




CD81: The Tetraspanin Master Regulator of Viral Entry, Immune Synapses, and Cancer Metastasis – Why Every Cell Biologist Needs a Reliable Detection Tool Like Abbkine's Polyclonal Antibody (ABP0138)
Imagine a single cell‑surface protein that serves as the primary entry gate for hepatitis C virus, orchestrates the formation of immune synapses, dictates the metastatic potential of tumors, and even marks the elusive extracellular vesicles known as exosomes. This protein is CD81 (Tetraspanin‑28, TAPA‑1) – a 25‑26 kDa four‑pass transmembrane glycoprotein belonging to the evolutionarily conserved tetraspanin superfamily . While often relegated to a mere “exosome marker” in flow cytometry, CD81 is in fact a dynamic signaling hub that organizes membrane microdomains, modulates integrin‑mediated adhesion, regulates B‑ and T‑cell activation, and directly binds viral glycoproteins to facilitate infection . Yet, when you attempt to detect CD81 in Western blot, immunofluorescence, or flow cytometry, you confront its low abundance, complex membrane topology, and propensity to form heteromeric complexes that obscure clear detection. The Abbkine CD81 Polyclonal Antibody (ABP0138) – a rabbit‑derived, affinity‑purified polyclonal antibody – cuts through this complexity by delivering high specificity for human CD81, validated performance across WB, IHC, IF, and ELISA, and minimal cross‑reactivity with other tetraspanins, enabling researchers to accurately map CD81 expression and function in virology, immunology, cancer biology, and extracellular vesicle research .
CD81 Is Far More Than an Exosome Marker – It's a Cholesterol‑Dependent Scaffold That Coordinates Viral Entry, Immune Synapse Assembly, and Integrin Signaling Through Dynamic Tetraspanin‑Enriched Microdomains
CD81 (cluster of differentiation 81), encoded by the CD81 gene on chromosome 11p15.5, is a prototypical tetraspanin characterized by four transmembrane domains, a small extracellular loop (SEL), a large extracellular loop (LEL), and short cytoplasmic N‑ and C‑termini . Unlike single‑pass receptors, CD81 does not act alone; it integrates into tetraspanin‑enriched microdomains (TEMs) – cholesterol‑rich membrane platforms that cluster integrins (α4β1, α3β1), immunoglobulin superfamily members (CD19, CD21), MHC class I/II molecules, and signaling kinases to regulate cell adhesion, migration, proliferation, and differentiation . In virology, CD81’s LEL directly binds the HCV envelope glycoprotein E2 with nanomolar affinity (Kd ≈ 1.8 nM), serving as an essential co‑receptor for hepatitis C virus entry into hepatocytes . Beyond HCV, CD81 facilitates HIV‑1 assembly and release by organizing viral budding sites at the plasma membrane, and it even contributes to Plasmodium sporozoite invasion of hepatocytes during malaria infection . In immunology, CD81 forms a critical co‑stimulatory complex with CD19 and CD21 on B cells, lowering the activation threshold for antigen receptor signaling; on T cells, it associates with CD4 and CD8 to modulate TCR signaling . In cancer biology, CD81 promotes tumor cell invasion and metastasis by regulating integrin‑dependent adhesion and matrix degradation; its overexpression correlates with poor prognosis in triple‑negative breast cancer, colorectal cancer, and hepatocellular carcinoma . And in cell biology, CD81 is a canonical exosome marker because it is enriched on the surface of these extracellular vesicles, where it may mediate vesicle‑cell communication . This functional pleiotropy stems from CD81’s ability to act as a membrane organizer – a property that makes its precise detection essential for dissecting its context‑dependent roles.
