




The IL‑6 Enigma: From Acute‑Phase Response to Cancer Metastasis — How Abbkine's Polyclonal Antibody (ABP0137) Unlocks Precise Detection in Western Blot, ELISA, and IHC
What if a single cytokine could dictate the fate of immune responses, fuel chronic inflammation, drive autoimmune destruction, and even propel cancer metastasis? Interleukin‑6 (IL‑6) — the 21 kDa, four‑helix‑bundle glycoprotein encoded by the IL6 gene on chromosome 7p15.3 — does exactly that. As a pleiotropic cytokine, IL‑6 orchestrates acute‑phase reactions, B‑cell maturation, T‑cell differentiation, hematopoiesis, and metabolic regulation, with serum concentrations that can skyrocket from a baseline of 1–5 pg/mL in healthy individuals to >1,000 pg/mL during sepsis, acute inflammation, or cytokine‑release syndromes . Yet, when you attempt to detect IL‑6 in cell lysates, tissue sections, or serum samples using conventional antibodies, you often encounter poor specificity, high background, cross‑reactivity with other IL‑6‑family cytokines, and inconsistent performance across applications. The Abbkine IL‑6 Polyclonal Antibody (ABP0137) — a rabbit‑derived, affinity‑purified polyclonal antibody — overcomes these hurdles by delivering high affinity, broad application compatibility (Western blot, ELISA, immunohistochemistry), and minimal cross‑reactivity, enabling researchers to precisely track IL‑6 expression in inflammatory, autoimmune, and oncological models with confidence and reproducibility .
IL‑6 Is Not Just a Pro‑Inflammatory Cytokine — It's a Bifunctional Master Regulator That Switches Between Tissue Protection and Pathological Destruction via Classic, Trans‑, and Cluster Signaling
Interleukin‑6 (IL‑6), initially identified as a B‑cell differentiation factor and hybridoma growth factor, operates through three distinct signaling modes that explain its paradoxical roles in homeostasis versus disease . In classic signaling, IL‑6 binds to the membrane‑bound IL‑6 receptor (IL‑6Rα) expressed primarily on hepatocytes, neutrophils, monocytes, and some lymphocytes, then recruits the ubiquitously expressed gp130 (IL‑6Rβ) to form a hexameric complex (2:2:2) that activates JAK‑STAT, Ras‑MAPK, and PI3K‑Akt pathways, driving acute‑phase protein synthesis, fever response, and anti‑inflammatory effects . However, trans‑signaling — where IL‑6 binds to a soluble IL‑6R (sIL‑6R) generated by alternative splicing or ADAM17‑mediated shedding — allows IL‑6 to act on any gp130‑expressing cell (endothelial cells, fibroblasts, neurons), unleashing pro‑inflammatory, pro‑angiogenic, and pro‑fibrotic programs that fuel rheumatoid arthritis, Crohn's disease, and cancer progression . A third mode, cluster signaling (trans‑presentation), occurs when dendritic cells present IL‑6‑IL‑6R complexes to neighboring T cells, driving Th17 differentiation and exacerbating autoimmune neuroinflammation . This signaling plasticity means that IL‑6 can be both protective (promoting liver regeneration, muscle repair, and metabolic homeostasis) and pathogenic (driving cytokine storms, fibrosis, and metastasis) — a duality that makes accurate IL‑6 detection critical for dissecting its context‑dependent functions .
Why Generic IL‑6 Antibodies Fail in Complex Samples — And How Abbkine's Polyclonal Antibody (ABP0137) Combines High Affinity with Multi‑Application Versatility
The Abbkine IL‑6 Polyclonal Antibody (ABP0137) is an affinity‑purified rabbit polyclonal antibody raised against a recombinant human IL‑6 protein . It recognizes endogenous human IL‑6 across multiple applications, including Western blot (WB), ELISA, and immunohistochemistry (IHC‑F) . Unlike monoclonal antibodies that may bind a single epitope (risking detection failure if that epitope is masked or modified), this polyclonal preparation contains a spectrum of antibodies targeting multiple IL‑6 epitopes, enhancing detection sensitivity and robustness, especially in denatured samples (WB) or fixed tissues (IHC) . The antibody is supplied as a liquid in PBS with 0.02% sodium azide and 50% glycerol, with a concentration of 1 mg/mL, and is stable for 12 months when stored at –20°C . Key advantages include:
• High specificity: The antibody shows no significant cross‑reactivity with IL‑11, LIF, CNTF, or other IL‑6‑family cytokines, ensuring clean signals in multiplex assays .
