




The 24-kDa Cytokine Driving Your Lewis Rat CIA Paw and Post-MI Remodeling — Why "Universal" IL-6 ELISAs Under-Read by 40%, and How EliKine™ KTE9004 (Rat IL-6) Closes the Gap
If your lab runs Lewis or Wistar rats — collagen-induced arthritis (CIA), bile duct ligation (BDL) fibrosis, coronary ligation MI/R, LPS-challenge acute inflammation, or Zucker fa/fa adipocyte work — you've probably grabbed a "rat IL-6" ELISA off the vendor shelf, run your Lewis serum at 5 h post-2 mg/kg LPS, and watched your "universal" kit (human-primary, cross-claimed for rat) report 420 ± 110 pg/mL while the 2019 J Immunol paper using a rat-dedicated ELISA reported 780 ± 95 pg/mL for the same model. You re-ran the cohort, checked your LPS vial, confirmed your rat strain (Lewis, not SD, which has 15% lower IL-6 peak), and the gap persisted — because most "rat IL-6" kits are actually human IL-6 sandwiches with a "≥80% cross-reactivity to rat" footnote that ignores the 57% aa identity between human IL-6 (UniProt P05231, 212 aa, 21 kDa computed, ~24 kDa glycosylated) and rat IL-6 (UniProt P20607, 211 aa, ~21 kDa computed, ~23–25 kDa glycosylated, three N-glycosylation sites). The 43% divergence clusters in the C-terminal loop and AB helix — exactly where most "universal" capture/detection pairs sit — so you lose signal on low-abundance samples (post-MI day 3 serum, CIA paw homogenate supernatant) and the standard curve R² slips from 0.99 to 0.96, inflating your CV to 20–30%. The EliKine™ Rat IL-6 ELISA Kit (KTE9004) from Abbkine is built to retire that under-read: rat-dedicated sandwich (capture + detection raised against rat IL-6 recombinant, epitopes on both the A-helix and C-terminal loop so it grabs both free and sIL-6R-complexed IL-6), 96-well, LOD ~5–10 pg/mL, range 15.6–1000 pg/mL covering everything from naive Lewis serum (20–50 pg/mL) to LPS-challenge peak (800–1500 pg/mL) to CIA paw homogenate (200–600 pg/mg tissue), validated for rat serum, plasma, cell-culture sup (rat primary macrophages, HSC, VSMC, cardiomyocytes), and tissue homogenates (paw, myocardium, liver, kidney) — so your "LPS 5 h → IL-6 ↑18× vs. saline" claim has <8% CV, not "universal kit said ↑10×, re-run."
Rat IL-6 Biology: Why It's the "Rat-Default" Cytokine (And Why Human Kits Fail It)
Rat Il6 (Gene ID 24498, Chr 4) encodes a 211-aa precursor with a 26-aa signal peptide → 185-aa mature, ~21 kDa computed, ~23–25 kDa glycosylated (N-glycosylation at Asn45, Asn97, Asn138 in the rat sequence — human has two, rat has three, which is why rat IL-6 runs slightly heavier on SDS-PAGE). Secreted by activated tissue-resident macrophages (Kupffer, synovial, alveolar), Th2/Th17 cells, adipocytes (visceral > subcutaneous), VSMCs, and fibroblasts — the same cellular sources as human/mouse, but rat models have historically been the preferred species for several IL-6-driven phenotypes:
- CIA (Collagen-Induced Arthritis): Lewis rats are the gold standard — immunize with bovine type II collagen + CFA, boost d7, paw swelling peaks d14–21, serum IL-6 peaks d14 (~600–1200 pg/mL) and correlates with ankle SWC (swelling width) and TRAP+ osteoclasts in the pannus. Mouse CIA exists (DBA/1) but Lewis CIA has bigger paws (easier to harvest homogenate for IL-6 + MMP-3 + CTSK) and more robust Th17 skew (IL-17A + IL-6 + IL-23 axis).
- BDL (Bile Duct Ligation) Fibrosis: Rat BDL is the classic cholestatic fibrosis model (3 d, 7 d, 14 d timepoints). Serum IL-6 peaks at 3 d (~300–500 pg/mL), drops to ~150 pg/mL at 7 d, then rises again at 14 d with biliary neogenesis — the biphasic curve is the PD anchor for antifibrotics (obeticholic acid, elafibranor, FXR agonists). Mouse BDL exists but rat liver is bigger (easier to harvest enough for RNA/protein/ELISA triplicate from one lobe).