Why Detecting CD81 Is Technically Challenging – And How Abbkine's Polyclonal Antibody (ABP0138) Overcomes These Hurdles with High Affinity and Multi‑Application Validation
The Abbkine CD81 Polyclonal Antibody (ABP0138) is an affinity‑purified rabbit polyclonal antibody raised against a recombinant human CD81 protein . It specifically recognizes endogenous human CD81 across a range of applications, including Western blot (WB), immunohistochemistry (IHC), immunofluorescence (IF), and enzyme‑linked immunosorbent assay (ELISA) . Unlike monoclonal antibodies that may fail if their single epitope is masked by post‑translational modifications or protein‑protein interactions, this polyclonal preparation contains a diverse repertoire of antibodies targeting multiple CD81 epitopes, ensuring robust detection even when CD81 is engaged in complexes or partially denatured . The antibody is supplied as a liquid in PBS with 0.02% sodium azide and 50% glycerol, at a concentration of 1 mg/mL, and remains stable for 12 months when stored at –20°C . Key advantages include:
• High specificity: The antibody shows minimal cross‑reactivity with other tetraspanins (CD9, CD63, CD151), ensuring clean signals in multiplex assays .
• Broad application compatibility: Validated for WB (1:500–1:2000 dilution), IHC‑F (1:50–1:200), IF (1:100–1:400), and ELISA (1:1000–1:5000), allowing consistent CD81 detection across experimental platforms .
• Recognition of multiple isoforms: CD81 has two known splice variants; the polyclonal nature of ABP0138 increases the likelihood of detecting both isoforms .
• Reliable performance in membrane‑rich samples: CD81 is a low‑abundance membrane protein; ABP0138 delivers clear signals in membrane fractions, whole‑cell lysates, and tissue sections without requiring excessive sample loads .
• Lot‑to‑lot consistency: Each batch is QC‑tested using CD81‑positive cell lines (e.g., Huh‑7 hepatoma cells) to ensure reproducible sensitivity and specificity.
Application Recommended Dilution Sample Types Expected Result
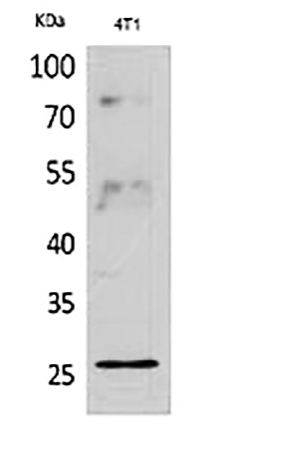
Western blot 1:500 – 1:2000 Cell lysates (Huh‑7, HEK293, B cells), tissue homogenates (liver, spleen, tumor) ~25‑26 kDa band (non‑glycosylated); ~30‑35 kDa band may appear due to glycosylation or dimerization.
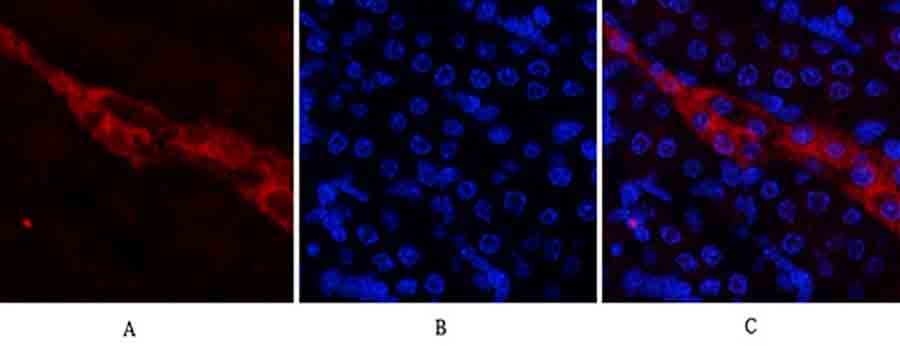
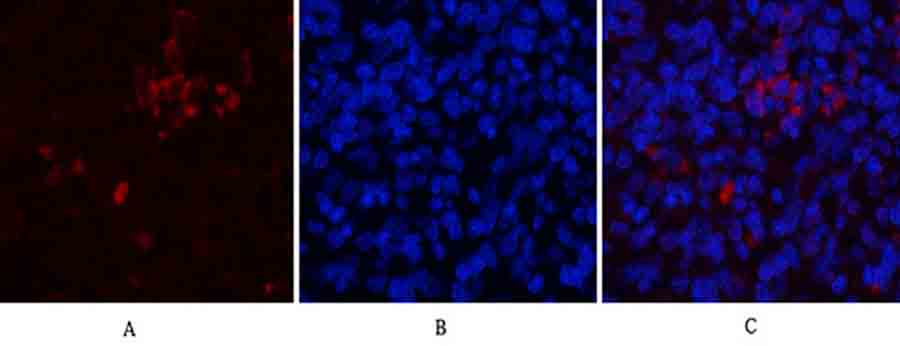
Immunohistochemistry (IHC‑F) 1:50 – 1:200 Formalin‑fixed, paraffin‑embedded (FFPE) tissues, frozen sections Membrane staining on hepatocytes, B cells, endothelial cells, and tumor cells; cytoplasmic staining may also be observed.