• Broad application range: Validated for WB (1:500–1:2000 dilution), ELISA (1:1000–1:5000), and IHC‑F (1:50–1:200), allowing consistent IL‑6 detection across experimental platforms .
• Reproducible performance: Each batch is QC‑tested using positive controls (IL‑6‑overexpressing cell lysates) to guarantee lot‑to‑lot consistency.
• Ready‑to‑use format: The antibody is pre‑aliquoted and supplied in a convenient volume (30 µL, 100 µL, or 200 µL), reducing preparation time and minimizing freeze‑thaw cycles.
Application Recommended Dilution Sample Types Expected Band/Pattern
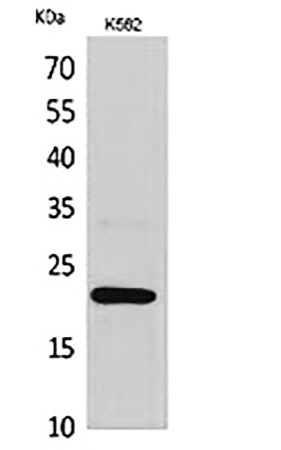
Western blot 1:500 – 1:2000 Cell lysates (HEK293, THP‑1, PBMCs), tissue homogenates (liver, lung, synovium) ~21 kDa band (glycosylated IL‑6); may also detect ~24‑26 kDa forms due to differential glycosylation.
ELISA 1:1000 – 1:5000 Serum, plasma, cell culture supernatants, tissue extracts Coating or detection antibody in sandwich ELISA; linear detection range 15.6–1000 pg/mL when paired with a matched antibody.
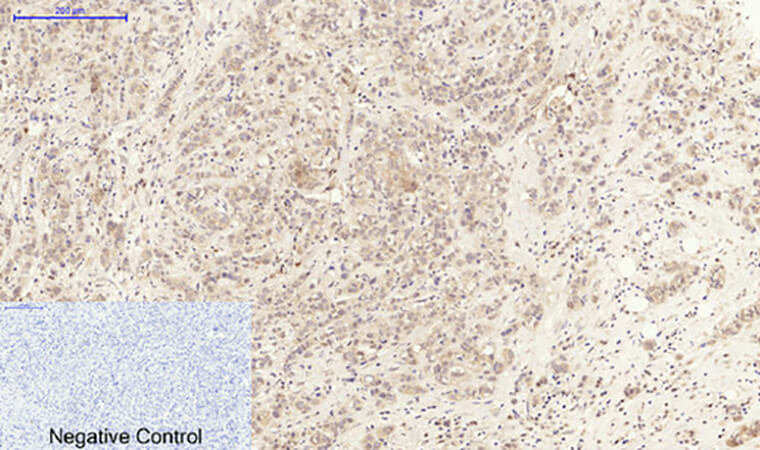
Immunohistochemistry (IHC‑F) 1:50 – 1:200 Formalin‑fixed, paraffin‑embedded (FFPE) tissues, frozen sections Cytoplasmic staining in macrophages, fibroblasts, endothelial cells, and tumor cells; nuclear staining may occur in activated STAT3‑positive cells.
Immunofluorescence (IF) 1:100 – 1:400 Cultured cells, tissue cryosections Punctate cytoplasmic signal; co‑localization with ER/Golgi markers in secreting cells.
Immunoprecipitation (IP) 1:50 – 1:100 Cell lysates, serum Efficient pull‑down of native IL‑6 for downstream mass‑spec or Western analysis.
From Sepsis to Solid Tumors: Five Research Areas Where Precise IL‑6 Detection Is Non‑Negotiable
Research Context Why IL‑6 Measurement Matters How ABP0137 Enables Insights
Sepsis & cytokine‑release syndrome (CRS) Serum IL‑6 levels >1,000 pg/mL correlate with disease severity, organ failure, and mortality; IL‑6 is a key therapeutic target (tocilizumab, siltuximab) . ELISA with ABP0137 allows serial monitoring of IL‑6 in patient serum to guide anti‑IL‑6 therapy and predict outcomes.
Rheumatoid arthritis (RA) & autoimmune diseases Synovial fluid IL‑6 drives Th17 differentiation, osteoclast activation, and joint destruction; IL‑6 trans‑signaling perpetuates chronic inflammation . IHC‑F on RA synovial tissue reveals IL‑6 expression in lining fibroblasts and infiltrating macrophages, informing pathogenesis.
