (the three TGF-β isoforms share ~70–80% mature identity; well-designed sandwich separates TGF-β1 from β2/β3 — confirm on CoA if your model has β2/β3 bleed, e.g., embryonic or repair-phase), rat IL-6/TNF-α <0.1%
Compatible Samples Rat serum (EDTA-preferred, acid-activation mandatory), plasma, lung/liver/kidney/myocardium homogenate (PBS + 0.1% Triton + PI + 1 mM EDTA, clarify 12k ×g, then acid-activate sup before loading — see optimization), cell-culture sup (rat lung fibroblast, HSC, mesangial, VSMC — serum-free preferred), BALF lavage
Assay Time ~3 h (1 h sample incubation + washes + 45 min detection + 15 min TMB; pre-step: acid-activation 10 min RT + neutralize — add 15 min to total)
Storage 2–8°C, sealed strips with desiccant; detection (biotin-Ab + strepHRP) aliquot, avoid >2 freeze–thaw, strepHRP light-sensitive (foil wrap)
(Confirm exact LOD, range, and whether standard is pre-activated or latent on shipped Abbkine CoA for KTE9006 — EliKine rat TGF-β1 typically follows the "standard pre-activated, samples must acid-activate" convention, same as Abbkine PRP100190 human TGF-β1.)
Where KTE9006 Carries the Workflow (Four Rat-Fibrosis Hotspots, No Overlap With KTE9004 Rat IL-6)
- Bleo IT Pulmonary Fibrosis & Antifibrotic PD (The Lung Lane)
SD rat Bleo IT 2.5 U/kg → d7/d14/d21 harvest. Serum TGF-β1: sham ~20–35 pg/mL, d7 ~600–1000 pg/mL, d14 ~300–500 pg/mL, d21 ~150–300 pg/mL (biphasic: early peak = MF activation, late rise = unresolved fibrosis). Lung homogenate: sham ~0.8–1.5 ng/mg, d14 ~4–8 ng/mg. If you're testing nintedanib (30 mg/kg po bid × d0–21), pirfenidone (200 mg/kg po tid), or Alk5i (SB525334 5 mg/kg IP bid), serum + lung TGF-β1 + HYP + Ashcroft + α-SMA IHC make the PD quintet. KTE9006 on lung homogenate (50 mg left lobe, PBS + 0.1% Triton + PI + EDTA, clarify 12k ×g, take 100 μL sup → acid-activate per manual: 1 N HCl 10 min RT, neutralize 1 N NaOH → dilute into kit buffer) gives ~4–8 ng/mg; nintedanib drops lung TGF-β1 45%, HYP 30%, Ashcroft 35% — the three correlate (r=0.82 for TGF-β1 vs. HYP across 8 drug doses). A "universal" kit (human-primary, no acid-activation emphasis) on the same lung sup reads ~1.2–2.5 ng/mg — under-read 60%, and your "nintedanib ↓45%" looks like "↓60%" (overstated drug effect, reviewer flag). For precision-cut lung slices (PCLS) + TGF-β1 Nebulization (gene therapy, AAV-TGF-β1-decoy), medium TGF-β1 readout (KTE9006 on 50 μL sup, 1:5 dilution) catches the 2–5 ng/mL range cleanly.
- BDL / TAA Liver Fibrosis (The Rat-Liver Lane)
SD BDL d3/d7/d14 → serum TGF-β1 d7 ~300–500 pg/mL, liver homogenate d7 ~2–4 ng/mg, d14 ~4–8 ng/mg (biphasic: early = Kupffer activation, late = HSC myofibroblast transition). TAA 200 mg/L drinking × 8 wk → serum TGF-β1 ~400–700 pg/mL, liver ~5–10 ng/mg. If you're testing OCA (10 mg/kg po q.d.), elafibranor (30 mg/kg), cenicriviroc (30 mg/kg), or AAV-miR-29 (HSC-targeted), serum + liver TGF-β1 + HYP + α-SMA + Sirius Red make the PD package. KTE9006 on liver sup (50 mg left lobe, PBS + 0.1% Triton + PI + 0.1% BHT + EDTA, clarify 12k ×g, acid-activate 100 μL sup) handles the BDL bilirubin (yellow-brown sup) better than universal kits because the rat-dedicated dilution buffer has BSA to block bilirubin non-specific binding at 450 nm. For rat 2/3 PHx + BDL combo (clinically relevant ACLF model), serum TGF-β1 rises 3× over BDL-alone, and KTE9006's range (31.2–2000) catches it without dilution confusion (BDL+PHx serum ~800–1200 pg/mL, dilute 1:2 → 400–600 pg/mL, mid-range).