Immunofluorescence (IF) 1:100 – 1:400 Cultured cells, tissue cryosections Punctate membrane staining, often co‑localizing with tetraspanin‑enriched microdomains, lipid rafts, or early endosomes.
ELISA 1:1000 – 1:5000 Cell culture supernatants, serum, plasma, tissue extracts Coating or detection antibody in sandwich ELISA; linear range typically 0.1–10 ng/mL when paired with a matched capture antibody.
Flow cytometry 1:100 – 1:500 Live or fixed cells, peripheral blood mononuclear cells (PBMCs) Surface staining of B cells, T cells, dendritic cells, and hepatoma cells; appropriate isotype control required.
Immunoprecipitation (IP) 1:50 – 1:100 Cell lysates, membrane extracts Efficient pull‑down of native CD81 and its interacting partners (CD19, integrins, HCV E2).
Five Cutting‑Edge Research Areas Where Precise CD81 Detection Is Non‑Negotiable
Research Context Why CD81 Measurement Matters How ABP0138 Enables Insights
HCV entry and antiviral drug discovery CD81 is the primary co‑receptor for hepatitis C virus; blocking CD81‑E2 interaction is a validated antiviral strategy . Western blot and flow cytometry with ABP0138 can monitor CD81 surface expression in hepatoma cells before/after treatment with entry inhibitors (e.g., anti‑CD81 antibodies, small‑molecule blockers).
Cancer metastasis and therapeutic resistance CD81 promotes integrin‑mediated invasion, EMT, and exosome‑mediated communication in triple‑negative breast, colorectal, and liver cancers . IHC‑F on tumor microarrays quantifies CD81 expression levels, correlating with clinical stage, metastasis, and patient survival.
B‑cell and T‑cell immunology CD81 forms the CD19‑CD21‑CD81 co‑receptor complex that amplifies B‑cell receptor signaling; its loss leads to immunodeficiency . Flow cytometry with ABP0138 identifies CD81+ B‑cell subsets in PBMCs; co‑immunoprecipitation validates CD81‑CD19 interactions.
Exosome biology and biomarker discovery CD81 is one of the most enriched proteins on exosome surfaces, used as a marker for extracellular vesicle isolation and characterization . Western blot of exosome pellets confirms CD81 enrichment; immuno‑EM or nanoparticle tracking analysis coupled with ABP0138 labeling validates exosome identity.
Muscle development and regeneration CD81 promotes myoblast fusion and myotube maintenance; its absence impairs muscle regeneration in mouse models . IF on differentiating myoblasts visualizes CD81 localization at fusion sites; WB tracks CD81 expression during myogenesis.
Step‑by‑Step Protocols: Detecting CD81 in Western Blot, IHC, and Immunofluorescence with ABP0138
Western Blot (WB)
- Sample preparation: Lyse cells or tissues in RIPA buffer (with protease inhibitors). For membrane‑enriched fractions, use a detergent‑based membrane extraction kit. Determine protein concentration via BCA assay. Load 20–40 µg of total protein per lane on a 12% SDS‑PAGE gel.