Cancer biology & immunotherapy Tumor‑derived IL‑6 promotes EMT, angiogenesis, and immunosuppression; elevated IL‑6 predicts poor response to immune‑checkpoint inhibitors . Western blot of tumor lysates quantifies IL‑6 upregulation in response to hypoxia, chemotherapy, or targeted therapies.
Neuroinflammation & neurodegenerative diseases Microglial IL‑6 exacerbates Alzheimer's, Parkinson's, and multiple sclerosis via trans‑signaling on neurons and astrocytes . Immunofluorescence on brain sections localizes IL‑6 to activated microglia and astrocytes, linking cytokine expression to pathology.
Metabolic disorders & obesity Adipose‑tissue IL‑6 contributes to insulin resistance and hepatic steatosis; IL‑6 levels correlate with BMI and fasting glucose . ELISA of adipose‑tissue explant supernatants measures IL‑6 secretion in response to lipopolysaccharide (LPS) or fatty acids.
The Step‑by‑Step Protocol: How to Detect IL‑6 in Western Blot, ELISA, and IHC with ABP0137
Western Blot (WB)
- Sample preparation: Lyse cells or tissues in RIPA buffer (with protease inhibitors). Determine protein concentration using BCA assay. Load 20–40 µg of total protein per lane on a 12% SDS‑PAGE gel.
- Transfer: Transfer to PVDF or nitrocellulose membrane at 100 V for 60 minutes in ice‑cold transfer buffer.
- Blocking: Block membrane with 5% non‑fat milk in TBST for 1 hour at room temperature.
- Primary antibody incubation: Dilute ABP0137 1:1000 in blocking buffer; incubate membrane overnight at 4°C with gentle shaking.
- Washing: Wash membrane 3 × 10 minutes with TBST.
- Secondary antibody incubation: Incubate with HRP‑conjugated anti‑rabbit IgG (1:5000) for 1 hour at room temperature.
- Detection: Develop using ECL substrate and image with a chemiluminescence system. Expected band: ~21 kDa.
ELISA (Sandwich)
- Coating: Coat a 96‑well plate with capture antibody (e.g., mouse anti‑human IL‑6) overnight at 4°C.
- Blocking: Block with 1% BSA in PBS for 2 hours at room temperature.
- Sample incubation: Add standards (recombinant IL‑6) and samples; incubate 2 hours at 37°C.
- Detection antibody: Add biotin‑labeled ABP0137 (1:2000 dilution); incubate 1 hour at 37°C.
- Streptavidin‑HRP: Add streptavidin‑HRP (1:1000); incubate 30 minutes at 37°C.
- Substrate: Add TMB substrate; incubate 15 minutes; stop with 2 M H₂SO₄.
- Readout: Measure absorbance at 450 nm. Calculate IL‑6 concentration using a 4‑parameter logistic curve.
Immunohistochemistry (IHC‑F)
- Deparaffinization: Bake FFPE sections at 60°C for 30 minutes, then deparaffinize in xylene and graded ethanol.
- Antigen retrieval: Perform heat‑induced epitope retrieval (HIER) in citrate buffer (pH 6.0) at 95°C for 20 minutes.
- Blocking: Block endogenous peroxidase with 3% H₂O₂, then block non‑specific sites with 5% normal goat serum.
- Primary antibody: Apply ABP0137 (1:100 dilution) overnight at 4°C.
- Secondary antibody: Apply HRP‑conjugated anti‑rabbit IgG for 1 hour at room temperature.
- Detection: Develop with DAB substrate, counterstain with hematoxylin, and mount.
Five Common Pitfalls in IL‑6 Detection — And How ABP0137 Helps You Avoid Them
Pitfall Consequence Solution with ABP0137
Cross‑reactivity with IL‑11, LIF, or CNTF False‑positive signals in Western blot or ELISA, leading to overestimation of IL‑6. ABP0137 is affinity‑purified against human IL‑6 and shows negligible cross‑reactivity with IL‑6‑family cytokines .
Low sensitivity in Western blot IL‑6 is a low‑abundance cytokine; weak bands or no signal even with 50 µg of lysate. The polyclonal nature of ABP0137 increases the chance of epitope recognition, enhancing sensitivity; use 1:500 dilution and enhanced chemiluminescence (ECL).
