




Your Th17 & Autoimmune Blockbuster Lives or Dies on One Heterodimeric Cytokine—Why Measuring "IL-12p40" Won't Cut It Anymore, and How Abbkine's KTE6025 Finally Gives You SpecificIL-23 Numbers That Survive a Tough Reviewer
If you've been following the last decade of immunology, you already know where the money, the breakthrough biologics, and the fiercest reviewer scrutiny have all converged: the IL-23 / Th17 axis. We went from "IL-17 is interesting" to ustekinumab (anti-IL-12p40) → guselkumab / risankizumab (anti-IL-23p19) being billion-dollar franchise therapies for psoriasis, Crohn's disease, and axial spondyloarthritis—because blocking the unique p19 subunit of IL-23 shuts down pathogenic Th17 effector programming without broadly immunosuppressing the IL-12 (p35/p40) interferon-γ axis you still need for host defense. The catch? Most labs still quantify this pathway the lazy way—running a p40 ELISA that lumps IL-12 (p35/p40) and IL-23 (p19/p40) into one ambiguous number, or relying on a Luminex bead with marginal sensitivity in the low-pg/mL range. When Reviewer #2 asks the obvious question—"How do the authors distinguish IL-23 from IL-12 given their shared p40 subunit?"—you realize your entire mechanism section is balancing on an assay that was never specific to begin with.
IL-23 Is a Heterodimer—and That p19 Subunit Is Exactly Why "Shared p40" Assays Are a Category Error
Interleukin-23 (IL-23) is formally composed of IL-12p40 + IL-23p19 (UniProt Q9NPF7, Gene ID 51561), linked by a disulfide bond. The p40 subunit it shares with IL-12(p35/p40) is not the business end that defines its unique biology. What makes IL-23 special—and the reason three FDA-approved anti-p19 antibodies exist—is that p19 alone drives the Th17 differentiation/maintenance program via the IL-23 receptor (IL-23R + IL-12Rβ1) expressed on memory CD4⁺ T cells, γδ-T cells, innate lymphoid cells (ILC3), and certain dendritic subsets. The functional readout of that signaling is the sustained production of IL-17A, IL-17F, and IL-22—the triad that both protects mucosal barriers and fuels the pathologies above when dysregulated.
Here's the practical problem in plain English:
• An anti-p40 ELISA will detect BOTH IL-12 AND IL-23 → you can't tell which cytokine your treatment affected.
• A properly designed anti-p19 sandwich ELISA captures only the p19-containing heterodimer (i.e., IL-23) → that's a mechanistically honest number.
That distinction is what separates a publishable Th17 story from one that gets kicked back with "the authors must provide p19-specific quantification."
The Sandwich ELISA Principle Behind KTE6025—Same Gold-Standard Architecture, But P19-Specific by Design
The EliKine™ Human IL-23 ELISA Kit (KTE6025) is a quantitative two-site (sandwich) ELISA built around a pre-coated anti-human IL-23 capture antibody (specific to the IL-23 complex, effectively targeting the p19/heterodimer configuration), a biotinylated detection antibody that binds a second, non-overlapping epitope, and Streptavidin-HRP → TMB → 450 nm readout with an optional 620–650 nm reference wavelength.
Parameter KTE6025 Specification
Assay type Sandwich ELISA (two-site, capture → detect)
Target Human IL-23 (heterodimer: IL-12p40 + IL-23p19 / UniProt Q9NPF7, Gene ID 51561)
Aliases IL-23A; IL-23 p19; IL-23 subunit alpha; IL23P19; SGRF; JKA3-induced upon T-cell activation
Samples Cell culture supernatants · Serum · Plasma (heparin/citrate) · Other biological fluids
Sensitivity (LOD) 16 pg/mL
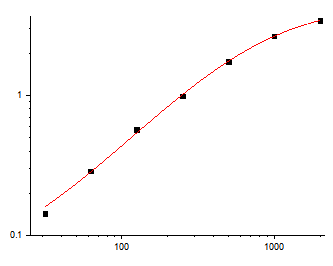
Dynamic range 31.25 – 2,000 pg/mL (7-point standard curve)
Detection TMB → 450 nm (620–650 nm optional reference)
Key components Pre-coated anti-IL-23 96-well plate · IL-23 protein standard · Biotin-anti-IL-23 detection Ab · EliKine™ Streptavidin-HRP · Standard/sample diluents · Wash buffer · TMB substrate · Stop solution · Sealing films
Storage / Ship 2–8°C (unopened); ship blue-ice gel pack; For research use only
The scientific advantage of the pre-coated format + supplied recombinant IL-23 standard isn't marketing fluff. It's the thing that lets you write, "IL-23 was quantified by p19-targeted sandwich ELISA (KTE6025, Abbkine; LOD 16 pg/mL, range 31.25–2,000 pg/mL) with a kit-supplied standard curve," and have the reviewer nod instead of asking whether your "IL-23" number is secretly 40% IL-12 contamination.