- Transfer: Transfer to PVDF membrane at 100 V for 90 minutes in ice‑cold transfer buffer.
- Blocking: Block membrane with 5% BSA in TBST for 1 hour at room temperature.
- Primary antibody incubation: Dilute ABP0138 1:1000 in blocking buffer; incubate membrane overnight at 4°C with gentle shaking.
- Washing: Wash membrane 3 × 10 minutes with TBST.
- Secondary antibody incubation: Incubate with HRP‑conjugated anti‑rabbit IgG (1:5000) for 1 hour at room temperature.
- Detection: Develop using ECL substrate and image with a chemiluminescence system. Expected band: ~25‑26 kDa (non‑glycosylated); higher bands may indicate glycosylation or dimers.
Immunohistochemistry (IHC‑F) on FFPE Tissues
- Deparaffinization: Bake sections at 60°C for 30 minutes, then deparaffinize in xylene and graded ethanol.
- Antigen retrieval: Perform heat‑induced epitope retrieval (HIER) in citrate buffer (pH 6.0) at 95°C for 20 minutes.
- Blocking: Block endogenous peroxidase with 3% H₂O₂, then block non‑specific sites with 5% normal goat serum.
- Primary antibody: Apply ABP0138 (1:100 dilution) overnight at 4°C.
- Secondary antibody: Apply HRP‑conjugated anti‑rabbit IgG for 1 hour at room temperature.
- Detection: Develop with DAB substrate, counterstain with hematoxylin, and mount. CD81 staining should appear as a crisp membrane signal on hepatocytes, lymphocytes, or tumor cells.
Immunofluorescence (IF) on Cultured Cells
- Fixation: Fix cells with 4% paraformaldehyde for 15 minutes at room temperature.
- Permeabilization: Permeabilize with 0.1% Triton X‑100 in PBS for 10 minutes (optional for surface staining only).
- Blocking: Block with 5% BSA in PBS for 1 hour.
- Primary antibody: Apply ABP0138 (1:200 dilution) overnight at 4°C.
- Secondary antibody: Apply fluorophore‑conjugated anti‑rabbit IgG (e.g., Alexa Fluor 488, 1:500) for 1 hour at room temperature.
- Mounting: Mount with DAPI‑containing mounting medium and image using a confocal microscope. CD81 typically shows punctate membrane staining, often co‑localizing with tetraspanin web components.
Five Common Pitfalls in CD81 Detection – And How ABP0138 Helps You Avoid Them
Pitfall Consequence Solution with ABP0138
Cross‑reactivity with CD9, CD63, or CD151 False‑positive signals in Western blot or IHC, leading to mis‑interpretation of CD81 expression. ABP0138 is affinity‑purified against human CD81 and shows negligible cross‑reactivity with other tetraspanins .
Weak or no signal in Western blot CD81 is a low‑abundance membrane protein; typical loads (20 µg) may yield faint bands. Use higher sample loads (30–40 µg), prolonged ECL exposure, or membrane‑enriched fractions; ABP0138’s polyclonal nature enhances sensitivity.
High background in IHC/IF Non‑specific staining in tissues or cells, obscuring true membrane localization. Optimize antigen‑retrieval conditions (citrate pH 6.0 vs. Tris‑EDTA pH 9.0) and increase blocking time; ABP0138 produces clean membrane‑specific staining.
Failure to detect glycosylated forms CD81 can be N‑glycosylated, shifting its apparent molecular weight to ~30‑35 kDa; some antibodies only recognize the non‑glycosylated form. ABP0138 recognizes both glycosylated and non‑glycosylated CD81; deglycosylation with PNGase F can confirm identity.
Lot‑to‑lot variability Inconsistent results when switching antibody batches, disrupting longitudinal studies. Each batch of ABP0138 is QC‑tested on CD81‑positive cell lines and comes with a certificate of analysis ensuring consistent performance.
Why Choose a Polyclonal Antibody for CD81 Detection Over a Monoclonal?