High background in IHC Non‑specific staining in FFPE tissues, masking true IL‑6 expression. Optimize antigen‑retrieval conditions (citrate buffer, pH 6.0) and use 5% normal serum blocking; ABP0137 produces clean cytoplasmic staining.
Matrix interference in serum ELISA Heterophilic antibodies or soluble receptors (sIL‑6R, sgp130) interfere with antibody binding. Use 1:2 to 1:10 sample dilution and include heterophilic blocking reagents; ABP0137 performs reliably in human serum/plasma .
Lot‑to‑lot variability Inconsistent results when switching antibody batches, disrupting longitudinal studies. Each batch of ABP0137 is QC‑tested on IL‑6‑spiked samples and comes with a certificate of analysis ensuring consistent performance.
Why Choose a Polyclonal Over a Monoclonal Antibody for IL‑6 Detection?
① Polyclonal antibodies recognize multiple epitopes, increasing the likelihood of detecting IL‑6 even if one epitope is masked by post‑translational modifications, aggregation, or denaturation.
IL‑6 can be glycosylated, phosphorylated, or bound to soluble receptors in biological samples; a polyclonal pool increases detection robustness across different sample types (native vs. denatured) .
② Polyclonal antibodies often deliver higher sensitivity in Western blot and IHC because they recruit multiple secondary antibodies, amplifying the signal.
For low‑abundance targets like IL‑6 (often <1 ng/mL in serum), the signal amplification provided by polyclonal antibodies can be decisive, especially when working with limited sample material .
③ Polyclonal antibodies are less prone to complete detection failure due to epitope loss — a risk with monoclonal antibodies if the single epitope is altered.
In fixed tissues (IHC) or reduced/denatured samples (WB), conformational epitopes may be destroyed; polyclonal antibodies, targeting linear and conformational epitopes, offer a safety net .
④ ABP0137 is validated for multiple applications (WB, ELISA, IHC‑F), allowing you to use the same antibody across different experimental workflows, saving time and reducing cross‑validation efforts.
Many monoclonal antibodies are optimized for a single application (e.g., WB only); ABP0137’s multi‑application validation means you can seamlessly transition from Western blot to immunohistochemistry without switching reagents .
⑤ The rabbit host minimizes interference with endogenous immunoglobulins in human samples, reducing background in IHC and ELISA.
Mouse‑derived monoclonal antibodies can bind human anti‑mouse antibodies (HAMA) present in serum, causing false‑positive signals; rabbit polyclonals like ABP0137 circumvent this issue .
Three Critical Validation Steps Before You Trust Your IL‑6 Data
Step Purpose How to Perform with ABP0137
Specificity verification Confirm that the ~21 kDa band in WB is indeed IL‑6, not a cross‑reacting protein. Perform siRNA‑mediated IL‑6 knockdown in a positive‑control cell line (e.g., THP‑1 stimulated with LPS); the band should disappear or diminish. Alternatively, pre‑absorb the antibody with recombinant IL‑6 protein — signal should be abolished.
Linearity & dilution recovery Ensure the antibody detects IL‑6 proportionally across a range of concentrations. Spike known amounts of recombinant IL‑6 into a negative matrix (e.g., IL‑6‑free serum); measure recovery by ELISA using ABP0137 as detection antibody. Recovery should be 80–120% across the assay range.
Cross‑reactivity profiling Rule out binding to IL‑11, LIF, CNTF, OSM, or other IL‑6‑family members. Run Western blot with lysates from cells overexpressing IL‑11, LIF, CNTF; ABP0137 should show no band at the corresponding molecular weights (~20–25 kDa).
From Bench to Bedside: How IL‑6 Detection with ABP0137 Informs Therapeutic Development
① Monitoring anti‑IL‑6 therapies (tocilizumab, siltuximab, sarilumab) in rheumatoid arthritis, Castleman's disease, and cytokine‑release syndrome.
ELISA with ABP0137 can track serum IL‑6 levels before and after treatment, correlating with clinical response and side effects . In clinical trials, IL‑6 is often measured as a pharmacodynamic biomarker to guide dosing.
② Identifying IL‑6‑driven cancer subtypes for targeted intervention.
IHC with ABP0137 on tumor microarrays can stratify patients into IL‑6‑high vs. IL‑6‑low groups, predicting response to IL‑6‑targeted therapies (e.g., siltuximab) or JAK inhibitors . In breast, prostate, and colorectal cancers, IL‑6 expression correlates with EMT, stemness, and poor prognosis .
③ Unraveling the role of IL‑6 trans‑signaling in neurodegenerative diseases.
