




Your Metabolic Phenotyping Looks "Right" Until the Reviewer Asks About Leptin Dynamics—Here's Why Your Current Detection Method Is Burning Both Your Serum Budget and Your Credibility (KTE6026 Is the Fix)
There's a very specific kind of frustration known to every obesity, adipose biology, and metabolic-disease lab: you've built a beautiful story around HFD-induced weight gain, insulin resistance, or bariatric-surgery recovery, your glucose/GTT/ITT curves tell a crisp tale, and your adipokine Western (adiponectin, resistin, FABP4) looks clean. Then Reviewer #2 drops the line every metabolic paper fears: "The authors are encouraged to provide quantitative leptin (LEP) protein levels in serum/plasma with proper assay validation, rather than inferring from adipose Lep mRNA alone." And suddenly you realize your "leptin data" is three pooled mouse sera run on a half-dead Luminex bead with a bloated CV, or a hand-me-down ELISA where the standard curve shifts every Tuesday and your ob/ob positive control is the only well that looks convincing.
Leptin Is the Original Adipose "Hunger Hormone"—and Its Protein-Level Quantification Is the Gatekeeper Your mRNA Panel Can't Replace
Leptin (LEP, UniProt P41159, Gene ID 3952, aliases OB / Obese protein / Obesity Factor) is a ~16 kDa class-I helical cytokine secreted primarily by white adipocytes (with secondary production in brown fat, placenta, gastric mucosa, and even mammary epithelium). Its canonical circuit is iconic: leptin enters the arcuate nucleus of the hypothalamus, binds LEPR (Ob-Rb, the long signalling isoform), suppresses NPY/AgRP orexigenic neurons, activates POMC/CART anorexigenic neurons, and — voilà — you stop eating and ramp EE. But the modern view is far richer: leptin is now recognized as a systemic metabolic hormone that regulates insulin sensitivity, bone remodelling (via Wnt/β-catenin crosstalk), fertility (GnRH pulsatility), and even Th1/Th17 immune polarization in chronic inflammation and rheumatoid settings.
The core experimental problem? Leptin mRNA ≠ secreted leptin protein, especially in high-fat feeding, lipodystrophy, or PCOS models where adipose expands but leptin resistance at the BBB decouples circulating concentration from hypothalamic response. If your story depends on whether the hormone is actually there in the serum — and whether your intervention (exercise, GLP-1RA, bariatric surgery, adipose-selective knockout) moved it in a dose-responsive, physiologically meaningful way — then a specific, sensitive, sandwich ELISA with a calibrated standard curve isn't optional. It's the centrepiece of a defensible metabolic panel.
Why "Any Leptin ELISA" Isn't Good Enough (and Why Your Current Kit Might Be the Reason for That Wide Error Bar)
Leptin's ~16 kDa size and helical structure make it amenable to sandwich detection, but three practical traps destroy data quality in real labs:
- Healthy human fasting leptin spans a huge range (~3–15 ng/mL in lean individuals, 30–80+ ng/mL in obesity), while mouse/rat can sit lower and your sample volume is often limited — so you need a wide dynamic range AND a low floor so you're not coding half your lean controls as "<LOD."
- Serum/plasma matrix effects from lipids, hemolysis, and anticoagulant choice can subtly shift apparent OD if the antibody pair isn't rigorously validated for those fluids.
- Plate-to-plate coating drift is the silent killer — if your standard curve slope changes 15% between Monday and Wednesday, your inter-assay normalization becomes a stats nightmare.
Enter EliKine™ Human Leptin ELISA Kit — KTE6026 (Abbkine)
This is a quantitative two-site (sandwich) ELISA engineered so the parts that usually drift can't:
Parameter KTE6026 Specification
Assay type Sandwich ELISA — anti-Leptin capture Ab pre-coated on 96-well plate
Target Human Leptin / LEP / OB (UniProt P41159, Gene ID 3952)
Aliases LEP; LEP_HUMAN; Obesity Factor; Obese protein; Leptin Precursor; FLJ94114; LEPD
Samples Cell culture supernatants · Serum · Plasma (heparin/citrate — avoid EDTA conflicts w/ some downstream HRP workflows) · Other biological fluids
Sensitivity (LOD) 16 pg/mL
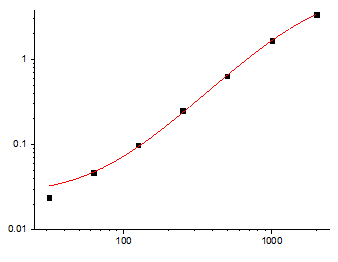
Dynamic range 31.25 – 2,000 pg/mL (7-point standard curve)
Detection TMB → 450 nm (620–650 nm optional reference)
Key components Pre-coated anti-Leptin 96-well plate · Leptin protein standard · Biotin-anti-Leptin detection Ab · EliKine™ Streptavidin-HRP · Standard/sample diluents · Wash buffer · TMB substrate · Stop solution · Sealing films
Storage / Ship 2–8°C (unopened); ship blue-ice gel pack; For research use only
The competitive edge — as with every well-built EliKine kit — is that the capture antibody is locked to the plate, the biotin-detection antibody hits a second, non-overlapping epitope, and the supplied recombinant human Leptin standard means you interpolate from a lot-calibrated curve, not a theoretical assumption. Your 450 nm signal is proportional to actual LEP protein, not "whatever stuck to a polyclonal serum coating."