What Actually Changes When Your IL-23 Readout Is Finally Specific (and Sensitive Enough to See Basal)
① Your anti-p19 therapeutic story becomes defensible at the protein level.
If you're testing guselkumab/risankizumab biosimilar candidates, small-molecule Th17 modulators, or microbiome-short-chain-fatty-acid effects on DC→Th17 priming, the key question is whether IL-23 protein in the supernatant actually dropped. A p19-specific sandwich ELISA with 16 pg/mL floor catches that delta—especially for human PBMC/MDDC co-cultures where unstimulated IL-23 can hover near the noise floor.
② Your "IL-12 vs. IL-23" mechanistic claim stops being a conjecture.
You can now show (not just cite) that your treatment modulated IL-23 (p19) while your IL-12p70 (measured separately with its own p35/p40 sandwich) stayed flat, or vice versa. That orthogonal pair of numbers is exactly what turns a Th17 paper from correlative to causal.
③ Ileal Crohn's / colitis / psoriasis-model validation panels get the resolution they demand.
DC-maturation protocols + TLR ligation (TLR2/4 agonists, fungal β-glucan, S. aureus WallC, etc.) produce IL-23 in a tight, inducible window that fits beautifully inside the 31.25–2,000 pg/mL range. The pre-coated plate means your inter-assay CV isn't at the mercy of who coated well A1 on a Tuesday.
The Bench Discipline That Keeps Your 450 nm Curve From Embarrassing You
These rules mirror every EliKine kit's operational requirements—and they're exactly the lines that make a Methods section reviewer-proof:
• RT balance (≥30 min): Bring all components to room temperature before opening the sealed plate pouch. Cold droplets on a warm lid = condensation = edge-effect drift you'll curse at 11 PM.
• Never cross-mix lot numbers. Don't borrow wash buffer or Streptavidin-HRP from a different batch. The standard curve is lot-calibrated; treat it that way.
• Fresh tips, every transfer. IL-23 is p19 (18–20 kDa) + p40 (~34–40 kDa disulfide-linked heterodimer—the captured complex is sticky, and one contaminated tip cascades through your entire standard curve.
• Seal unused strips back into the foil pouch with desiccant → 2–8°C. Moisture is the silent killer of pre-coated plates.
• Gentle mixing: low-speed orbital shake or a tap every ~10 min during incubations. No vortex-the-plate chaos.
• Duplicates/triplicates: always. The kit expects it; your CV will thank you.
Where KTE6025 Earns Its Spot in Real, Funded Programs
Research Context Why p19-specific IL-23 (16 pg/mL–2,000 pg/mL) Matters
Psoriasis / imiquimod or IL-23 intradermal models Lesional IL-23 drives IL-17/IL-22 → p19-specific ELISA is the only way to dissociate from IL-12p70
Crohn's / ileal inflammation & microbiome–immune crosstalk DC-derived IL-23 is the gatekeeper of pathogenic Th17 in the mucosa; 16 pg/mL floor catches low-secreting DCs without "ND" purgatory
Anti-p19 biologic PK/PD & biosimilar development Target-engagement bioassay = measure the ligand you just blocked; pre-coated format = consistent across timepoints
Cancer immuno-oncology (TME Th17/IL-23 paradox) Tumor-infiltrating DCs can fuel or restrain via IL-23 → quantifying the actual heterodimer (not p40 proxy) clarifies which camp your data sits in
Innate immune training & vaccine-adjuvant screens (TLR2/4 → DC maturation) DC IL-23 secretion is a primary pharmacodynamic marker; sandwich ELISA with kit-standard gives you a traceable U/mL
A Drop-In Methods Paragraph You Can Borrow
IL-23 was quantified using a p19-targeted sandwich ELISA (EliKine™ Human IL-23 ELISA Kit, KTE6025; Abbkine) per the manufacturer's protocol. A microplate pre-coated with capture anti-IL-23 was incubated with standards and samples; following washing, a biotinylated anti-IL-23 detection antibody and Streptavidin-HRP were applied, developed with TMB, stopped, and read at 450 nm (620–650 nm reference). Values were interpolated from the supplied recombinant IL-23 (p19/p40) standard curve (range 31.25–2,000 pg/mL; LOD 16 pg/mL) and expressed as pg/mL, or normalized to cell number/protein as indicated.
Explore the EliKine™ Human IL-23 ELISA Kit (KTE6025) full specs, manual & ordering options here:
🔗 https://www.abbkine.com/product/elikine-human-il-23-elisa-kit-kte6025/
(For research use only. Not for human or clinical diagnostic use.)