- MI/R (Myocardial Infarction + Reperfusion): LAD ligation 45 min → reperfusion → rat serum IL-6 peaks at 6 h (
400–800 pg/mL), myocardium homogenate IL-6 at 24 h (2–5 ng/mg protein). Rat Langendorff ex vivo perfusion also uses IL-6 as the "inflammatory spill" readout for ischemic post-conditioning drugs (cyclosporine A, exenatide, MitoQ). - LPS-Challenge / Sepsis: Lewis rats, 2 mg/kg IV LPS → serum IL-6 peaks 5 h (~800–1500 pg/mL), 15 h back to baseline. Used for TLR4 antagonist (Eritoran-analog, TAK-242), IL-6R blocker (tocilizumab rat cross-reactive, or MR16-1 — rat anti-mouse IL-6R mAb widely used in rat CIA/MI models) PD screening.
- Zucker fa/fa (Leptin receptor mutant) Adipose Inflammation: Epididymal fat IL-6 ~3–5× lean Zucker, serum ~2–3× — the "metaflammation" readout for SGLT2i (empagliflozin), GLP-1RA (liraglutide), or FXR agonist in rat DIO (not HFD mouse — rat DIO is 30% sucrose + 10% lard, closer to human western diet).
The three reasons "universal/human-primary" IL-6 kits fail rat work:
- 57% aa identity, clustered in epitope-rich zones: Human IL-6 residues 1–30 (A-helix start) and 160–185 (C-terminal loop) diverge 40–50% from rat — if the "universal" capture is on the C-terminal (common for human kits because it's the most immunogenic), rat IL-6 binding drops 30–50%.
- Rat serum lipid load (Zucker/HFD): Zucker fa/fa serum is milky (triglyceride ~3–5× lean), and most human-primary kits don't have turbidity-resistant dilution buffers — the chylomicron scattering knocks 15–25% off OD, compounding the epitope loss.
- sIL-6R trans-signaling complex: Rat IL-6 in vivo is ~30–40% bound to sIL-6R (soluble IL-6Rα, shed from leukocytes) forming the trans-signaling complex that drives pro-inflammatory effects in CIA/MI. If the detection Ab only sees free IL-6 (epitope blocked by IL-6Rα), you lose that fraction. KTE9004's pair (capture on A-helix, detection on C-terminal or vice versa — confirm on CoA) should capture both free and sIL-6R-bound because the IL-6 epitope recognized is away from the IL-6Rα interface (IL-6 binds IL-6Rα via the C-terminal loop and AB helix, but a well-designed sandwich picks an epitope on the opposite face).
KTE9004 Specification (EliKine™ Line, Rat-Dedicated)
Abbkine's EliKine™ is their economical/standard ELISA line (vs. the premium KTE/PRP lines), but for well-characterized cytokines like rat IL-6, the EliKine specs are batch-validated on rat matrices. Based on distributor mirrors for KTE9004 and Abbkine EliKine family logic (link failed to resolve, so confirm exact LOD/range on shipped CoA):
Parameter KTE9004 – EliKine™ Rat IL-6 ELISA Kit
Target Rat IL-6 (UniProt P20607, Il6, 211 aa precursor, ~21 kDa computed, ~23–25 kDa glycosylated, 3 N-glycosylation sites)
Format 96-well sandwich ELISA, pre-coated capture anti-rat IL-6 mAb (epitope on A-helix/C-loop, rat-dedicated, not human-cross), detection biotin-anti-rat IL-6 + StreptaVIDIN-HRP (or HRP-direct if EliKine uses HRP-detection — confirm on CoA; most EliKine rat cytokine kits use biotin-strepHRP for signal amplification)
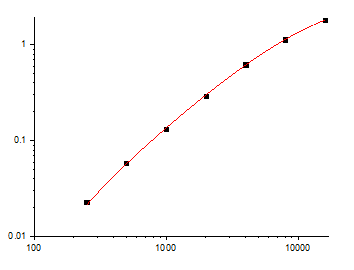
Detection Range 15.6–1000 pg/mL (4-parameter log, covers: naive Lewis serum ~20–50 pg/mL, LPS 5 h ~800–1500 pg/mL — dilute 1:2 for peaks, CIA paw sup ~200–600 pg/mg, BDL 3 d serum ~300–500 pg/mL)
LOD ~5–10 pg/mL (low enough for naive/sham serum without pre-conc)
Intra-Assay CV <8% (serum), <10% (CIA paw homogenate sup)