Double‑label immunofluorescence with ABP0137 and astrocyte/microglial markers can visualize IL‑6 production in the brain of Alzheimer's or multiple‑sclerosis models, helping to distinguish classic vs. trans‑signaling contributions .
④ Screening small‑molecule inhibitors of IL‑6 production or signaling.
Western blot with ABP0137 on LPS‑stimulated macrophage lysates quantifies IL‑6 suppression by JAK inhibitors, STAT3 inhibitors, or natural compounds . High‑throughput ELISA using ABP0137 as detection antibody enables drug‑discovery campaigns .
⑤ Validating IL‑6 as a prognostic biomarker in sepsis, COVID‑19, and acute respiratory distress syndrome (ARDS).
Multiplex ELISA platforms that include ABP0137 can measure IL‑6 alongside other cytokines (TNF‑α, IL‑1β, IL‑10) to define cytokine signatures associated with disease severity and outcomes .
A Ready‑to‑Use Methods Paragraph for Your Paper
IL‑6 protein expression was analyzed using the Abbkine IL‑6 Polyclonal Antibody (ABP0137). For Western blot, cells were lysed in RIPA buffer (Thermo Fisher) containing protease inhibitors. Total protein (30 µg per lane) was separated on a 12% SDS‑PAGE gel and transferred to a PVDF membrane. The membrane was blocked with 5% non‑fat milk in TBST for 1 hour, then incubated with anti‑IL‑6 antibody (ABP0137, 1:1000 dilution) overnight at 4°C. After washing, the membrane was incubated with HRP‑conjugated anti‑rabbit secondary antibody (1:5000) for 1 hour at room temperature. Signals were detected using ECL substrate (Bio‑Rad) and quantified with ImageLab software. For ELISA, a sandwich assay was performed: plates were coated with capture antibody (mouse anti‑human IL‑6, 2 µg/mL) overnight, blocked with 1% BSA, then incubated with standards or samples for 2 hours at 37°C. After washing, biotin‑labeled ABP0137 (1:2000) was added for 1 hour, followed by streptavidin‑HRP (1:1000) for 30 minutes. TMB substrate was added, and absorbance was measured at 450 nm. IL‑6 concentrations were calculated using a 4‑parameter logistic standard curve.
The Five Bench Rules for Reliable IL‑6 Detection with ABP0137
Rule Rationale
Always include a positive control (LPS‑stimulated THP‑1 or PBMC lysates) and a negative control (unstimulated cells or IL‑6‑knockdown lysates) Verifies antibody functionality and assay sensitivity; confirms that the ~21 kDa band is IL‑6‑specific.
For WB, use fresh samples and avoid repeated freeze‑thaw cycles IL‑6 is prone to degradation; aliquot lysates and store at –80°C; thaw on ice only once.
In IHC, optimize antigen‑retrieval time and pH Over‑retrieval can destroy epitopes; under‑retrieval yields weak staining. Test citrate (pH 6.0) vs. Tris‑EDTA (pH 9.0) buffers.
For serum/plasma ELISA, dilute samples 1:2 to 1:10 to minimize matrix effects Undiluted serum may contain heterophilic antibodies or soluble receptors that interfere.
Include a recombinant IL‑6 standard curve in every ELISA run Corrects for inter‑assay variability; ensures quantitative accuracy.
Use low‑binding tubes for sample storage and handling IL‑6 adsorbs to plastic; siliconized or low‑binding tubes reduce protein loss.
When performing multiplex IHC/IF, validate antibody compatibility Ensure secondary antibodies are species‑specific and fluorophore combinations do not bleed‑through.
For longitudinal studies, use the same antibody lot throughout Lot‑to‑lot variations, though minimal with ABP0137, can affect signal intensity.
Always run samples in duplicate or triplicate Improves statistical reliability, especially for low‑abundance IL‑6 measurements.
Document antibody dilution, incubation times, and detection conditions Ensures reproducibility across experiments and lab members.
Explore the Abbkine IL‑6 Polyclonal Antibody (ABP0137) — with high specificity for human IL‑6, validated for WB, ELISA, and IHC‑F, and backed by rigorous QC — for your next inflammation, autoimmunity, or cancer study.
🔗 Product reference: ABP0137 (Abbkine)
(For research use only. Not for diagnostic or therapeutic procedures. Store at –20°C; avoid repeated freeze‑thaw cycles; use within 12 months of receipt.)





