




The Cystinuria Transporter You Can Finally Quantify: SLC7A9 (b⁰,⁺ BAT1) ELISA for Nephrology, Gut, and Transport Physiology Labs
There are proteins that sit at the center of a disease mechanism but somehow never feel “accessible” to a standard wet-lab workflow — and SLC7A9 is the textbook example. Officially the B⁰,⁺-type amino acid transporter 1 (also called BAT1, b⁰,+AT, or hAT2), SLC7A9 encodes the heavy-chain-associated light-chain subunit that teams up with SLC3A1 (rBAT) to form the system B⁰,⁺ heteromeric exchanger at the apical brush border of proximal tubule kidney cells and intestinal enterocytes. This antiporter imports cysteine, cystine, and dibasic AAs (Lys, Arg, Orn) in exchange for neutral/cationic AAs, and when its activity collapses, cystine reabsorption fails — causing the cystine supersaturation that defines non-type I cystinuria. The catch is that SLC7A9 is a membrane protein, not a secreted signal, so labs often get stuck oscillating between “mRNA looks changed” and “Western band is too faint/too tricky to densitometrize properly.” The Human B⁰,⁺-type amino acid transporter 1 (SLC7A9) ELISA Kit (KTE60585) from Abbkine is designed to break that bottleneck by giving you a sandwich ELISA that treats SLC7A9 like a quantifiable variable — not a gamble — in cell/tissue lysates and membrane-enriched preparations.
SLC7A9 in One Sentence — Then Why It Controls Kidney Stone Risk
SLC7A9 (UniProt: Q9NRG9, ~64–68 kDa, 12 TM segments) does not move amino acids on its own; it docks into the heteromeric complex where SLC3A1/rBAT provides the glycosylated “anchor/display” subunit and SLC7A9 provides the transport pathway. Together, at the proximal tubule apical membrane, they recycle cyst(e)ine and dibasic AAs from the filtrate back into the blood.
In non-type I cystinuria (MIM 604144), homozygous/compound-heterozygous SLC7A9 loss-of-function disrupts this reclamation: urinary cystine climbs, stones form, and patients present with recurrent nephrolithiasis despite normal rBAT expression. But SLC7A9 isn’t only “kidney stone genetics” — it matters wherever the kidney or gut epithelium has to manage AA reabsorption under acid–base stress, diuretics, high-protein load, or tubular injury, and wherever your experiment manipulates brush-border membrane turnover, trafficking, or heterodimer stability.
Why “Just Run SLC7A9 on a Gel” Isn’t Good Enough Anymore
If you’ve ever tried to densitometrize a ~65 kDa membrane-protein band across a 12-lane blot that’s also fighting uneven transfer near the stacking/gel interface, you already know the problem:
• Membrane proteins are low-abundance at the whole-cell level unless you enrich (brush-border isolates, membrane fractions, polarized epithelium).
• Antibody specificity is everything — one cross-reactive band at ~55–70 kDa ruins your normalization.
• Reviewers increasingly want a calibrated concentration, not “darker vs. lighter,” when the claim is “treatment X reduces transporter protein at the membrane by ~30–40%.”
A sandwich ELISA fixes this by using two independent anti-SLC7A9 epitopes (capture + detection) and a recombinant standard curve on every plate, so your 450 nm readout becomes ng/mL (or ng per µg total protein) instead of a relative-intensity argument.
Assay Principle: What KTE60585 Actually Does on the Bench
Like the rest of Abbkine’s targeted-protein ELISA lines, KTE60585 is a quantitative two-site sandwich ELISA:
- A microplate is pre-coated with a capture antibody specific for human SLC7A9.
- Standards and samples (tissue homogenates, cell lysates, membrane-enriched fractions, biological fluid-compatible preparations) are added; any SLC7A9 present binds.
- After washing, a biotinylated anti-SLC7A9 detection antibody (different epitope) forms the sandwich.
- Streptavidin–HRP binds biotin → TMB generates color ∝ bound SLC7A9.