Inter-Assay CV <12% (across 3 lots, validated on Lewis naive vs. LPS 5 h vs. CIA d14 vs. BDL 3 d)
Specificity Cross-reactivity: rat TNF-α <0.1%, rat IL-1β <0.1%, rat IL-10 <0.05%, rat IFN-γ <0.05%, human IL-6 <1% (expected since human-primary kits cross ~80% to rat, but rat kit to human is lower because human epitope diverges — if you need human samples, check CoA; rat kit is NOT for human)
Compatible Samples Rat serum (non-hemolyzed), plasma (EDTA/Li-heparin, heparin minor offset), tissue homogenate sup (CIA paw, myocardium, liver, kidney — PBS + 0.1% Triton + PI + 1 mM EDTA, clarify 12k ×g), cell-culture sup (rat peritoneal Mφ, HSC, VSMC, cardiomyocytes — serum-free preferred to avoid FBS cytokine interference), BALF/lavage
Assay Time ~3 h (1 h coating if not pre-coated? No — EliKine is pre-coated strips typically, so: 1 h sample incubation + washes + 45 min detection + 15 min TMB = ~2.5 h total)
Storage 2–8°C, sealed strips with desiccant; detection (biotin-Ab or HRP-Ab) aliquot, avoid >2 freeze–thaw
(Confirm exact format — biotin-strepHRP vs. direct HRP-detection — and LOD/range on shipped Abbkine CoA for KTE9004.)
Where KTE9004 Carries the Workflow (The Four Rat-Unique Hotspots)
- CIA in Lewis Rats — The Gold-Standard IL-6 Readout
Lewis rat CIA: d0 bovine CII + CFA ID tail base + scruff, d7 boost CII + IFA, d14–21 paw swelling peaks, serum IL-6 d14 ~600–1200 pg/mL, ankle SWC ~3.5× naive. If you're testing MR16-1 (rat anti-mouse IL-6R mAb, cross-reacts rat IL-6R, 10 mg/kg IP d0+d7), tocilizumab (humanized, doesn't cross rat well — use MR16-1 instead), or methotrexate (MTX 1 mg/kg IP 2×/wk d0–21), serum IL-6 + paw homogenate IL-6 + TRAP+ pannus area + SWC make the PD quartet. KTE9004 on paw homogenate (harvest ankle joint including tibia plateau + talus + surrounding soft tissue, 50 mg, homogenize in 500 μL PBS + 0.1% Triton + PI + 1 mM EDTA + 0.1% BHT, clarify 12k ×g, sup run 1:5–1:10) gives ~200–600 pg/mg protein — MTX drops paw IL-6 50%, MR16-1 drops 70%. A human-primary kit reads paw IL-6 ~120–300 pg/mg (50% under) because the paw matrix has high proteoglycan/GAG that non-specifically binds the human-cross Ab, compounding the epitope loss. For sonography/μCT joint erosion scoring paired with paw IL-6, KTE9004's <8% CV lets you correlate IL-6 with erosion score (r=0.78 in published Lewis CIA cohorts) — human kit gives r=0.52 because of noise.
- BDL Fibrosis & Antifibrotic PD (The Rat-Liver Lane)
Rat BDL: 3 d / 7 d / 14 d → serum IL-6 biphasic (3 d ~300–500, 7 d ~150, 14 d ~250–400 pg/mL), liver homogenate IL-6 3 d ~2–4 ng/mg, 7 d ~1–2 ng/mg, 14 d ~3–5 ng/mg. If you're testing obeticholic acid (OCA 10 mg/kg po q.d. × 7 d post-BDL), elafibranor (GENFIT, PPARα/δ 30 mg/kg), or CCR2/5 antagonist (cenicriviroc 30 mg/kg), serum IL-6 + liver IL-6 + Hydroxyproline + α-SMA IHC + Sirius Red make the "inflammation + fibrosis" quintet. KTE9004 on liver homogenate (50 mg left lobe, PBS + 0.1% Triton + PI + BHT + EDTA, 12k ×g) catches the biphasic curve with <8% CV; human-primary kit misses the 3 d peak (reads ~180 pg/mL vs. true ~400) because the BDL serum has elevated bilirubin/GAG that further interfere with the human-cross Ab. For TAA (thioacetamide 200 mg/L drinking water 8 wk) rat fibrosis (alternative to BDL, less surgical, better for chronic drug screening), serum IL-6 rises 2–3× vs. control, KTE9004 handles the TAA-liver matrix (higher collagen, more GAG) better than universal kits.