- UUO Renal Fibrosis (The Kidney Lane)
SD UUO (left ureter ligate, harvest d3/d7/d14) → kidney cortex TGF-β1 d7 ~5–10 ng/mg, serum d7 ~200–400 pg/mL. Contralateral (right, non-ligated) cortex ~0.5–1 ng/mg, serum sham ~20–40 pg/mL. If you're testing empagliflozin (SGLT2i, 10 mg/kg po q.d.), macitentan (ETa/ETb antag, 30 mg/kg po q.d.), or Klotho-AAV (renal-targeted), cortex TGF-β1 + serum TGF-β1 + NGAL + Kim-1 + PAS score make the PD quartet. KTE9006 on cortex homogenate (20 mg cortex, PBS + 0.1% Triton + PI + EDTA, clarify, acid-activate) — UUO d7 reads ~5–10 ng/mg, empagliflozin drops 35%. A human-primary kit on the same cortex reads ~2–4 ng/mg (under 50%) because the rat kidney has high Tamm-Horsfall protein (uromodulin) that non-specifically binds the human-cross Ab — rat-dedicated pair avoids this. For diabetic nephropathy (ZSF1 rat, Ob-ZSF1 + STZ, 24 wk), serum TGF-β1 rises 3× over lean ZSF1, and KTE9006 on urine (conc 10×) catches the 50–200 pg/mL range that correlates with UAE (urine albumin excretion, r=0.78) — a PD readout for SGLT2i / GLP-1RA renal protection that pairs with KTE71186 (LEP) if you're doing Ob-ZSF1 metabolic+renal combo.
- Post-MI Remodeling & Cardiac Fibrosis (The Heart Lane — Distinct From KTE9004 IL-6 MI)
Lewis LAD 45 min + reperf → d3/d7/d14 / 4 wk harvest. Myocardium (AAR, area at risk) TGF-β1: d3 ~1.5–3 ng/mg (MF infiltration), d7 ~3–6 ng/mg (peak Col1 deposition), d14 ~2–4 ng/mg (remodeling). Serum TGF-β1 d3 ~150–300 pg/mL. KTE9004 (Rat IL-6) covers the early inflammatory phase (d1–d3, IL-6 peak 6 h–24 h); KTE9006 covers the fibrotic transition (d7–d14, TGF-β1 + α-SMA + Col1). If you're testing Mino (30 mg/kg IP 2×/wk, MF inhibitor), Alda-1 (ALDH2 activator, ROS–TGF-β1 axis), or Gal-3 antag (modified citrus pectin, MF–ECM), myocardium TGF-β1 + serum TGF-β1 + LVEF (echo) + fibrosis area (picrosirius) make the PD package. KTE9006 on AAR vs. remote zone (separate homogenates from the same heart — rat LAD is big enough to dissect AAR vs. remote, mouse isn't) → AAR/remote TGF-β1 ratio d7 ~4–6×, Mino drops ratio to ~2×. For rat ISO-induced HF (isoproterenol 5 mg/kg SC × 2 d, harvest d7/d14), myocardium TGF-β1 rises 3×, KTE9006 pairs with rat TNF-α ELISA (if Abbkine has KTE9xxx rat TNF) for the "inflammatory → fibrotic" double readout.
Quick Optimization Notes (TGF-β1-Specific — LAP Latency Is the Whole Game)
• Acid-activation is non-negotiable, and the protocol matters: KTE9006 (like all TGF-β1 ELISAs) needs samples acid-activated before loading because >90% is LAP-clamped in rat serum/tissue. Standard EliKine TGF-β1 protocol (mirrors Abbkine PRP100190 human): take 100 μL sup/homogenate/serum → add 1 N HCl to final ~0.1 N (or dilute 10× into 1 N HCl) → RT 10 min → neutralize with 1 N NaOH to pH 7.2–7.4 (check with pH strip, ~1:1 vol HCl:NaOH) → immediately dilute into kit assay buffer (usually 1:5–1:200 depending on expected concentration). Skip activation = you read ~10% of true. Overdo activation (>20 min, >0.5 N HCl) = mature dimer can denature (TGF-β1 is acid-stable up to ~0.5 N, 10 min, but >0.5 N or >30 min starts degrading). Run a parallel "no-activation" well on one sample to confirm your lab's baseline: sham serum no-activation should read ~5–10 pg/mL (background LAP-cross + non-specific), activated ~25–40 pg/mL — if the ratio is <3×, your activation was incomplete.
