




You Swapped ERα for ERβ Because the Story "Didn't Fit Alpha"—Now the Reviewer's Asking for Proof: Why Your ERβ Antibody Choice Is the Difference Between a Precision Hormone Paper and an Embarrassing Western (ABP0087 Is the Fix)
There's a very specific kind of sinking feeling that hits when your paper comes back with theMethods critique that reads: "Given the structural homology between ERα (ESR1) and ERβ (ESR2), the authors must providevalidation of the ERβ antibody's specificity—preferably including a control showing no signal in ERβ-knockdown or ERα-dominant tissue." If you've been winging it with a generic "anti-estrogen receptor" polyclonal that was raised against the highly conserved DNA-binding domain, you know exactly what comes next: your ~55 kDa band might be ERβ… or it might be ERα cross-reactivity, or some random nuclear DNA-binding protein that runs close enough to ruin your densitometry. The uncomfortable truth? ERβ (ESR2/NR3A2, UniProt Q92731, Gene ID 2100) is NOT a niche "bonus panel" for sex hormone work—it's the receptor that actually mediates the protective, anti-proliferative, pro-differentiation side of estrogen signaling, and it deserves an antibody built around an epitope it doesn't share with ERα.
ERβ Is the "Quiet Twin" of Estrogen Signaling—and It Demands a Dedicated, Epitope-Conscious Reagent
While ERα (ESR1) grabs the oncology headlines (~70% of breast cancers are ERα-positive, tamoxifen/fulvestrant act primarily on alpha), ERβ (encoded by ESR2) is the receptor that actually dominates in prostate epithelium, ovarian granulosa cells, osteoblasts/osteocytes, specific hypothalamic nuclei, vascular endothelium, and key colorectal/thyoid/ lung-tissue contexts. Instead of driving a classical proliferative program the way unopposed ERα can, ERβ antagonizes several ERα-mediated proliferative outputs, promotes differentiation, apoptosis in select lineages, and anti-inflammatory transcriptional programs (including cross-talk with PPARA/PPARG and the Nrf2/ARE antioxidant axis in vasculature and colon).
The biochemical problem is real: ERβ and ERα share the N-terminal AF-1 / DNA-binding domain architecture, so any polyclonal raised against "full-length ER" or an N-terminal/GST-fusion covering the DBD will happily blur the two. What you need for a clean figure is an anti-ERβ reagent raised against a human ERβ-specific peptide region (here, around the non-phosphorylation site of S105)—a sequence that distinguishes ESR2 from ESR1—so your ~55–59 kDa band actually means ERβ, not "something nuclear that looks close."
Enter ABP0087 — ERβ Polyclonal Antibody (Abbkine), Built Around an ERβ-Unique Immunogen
This isn't a repurposed ERα serum. It's a rabbit polyclonal IgG raised against a synthesized peptide derived from human ERβ around the non-phosphorylation site of S105—a region chosen specifically to avoid the DBD overlap that causes the ERα/ERβ identity crisis in cheaper reagents.