① Polyclonal antibodies recognize multiple epitopes, increasing the chance of detecting CD81 even when some epitopes are masked by protein‑protein interactions or post‑translational modifications.
CD81 exists in complexes with integrins, CD19, and other tetraspanins; a polyclonal pool increases the likelihood of binding accessible epitopes, especially in native IP or flow cytometry experiments .
② Polyclonal antibodies often provide higher sensitivity in Western blot and IHC because they recruit multiple secondary antibodies, amplifying the signal.
For low‑abundance targets like CD81 (especially in non‑hematopoietic tissues), the signal amplification offered by polyclonal antibodies can be decisive, reducing the need for excessive sample loads .
③ Polyclonal antibodies are less prone to complete detection failure due to epitope loss – a risk with monoclonal antibodies if the single epitope is altered by fixation, denaturation, or genetic polymorphism.
In FFPE tissues (IHC) or reduced/denatured samples (WB), conformational epitopes may be destroyed; polyclonal antibodies, targeting both linear and conformational epitopes, offer a safety net .
④ ABP0138 is validated for multiple applications (WB, IHC, IF, ELISA), allowing you to use the same antibody across different experimental workflows, saving time and reducing cross‑validation efforts.
Many monoclonal antibodies are optimized for a single application (e.g., flow cytometry only); ABP0138’s multi‑application validation means you can seamlessly transition from Western blot to immunofluorescence without switching reagents .
⑤ The rabbit host minimizes interference with endogenous immunoglobulins in human samples, reducing background in IHC and flow cytometry.
Mouse‑derived monoclonal antibodies can bind human anti‑mouse antibodies (HAMA) present in serum or tissues, causing false‑positive signals; rabbit polyclonals like ABP0138 circumvent this issue .
Three Critical Validation Steps Before You Trust Your CD81 Data
Step Purpose How to Perform with ABP0138
Specificity verification Confirm that the ~25‑26 kDa band in WB is indeed CD81, not a cross‑reacting protein. Perform siRNA‑mediated CD81 knockdown in a positive‑control cell line (e.g., Huh‑7); the band should disappear or diminish. Alternatively, pre‑absorb the antibody with recombinant CD81 protein – signal should be abolished.
Subcellular localization confirmation Ensure that the antibody correctly labels membrane‑localized CD81, not cytoplasmic artifacts. Co‑stain with membrane markers (e.g., Na⁺/K⁺ ATPase) in IF; CD81 signal should co‑localize with the membrane marker. In IHC, membrane‑specific staining should be evident on hepatocytes or lymphocytes.
Cross‑reactivity profiling Rule out binding to other tetraspanins (CD9, CD63, CD151) or unrelated membrane proteins. Run Western blot with lysates from cells overexpressing CD9, CD63, CD151; ABP0138 should show no band at the corresponding molecular weights (~22‑30 kDa).
From Bench to Bedside: How CD81 Detection with ABP0138 Informs Therapeutic Development
① Screening anti‑HCV entry inhibitors that target the CD81‑E2 interaction.
ELISA with ABP0138 as a detection antibody can measure blockade of CD81‑E2 binding by candidate compounds or neutralizing antibodies . High‑throughput flow cytometry using ABP0138 can quantify CD81 surface expression in hepatoma cells treated with entry inhibitors.
② Stratifying cancer patients based on CD81 expression for targeted therapy.
IHC with ABP0138 on tumor microarrays can identify CD81‑high tumors that may be more aggressive or metastatic; CD81 expression may predict response to integrin‑targeted therapies or exosome‑based interventions .
③ Monitoring B‑cell malignancies and immunodeficiencies.
Flow cytometry with ABP0138 on peripheral blood or lymph node biopsies can assess CD81 expression on B‑cell subsets, aiding in the diagnosis of CD81‑deficient immunodeficiencies or tracking CD81 modulation during immunotherapy .
④ Validating exosome isolation protocols and characterizing extracellular vesicles.