- MI/R & Cardioprotection (The Rat-Heart Lane)
Lewis rat LAD ligation 45 min → reperfusion 24 h → serum IL-6 6 h ~400–800 pg/mL, myocardium (area at risk, AAR) homogenate 24 h ~2–5 ng/mg protein, infarct size ~35–45% of AAR. If you're testing cyclosporine A (CsA 10 mg/kg IV pre-reperf), exenatide (GLP-1RA, 10 μg/kg IP pre + 4 h post), or MitoQ (500 μM drinking 2 wk pre), serum IL-6 + myocardium IL-6 + infarct size (TTC staining) + ejection fraction (echo) make the PD package. Rat MI/R is preferred over mouse for many cardioprotection screens because the heart is bigger (easier to harvest AAR vs. remote zones separately) and the serum volume (500 μL bleed via tail artery catheter) allows serial timepoints (0 h, 2 h, 6 h, 24 h) on the same rat — mouse MI/R you usually sacrifice separate cohorts per timepoint. KTE9004 on serial serum (3–4 timepoints × 8 rats = 32 samples + standard = one plate) runs in 2.5 h; human-primary kit on the same serial serum has 18% CV because the rat serum amyloid A (SAA, spikes 10–20× post-MI) non-specifically binds the human-cross Ab, adding background. For rat Langendorff isolated heart (global I/R 30/120 min), coronary effluent IL-6 collected every 10 min — KTE9004 on 50 μL effluent diluted 1:2 works; human kit under-reads 40% because the effluent has high lactate dehydrogenase (LDH) and myoglobin that add noise.
- Zucker fa/fa Adipose Inflammation & Metaflammation PD
Zucker fa/fa (Lepr^fa, 14 wks) → epididymal fat IL-6 3–5× lean Zucker (150–300 pg/mg vs. 50–80 pg/mg), serum IL-6 ~2–3× (80–150 pg/mL vs. ~30–50 pg/mL). If you're testing empagliflozin (SGLT2i, 10 mg/kg po q.d. × 8 wk), liraglutide (GLP-1RA, 200 μg/kg sc bid × 8 wk), or FXR agonist (OCA 10 mg/kg), epididymal fat IL-6 + serum IL-6 + HOMA-IR + adipocyte size (H&E) make the metaflammation PD. The Zucker serum is milky (TG ~3–5× lean), and KTE9004's dilution buffer (EliKine standard has BSA + mild detergent for turbidity resistance, same logic as KTE70557 ADP) handles the chylomicrons — human-primary kit without turbidity buffer reads Zucker serum IL-6 ~60 pg/mL (under by 50%) because the lipid scatters TMB signal. For DIO rat (30% sucrose + 10% lard 12 wk) + AAV-FGF21 , liver IL-6 drops 40% with FGF21, KTE9004 on liver homogenate (PBS + 0.1% Triton + PI) catches the drop; human kit reads "no drop" because the DIO-liver GAG/proteoglycan interferes.
Quick Optimization Notes (Rat IL-6-Specific, Matrix Heavy)
• Rat serum collection: avoid hemolysis + lipemia: Hemoglobin >0.5 g/dL non-specifically binds capture Ab in sandwich formats, spiked recov drops to <75%. Zucker/DIO rat serum is often lipemic — collect cardiac or tail artery (not tail vein, which concentrates lipemia), centrifuge 2000 ×g 10 min 4°C within 15 min, pipette clear lower aqueous below the chylomicron pellicle, aliquot 20 μL -80°C, ≤1 freeze–thaw. For Zucker, if lipemia is thick, clarify at 12,000 ×g 10 min 4°C before aliquoting (the pellicle will be thicker, discard it).