Parameter ABP0087 (ERβ Polyclonal Antibody)
Target ERβ / Estrogen Receptor β / ESR2 (UniProt Q92731, Gene ID 2100)
Aliases ESR2; ESTRB; NR3A2; ER-beta; Nuclear receptor subfamily 3 group A member 2
Immunogen Synthesized peptide derived from human ERβ around the non-phosphorylation site of S105 (ERβ-specific epitope, not the conserved DBD)
Host / Isotype Rabbit · IgG · Polyclonal (affinity-purified from antiserum via epitope-specific affinity chromatography)
Reactivity Human, Mouse, Rat (H/M/R cross-validated)
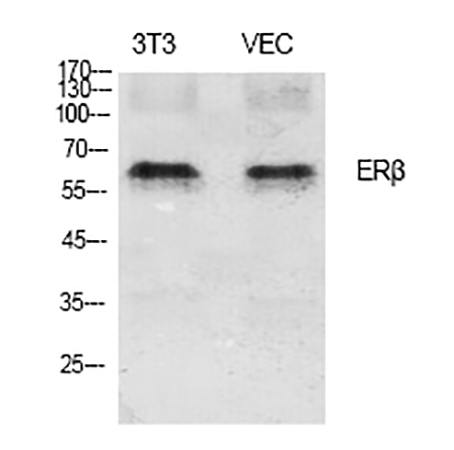
Calculated MW ~59 kDa (canonical ERβ; observed band typically ~53–59 kDa depending on gel system & splice)
Cellular localization Nucleus (also reported cytoplasm/mitochondria depending on isoform, ligand state, and fixation)
Validated apps & starts WB: 1:500–2,000 · IF: 1:50–300 · IHC-P: 1:50–300 · ELISA: ~1:20,000
Format / Conc. Liquid, 1 mg/mL in PBS pH 7.4 + 0.5% BSA + 0.02% NaN₃ + 50% glycerol
Storage / Ship -20°C, stable 1 year from ship date; centrifuge vial after thawing / before opening; aliquot to avoid repeated freeze–thaw; ships blue-ice gel pack
Status For research use only; not for human/clinical diagnostic use
The key differentiator—same story as the ERα article, but applied to the beta side—is that epitope choice = specificity. A peptide immunogen centered on S105-flanking sequence gives you a much higher probability that your ~55–59 kDa nuclear band is ERβ, not ERα bleed-through or a DNA-binding impostor.
What Actually Changes in Your Figures When ERβ Behaves Instead of "Showing Up Somewhere Near 55 kDa"
① Your "ERβ is pro-apoptotic / anti-proliferative here" claim gains a spine.
Run ABP0087 at 1:1,000–2,000 on a positive tissue (rat prostate epithelium, ovary, or an ERβ-overexpressing line) and—critically—a negative control (ERβ-knockdown via siRNA/shRNA, or an ERα-dominant line like MDA-MB-231 where ERβ is natively negligible). When the ~55–59 kDa band disappears in the knockdown and stays in the positive, your reviewer sees proof, not assertion.
② Your IHC-P on FFPE patient cores / xenografts stops being "nuclear brown stuff."
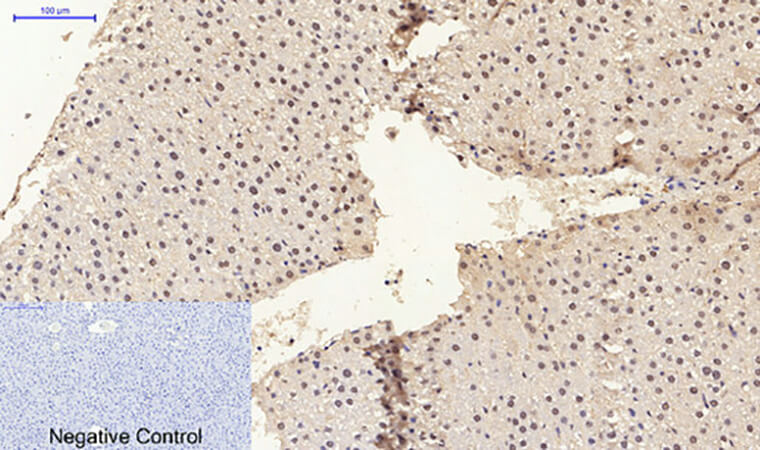
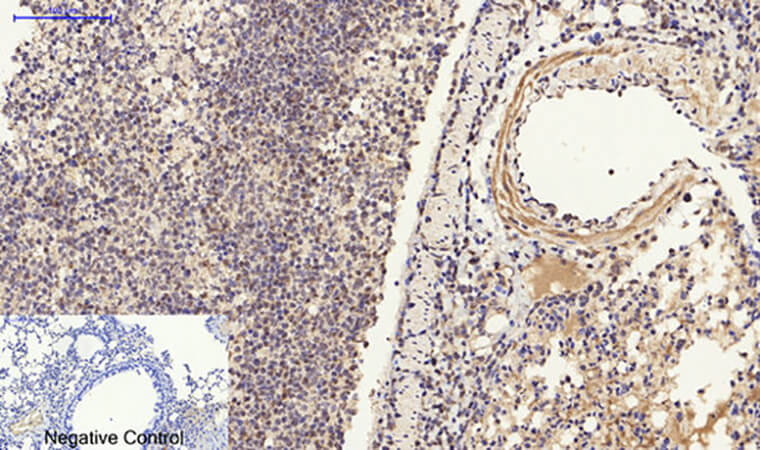
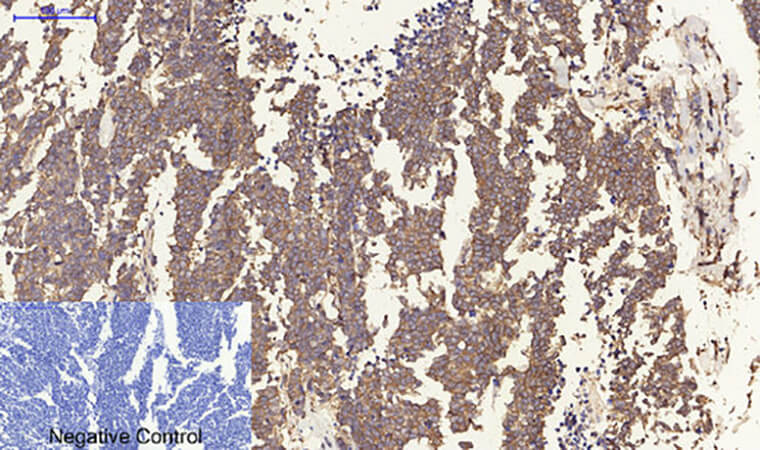