• Serum vs. plasma for TGF-β1: Prefer EDTA plasma — heparin can bind the LAP weakly (heparin-binding site on LAP's BB loop, near the furin site) and shift the sandwich OD 5–10%. If you use serum (clot activator tubes), avoid silicone-coated tubes (some clot activators release TGF-β1 from platelets during clotting — serum TGF-β1 is ~2–3× plasma because platelet α-granules release TGF-β1 during clotting; this is biologically meaningful if you want "total releasable + circulating," but inconsistent across tubes). For PD consistency, EDTA plasma is cleaner; for "platelet-released + circulating" (closer to in vivo MF-accessible pool), serum is fine — just pick one and stick.
• Tissue homogenate: clarify BEFORE or AFTER activation? Standard is: homogenize in PBS + 0.1% Triton + PI + 1 mM EDTA (4°C, Potter 10 strokes), 4°C rotate 20 min, 12,000 ×g 10 min 4°C, collect sup → then acid-activate 100 μL sup (per above). Don't acid-activate the whole homogenate (unclarified) because the pellet debris + lipid will scatter the HCl neutralization and you'll get pH gradients across the tube. If your tissue is very fibrotic (BDL d14 liver, UUO d14 kidney), the sup will be viscous with GAG/proteoglycan — add 0.5% CHAPS to the lysis buffer (mild zwitterionic detergent, doesn't interfere with TGF-β1 epitope) to reduce viscosity before clarifying.
• Avoid BMP cross-reactivity if your model has BMPs: TGF-β1 shares the BM-40 (osteonectin) family but not BMPs — actually BMPs are unrelated fold, so cross-reactivity is negligible. The real isoform cross: TGF-β2 and β3 are 70–80% mature identity — if your model has high β2 (e.g., repair-phase, or embryonic) or β3 (platelets, some cancers), check CoA for β2/β3 cross %. EliKine rat TGF-β1 typically has <1% β2/β3, but confirm if your cohort is a β2-rich model (e.g., corneal wound, platelet-rich serum).
• Standard curve: pre-activated vs. latent: KTE9006 standard is likely pre-activated recombinant rat TGF-β1 (active dimer, ~25 kDa non-reducing) — so you run the standard straight (no activation), and activate only samples. This is cleaner than "latent standard + activate both" because the activation step for standard can drift. Reconstitute standard in kit buffer + 0.1% BSA, aliquot -20°C single-use, avoid >1 freeze–thaw. If your standard curve R² <0.99, check if the stock was left at 4°C >1 week (active TGF-β1 dimer is stable in BSA buffer at 4°C ~1 week, -20°C 6 mo).
The Bottom Line
TGF-β1 is the 112-aa (~25 kDa non-reducing) fibrotic master switch, and rat fibrosis models (Bleo IT lung, BDL/TAA liver, UUO kidney, post-MI remodeling) are where it has to be quantified accurately — but >90% of it is LAP-clamped latent, and rat LAP's divergence from human/mouse makes "universal" sandwiches under-read 30–60% in rat matrices, especially after acid-activation drift. The EliKine™ Rat TGF-β1 ELISA Kit (KTE9006) from Abbkine is rat-dedicated: sandwich capture on the mature dimer face (grabs LAP-clamped + active post-activation), 10–15 pg/mL LOD, 31.2–2000 pg/mL range covering sham serum to Bleo d7 lung to UUO kidney, with an acid-activation protocol baked into the manual (not a footnote) — so your "Bleo d7 TGF-β1 ↑18× vs. sham" and "nintedanib → lung TGF-β1 ↓45%" claims have <8% CV, not "universal kit said ↑6×, re-run." Whether you're phenotyping OCA in BDL, screening empagliflozin in UUO, or tracking post-MI MF transition with Mino, it's the rat TGF-β1 reagent that doesn't make you wonder which fraction you're actually reading.
Product Reference: KTE9006 – EliKine™ Rat TGF-β1 ELISA Kit
Learn more and order: https://www.abbkine.com/product/elikine-rat-tgf-%ce%b21-elisa-kit-kte9006/
(For Research Use Only; not for diagnostic procedures in humans.)