What Actually Changes in Your Metabolic Paper When Leptin Is Finally a Defensible Number
① Your HFD / DIO / bariatric / GLP-1 story gains a causal anchor instead of a correlation.
When you can write:
Serum leptin was quantified by sandwich ELISA (EliKine™ KTE6026; Abbkine; LOD 16 pg/mL, range 31.25–2,000 pg/mL) and showed a 4.3-fold rise with HFD that was partially reversed by [intervention],
…the reviewer sees a measurement, not a hope. Paired with adiponectin (separate ELISA), insulin, and a HOMA-IR or GTT, your metabolic panel becomes the kind that clears in one round.
② Your serum sample economy stops forcing "pool three mice per lane" compromises.
The microplate format means you can run individual animal sera in triplicate across a cohort of n=8–12, use the supplied standard curve on every plate, and normalize to a dilution series if a super-obese sample overshoots 2,000 pg/mL (dilute in the kit's sample diluent — never plain water). That individual-animal resolution is what powers a proper stat test instead of a pooled SD that hides the variance.
③ Clinical-pilot / cohort-style work becomes viable without a core-lab analyser.
Working with human serum or plasma from metabolic clinics? The 16 pg/mL floor means even unexpectedly lean donors produce a real interpolated value rather than an <LOD you have to left-censor. And because the plate is pre-coated, your inter-plate CV stays in the defensible range across a 48T/96T run.
The Bench Rules That Keep Your 450 nm Curve From Embarrassing You
These are the operational disciplines that make an EliKine Leptin run reviewer-proof:
• RT balance (≥30 min): Bring all components to room temperature before cracking the pre-coated plate seal. Cold reagent on a warm lid = condensation = edge drift.
• Never cross-mix lot numbers. Don't "borrow" wash buffer or Streptavidin-HRP from a different batch. The standard curve is lot-calibrated — treat it that way.
• Fresh tips, every transfer. Leptin is ~16 kDa and sticky; one contaminated well cascades through your curve.
• Seal unused strips back into the foil pouch with desiccant → 2–8°C. Moisture is the silent killer of pre-coated plates.
• Gentle mixing: low-speed orbital shake or manual tap every ~10 min during incubations — never vortex the plate.
• Duplicates/triplicates: always. The kit explicitly recommends replicate wells; your CV (and your statistician) will thank you.
• Sample prep note: Allow clot to form at room temp for serum; for plasma, heparin or citrate is typical — follow the manual's anticoagulant guidance and keep samples cold until they hit the well.
Where KTE6026 Earns Its Spot in Real, Funded Programs
Research Context Why Leptin (16 pg/mL–2,000 pg/mL) + Pre-Coated Sandwich Is Non-Negotiable
Diet-Induced Obesity (DIO) & HFD models Serum leptin is the adipose-expansion readout; paired with ITT/GTT, it validates the metabolic state
Bariatric / VSG / RYGB outcomes Post-op leptin drops faster than weight, and the kinetics matter — individual-animal ELISA beats pooled clinical chem-panel proxies
Leptin resistance & BBB transport studies You need circulating LEP accurately quantified to argue the problem is transport/signalling, not hormone absence
PCOS & reproductive endocrine work Hyperleptinaemia is a diagnostic thread; precise ELISA lets you correlate LEP vs. testosterone/LH/FSH cleanly
Adipose tissue explant / 3T3-L1 differentiation CM leptin secretion validates successful adipogenesis and functional secretory status alongside PPARγ/aP2
Inflammatory / autoimmune links (Th1 bias via leptin) Leptin is immunomodulatory; quantifying it cleanly prevents the "is this just adipose inflammation?" pushback
A Clean Methods Paragraph You Can Drop Straight In
Serum/plasma leptin (LEP) was quantified using a sandwich ELISA (EliKine™ Human Leptin ELISA Kit, KTE6026; Abbkine) per the manufacturer's protocol. A microplate pre-coated with capture anti-Leptin was incubated with standards and samples; following washing, a biotinylated anti-Leptin detection antibody and EliKine™ Streptavidin-HRP were applied, developed with TMB, stopped, and read at 450 nm (620–650 nm reference). Values were interpolated from the supplied recombinant human Leptin (UniProt P41159) standard curve (range 31.25–2,000 pg/mL; LOD 16 pg/mL) and expressed as pg/mL or ng/mL as indicated (samples exceeding the upper limit were diluted in kit sample diluent and corrected).
Explore the EliKine™ Human Leptin ELISA Kit (KTE6026) full specs, manual & ordering options here:
🔗 https://www.abbkine.com/product/elikine-human-leptin-elisa-kit-kte6026/
(For research use only. Not for human or clinical diagnostic use.)