ERβ's clinical intrigue is real: it's been linked to better differentiation score in prostate and colorectal carcinoma, protective vascular/endothelial phenotypes, and ovarian follicle maturation dynamics. Used at 1:100–200 (4°C overnight) with a proper citrate pH 6.0 or EDTA pH 8.0 antigen retrieval, ABP0087 gives you nuclear-restricted staining whose intensity gradient you can actually defend during TMA scoring, rather than a diffuse cytoplasmic "tan" that makes pathologists wince.
③ One vial, three platforms, zero reinvention.
Because it covers WB + IHC-P + IF (+ ELISA-range utility), your cell-lysate screen → xenograft validation → FFPE cohort scoring all ride the same rabbit polyclonal/epitope, keeping your Methods tight and your batch-consistency headache minimal.
The Bench Rules That Keep Your ~55–59 kDa Band (and Your Friday Night) Intact
ERβ is a nuclear hormone receptor whose ligand-binding domain is structurally sensitive and whose best Westerns come from freshly prepared, protease-inhibitor-guarded nuclear-enriched or total lysates—not lysates that sat at 4°C for three hours while you finished cloning.
• Centrifuge before opening. The stock is 1 mg/mL in 50% glycerol/PBS—dense. Brief spin recovers every µL from cap/septum.
• Aliquot Day 1 into 5–10 µL tubes. The format tolerates -20°C beautifully, but repeat freeze–thaw is what aggregates IgG and raises your nuclear-background fog.
• Mind the NaN₃ (0.02%). It inhibits HRP, so after your primary incubation on the membrane: 3–4 thorough TBST washes before the HRP-conjugated anti-rabbit secondary. Basic, but it's the #1 reason someone says "my ERβ band is faint."
• WB dilution scouting: start 1:1,000 on a known-positive (rat prostate, ovary, or ERβ-construct-transfected lane). The suggested ceiling goes to 1:2,000 for a clean signal if your transfer and blocking are dialed in. Always include: a positive and a negative/knockdown lane once, document it, and breathe easier every time Reviewer #2 opens your supplement.
• For IHC-P: standard citrate pH 6.0 microwave/steamer retrieval (or EDTA pH 8.0 for tough cores), peroxidase block (3% H₂O₂), normal serum block → 1:100–200, 4°C overnight → HRP-secondary → DAB → hematoxylin counter. Keep your retrieval time identical across the cohort or your intensity scores lose meaning.