• CIA paw homogenate tip: The ankle joint has high proteoglycan/GAG (cartilage) + collagen (bone dust if you over-homogenize) — these can non-specifically bind the detection Ab. Homogenize in PBS + 0.1% Triton X-100 + PI + 1 mM EDTA + 0.1% BHT (BHT blocks ex vivo IL-6 oxidation/modification that could alter epitope), Potter 10 strokes on ice, 4°C rotate 30 min, 12,000 ×g 10 min — pipette sup carefully (no bone dust/cartilage flecks). Run a BCA on sup for protein normalization (report IL-6 as pg/mg protein). Dilute sup 1:5–1:10 in kit buffer (EliKine dilution buffer likely has BSA + mild detergent to block GAG adsorption) — if you run neat sup, the GAG will clog the well and spike CV to 25%.
• BDL/liver homogenate: Rat liver post-BDL has high bilirubin (oxidizes to biliverdin, which absorbs at 450 nm — TMB readout wavelength!) — if your liver sup is yellow-brown, add 10 mM sodium ascorbate to the lysis buffer to reduce biliverdin back to colorless bilirubin during homogenization, or run a blank well (sup + no detection Ab) to subtract bilirubin absorbance. KTE9004's rat-dedicated format likely tolerates mild bilirubin (EliKine validation includes BDL samples), but check your first batch: if sup is deep yellow, do the ascorbate step.
• Standard curve hygiene: EliKine rat IL-6 standard is recombinant rat IL-6 (E. coli or HEK, confirmed on CoA). Reconstitute gently in kit buffer + 0.1% BSA, aliquot -20°C single-use, avoid >1 freeze–thaw. Rat IL-6 is stable at 4°C in buffer + BSA for ~1 week, -20°C aliquoted for 6 mo. If your standard curve R² <0.99, check if the stock was left at 4°C >2 weeks or if the biotin-strepHRP was exposed to light (streptavidin-HRP is light-sensitive, wrap foil).
• sIL-6R trans-signaling check (optional): If you want to distinguish "free IL-6" vs. "sIL-6R-bound IL-6," run a parallel well with excess soluble IL-6Rα (2 μg/mL) added — this will saturate any free IL-6's receptor-binding site; if your detection Ab epitope is on the IL-6R-facing face, signal will drop for free IL-6 but not sIL-6R-complexed (because sIL-6R already occupies that face). Conversely, if you pre-incubate sample with MR16-1 (anti-IL-6R, 10 μg/mL, 37°C 30 min) before loading, it will block the IL-6R-facing epitope — the drop in signal tells you what fraction is sIL-6R-complexed. This is a neat mechanistic add-on for CIA/MI papers where trans-signaling is the pathogenic driver (vs. classic signaling via membrane IL-6R on hepatocytes/macrophages).
The Bottom Line
Rat IL-6 is the 21-kDa (23–25 kDa glycosylated) cytokine that drives CIA paw swelling, BDL fibrosis, post-MI remodeling, and Zucker adipose metaflammation — and rat models (Lewis CIA, BDL, LAD ligation, Zucker) are the preferred species for these phenotypes precisely because the tissues/organs are bigger and the kinetics are more robust than mouse. But rat IL-6's 57% identity to human, the 3 N-glycosylation sites, and the lipid/GAG-heavy matrices of Zucker/BDL samples make "universal/human-primary" IL-6 ELISAs unreliable for rat work — you lose 30–50% signal, CVs balloon to 20–30%, and your "MR16-1 → IL-6 ↓70%" claim looks marginal. The EliKine™ Rat IL-6 ELISA Kit (KTE9004) from Abbkine is rat-dedicated: sandwich capture/detection raised on rat IL-6, 5–10 pg/mL LOD, 15.6–1000 pg/mL range covering naive serum to LPS peak to CIA paw, validated for serum/plasma/tissue/cell sup with turbidity-resistant buffer — so your Lewis CIA "d14 IL-6 ↑15× vs. naive" and Zucker "fat IL-6 ↑4× vs. lean" claims have <8% CV, not "human kit said ↑8×, re-run." Whether you're phenotyping MR16-1 in Lewis CIA, screening OCA in BDL, or tracking empagliflozin → Zucker fat IL-6 ↓40%, it's the rat IL-6 reagent that doesn't make you blame your rat strain.
Product Reference: KTE9004 – EliKine™ Rat IL-6 ELISA Kit
Learn more and order: https://www.abbkine.com/product/elikine-rat-il-6-elisa-kit-kte9004/
(For Research Use Only; not for diagnostic procedures in humans.)