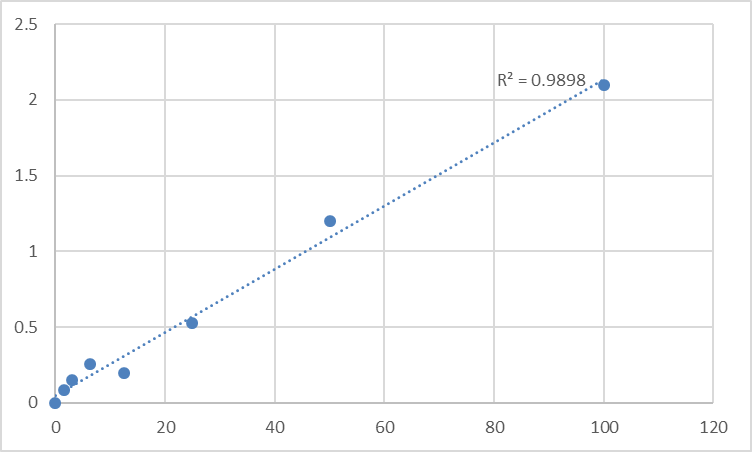
- Stop solution turns the well yellow → read Absorbance at 450 nm → interpolate unknowns from the SLC7A9 standard curve.
The whole run typically fits inside a 3–5 hour window, which means you can process a brush-border-fraction time-course or a drug-treatment panel in a single sitting and actually trust the numbers coming off the plate reader.
Where This Kit Earns Its Keep (And Who Should Care)
- Cystinuria & proximal tubule transport research
Quantify SLC7A9 protein levels in kidney tissue homogenates, tubule isolates, or relevant cell models (e.g., opossum kidney/PTE cell lines where brush-border transporters are tracked) to correlate genotype → transporter expression → functional uptake deficits. ELISA lets you move from “band present” to “how much protein survived the mutation/traffic block?”
- Brush-border membrane (BBMV) prep QC
If your lab makes renal BBMVs for uptake assays, SLC7A9 (often with SLC3A1/rBAT) is a great quantitative marker of apical-enrichment success — and an ELISA is faster than rerunning gels just to check loading.
- Gut–kidney axis, high-protein diet, and acid–base stress models
Dietary protein and acidosis remodel proximal-tubule AA transport; being able to say “SLC7A9 protein at the membrane shifted 1.8× vs. control” with a plate-based curve is a stronger story than an n=3 band.
- Drug-induced tubular injury screening
Cisplatin, tenofovir, and other nephrotoxins hit the proximal tubule first. Tracking whether SLC7A9 drops as part of a transporter-loss signature (alongside NHE3, NaPi-IIa, etc.) is a sensible protein-level endpoint — and ELISA throughput scales better than constant Westerns.
- CRISPR/siRNA validation in transporter biology
Knocking SLC7A9 or SLC3A1? Don’t just show a fainter blot — report % transporter protein remaining ± SEM from a calibrated curve, and do it in membrane fractions, not just whole-cell lysate where the signal can dilute below detectability.
Practical Notes: Membrane Proteins Need a Little Extra Respect
Because SLC7A9 is not a soluble cytokine, your sample prep decides whether the kit sings or struggles:
• Work in BBMV/membrane-enriched or at least well-clarified homogenates (high-speed spin to remove debris and nuclei; keep protease inhibitors cold).
• If you quantify total protein (BCA/KTD3001 or Bradford/KTD3002), express SLC7A9 as ng per mg total protein so your “loading” isn’t a separate religion.
• If you’re coming from polarized epithelia, remember the biologically relevant pool is often biotinylation-protected/apical; whole-cell lysate alone can blur the trafficking story.
• Run a standard curve on every plate — membrane prep variability is why “reuse yesterday’s curve” is a bad idea.
The Bottom Line
SLC7A9 is one of those transporters everyone names when they talk about cystinuria, kidney stone genetics, or proximal tubule reabsorption — but relatively few labs measure cleanly because it’s stuck in the membrane and easy to bury under background. The Human B⁰,⁺-type amino acid transporter 1 (SLC7A9) ELISA Kit (KTE60585) exists to change that: same field-proven sandwich ELISA architecture, anti-SLC7A9 capture + biotin detection, HRP–TMB readout at 450 nm, and a workflow that respects the fact that your time is better spent interpreting transport, trafficking, and disease mechanisms than debating blot exposure levels.
Product Reference: KTE60585 – Human B⁰,⁺-type amino acid transporter 1 (SLC7A9) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-b-0-type-amino-acid-transporter-1-slc7a9-elisa-kit-kte60585/
(For Research Use Only; not for diagnostic procedures in humans.)