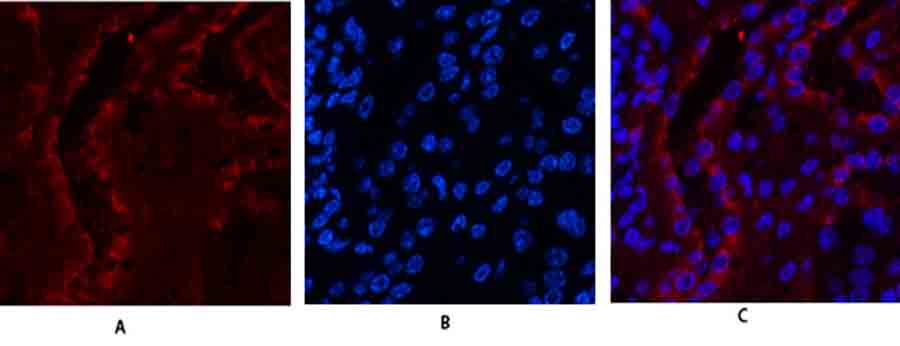
• For IF: 1:100–200 on permeabilized, blocked cells; use fluorophore-appropriate secondary; DAPI for nucleus; image on a calibrated scope so "intensity" isn't post-hoc Photoshop.
Where ABP0087 Earns Its Line in Real, Cited Work
Research Context Why ERβ (ABP0087) Must Be Specific, Not "Close Enough"
Prostate biology & ERβ-selective ligands / SERMs/SARMs (non-proliferative ERβ agonist programs) ERβ in basal/prostate epithelium is the differentiation guard — your WB/IHC must exclude ERα bleed
Colorectal cancer differentiation & IBD-related dysplasia ERβ loss correlates with poorer differentiation; nuclear IHC scoring only works if the antibody isn't picking up ERα or random nuclear DBD proteins
Ovarian follicle maturation & PCOS / endometriosis models Granulosa-cell ERβ is the dominant isoform; a S105-flanking epitope gives you the clean nuclear signal that matters
Vascular/atherosclerosis & endothelial estrogen signaling ERβ-mediated NO/prostacyclin pathways are cardio-protective; quantifying ERβ protein (not just "total ER") sharpens the mechanism
Osteoblast/osteocyte & bone-loss models (menoopause, oophorectomy, SERM comparison) ERβ contributes to bone homeostasis; tracking it alongside ERα gives you a receptor-ratio story that's much harder to dismiss
Environmental EDCs (BPA, genistein, alkylphenols) — receptor-selective profiling If your EDC binds both isoforms but only disrupts one's transcriptional output, you need an ERβ-specific tool that doesn't cross-signal on ERα
A Clean Methods Paragraph You Can Drop Straight In
Estrogen Receptor β (ERβ/ESR2, UniProt Q92731) was detected with a rabbit polyclonal anti-ERβ (ABP0087; Abbkine), immunogen: synthesized peptide derived from human ERβ around the non-phosphorylation site of S105, at 1:1,000–2,000 for Western blot (observed ~55–59 kDa) and 1:100–200 for IHC-P on FFPE sections following citrate pH 6.0 antigen retrieval, per the manufacturer's recommendations. Membranes were washed thoroughly prior to HRP-secondary incubation to remove residual azide (0.02%) from the antibody storage buffer. Specificity was confirmed using ERβ-knockdown (siESR2) or ERα-dominant negative-control lysates as appropriate.
Explore the ERβ Polyclonal Antibody (ABP0087) full specs, datasheet & ordering options here:
🔗 https://www.abbkine.com/product/er%ce%b2-polyclonal-antibody-abp0087/
(For research use only. Not for human or clinical diagnostic use. Centrifuge before opening; aliquot to avoid freeze–thaw; 0.02% NaN₃ present — rinse membranes thoroughly before HRP-secondary.)