Western blot with ABP0138 on exosome pellets confirms the presence of CD81 as a positive exosome marker; combined with negative markers (calnexin, GM130), it ensures purity of isolated vesicles .
⑤ Investigating muscle regeneration and muscular dystrophies.
Immunofluorescence with ABP0138 on muscle sections can visualize CD81 at myoblast fusion sites, providing insights into muscle repair mechanisms and potential therapeutic targets for muscle wasting disorders .
A Ready‑to‑Use Methods Paragraph for Your Paper
CD81 expression was analyzed using the Abbkine CD81 Polyclonal Antibody (ABP0138). For Western blot, cells were lysed in RIPA buffer (Thermo Fisher) containing protease inhibitors. Total protein (30 µg per lane) was separated on a 12% SDS‑PAGE gel and transferred to a PVDF membrane. The membrane was blocked with 5% BSA in TBST for 1 hour, then incubated with anti‑CD81 antibody (ABP0138, 1:1000 dilution) overnight at 4°C. After washing, the membrane was incubated with HRP‑conjugated anti‑rabbit secondary antibody (1:5000) for 1 hour at room temperature. Signals were detected using ECL substrate (Bio‑Rad) and quantified with ImageLab software. For immunofluorescence, cells were fixed with 4% paraformaldehyde, permeabilized with 0.1% Triton X‑100, blocked with 5% BSA, and incubated with ABP0138 (1:200) overnight at 4°C. After washing, cells were incubated with Alexa Fluor 488‑conjugated anti‑rabbit IgG (1:500) for 1 hour, counterstained with DAPI, and imaged using a confocal microscope. For flow cytometry, live cells were stained with ABP0138 (1:200) for 1 hour on ice, followed by FITC‑conjugated anti‑rabbit IgG (1:500), and analyzed on a BD FACSCanto II.
The Five Bench Rules for Reliable CD81 Detection with ABP0138
Rule Rationale
Always include a positive control (Huh‑7 hepatoma cells, Raji B cells, or CD81‑overexpressing HEK293 cells) and a negative control (CD81‑knockdown or knockout cells) Verifies antibody functionality and assay sensitivity; confirms that the ~25 kDa band is CD81‑specific.
For WB, use fresh samples and avoid repeated freeze‑thaw cycles CD81 is prone to degradation; aliquot lysates and store at –80°C; thaw on ice only once.
In IHC, optimize antigen‑retrieval time and pH Over‑retrieval can destroy epitopes; under‑retrieval yields weak staining. Test citrate (pH 6.0) vs. Tris‑EDTA (pH 9.0) buffers.
For flow cytometry, titrate the antibody to determine optimal dilution Too high concentration increases background; too low reduces signal. Start with 1:200 and adjust based on cell type.
Include a recombinant CD81 standard curve in every ELISA run Corrects for inter‑assay variability; ensures quantitative accuracy.
Use low‑binding tubes for sample storage and handling CD81 adsorbs to plastic; siliconized or low‑binding tubes reduce protein loss.
When performing multiplex IHC/IF, validate antibody compatibility Ensure secondary antibodies are species‑specific and fluorophore combinations do not bleed‑through.
For longitudinal studies, use the same antibody lot throughout Lot‑to‑lot variations, though minimal with ABP0138, can affect signal intensity.
Always run samples in duplicate or triplicate Improves statistical reliability, especially for low‑abundance CD81 measurements.
Document antibody dilution, incubation times, and detection conditions Ensures reproducibility across experiments and lab members.
Explore the Abbkine CD81 Polyclonal Antibody (ABP0138) – with high specificity for human CD81, validated for WB, IHC, IF, and ELISA, and backed by rigorous QC – for your next virology, immunology, cancer, or exosome study.
🔗 Product reference: ABP0138 (Abbkine) – https://www.abbkine.com/product/cd81-polyclonal-antibody-abp0138/
(For research use only. Not for diagnostic or therapeutic procedures. Store at –20°C; avoid repeated freeze‑thaw cycles; use within 12 months of receipt.)





