




TMED9: The Unseen Orchestrator of ER‑to‑Golgi Traffic – Why Quantifying This Cargo Receptor with Abbkine's ELISA Kit (KTE60300) Is Key to Understanding Proteinopathies
Transmembrane emp24 domain‑containing protein 9 (TMED9) — a 25 kDa type‑I integral membrane glycoprotein belonging to the conserved p24 family — is not merely a passive component of the early secretory pathway; it is the critical cargo receptor that decides which newly synthesized proteins proceed from the endoplasmic reticulum (ER) to the Golgi, which are retrieved back, and which misfolded clients are entrapped in a toxic limbo, with its dysregulation directly linked to Mucin‑1 kidney disease, neurodegenerative proteinopathies, and cancer progression . Yet, when you attempt to measure TMED9 levels in cell lysates, tissue homogenates, or patient serum using Western blot or conventional immunoassays, you face low abundance, poor antibody specificity, and the challenge of distinguishing membrane‑bound from soluble pools. The Abbkine Human Transmembrane emp24 domain‑containing protein 9 (TMED9) ELISA Kit (KTE60300) overcomes these hurdles with a sandwich ELISA format that detects human TMED9 with <0.188 ng/mL sensitivity, a dynamic range of 0.313–20 ng/mL, and no cross‑reactivity with other TMED family members — enabling precise, high‑throughput quantification of this elusive trafficking regulator without membrane fractionation, tedious sample preparation, or compromised specificity .
TMED9 Is Not Just Another Golgi Protein — It's the Quality‑Control Sentinel That Recognizes Misfolded Cargo, Recruits COPI/COPII Coatomers, and Maintains ER‑Golgi Homeostasis, with Its Oligomerization Driving Cytotoxic Protein Entrapment in Diseases Like MKD and Alzheimer's
TMED9 (also known as p25, GMP25, or p24‑alpha‑2), encoded by the TMED9 gene on chromosome 5q35.3, functions as a key component of the p24 heterooligomeric complex that shuttles between the ER, ER‑Golgi intermediate compartment (ERGIC), and cis‑Golgi . Its domain architecture — an N‑terminal signal sequence, a luminal Golgi‑dynamics (GOLD) domain for cargo recognition, a coiled‑coil domain for oligomerization, a single transmembrane domain, and a cytoplasmic tail containing dilysine (KK) and diphenylalanine (FF) motifs for COPI/COPII binding — enables it to act as a bidirectional trafficking receptor . In normal physiology, TMED9 facilitates anterograde transport of correctly folded proteins via COPII vesicles and retrograde retrieval of escaped ER residents via COPI vesicles, while also participating in Golgi organization and ER‑exit‑site formation . However, recent cryo‑EM studies reveal that TMED9 can self‑oligomerize into octamers and dodecamers, a property that allows it to entrap misfolded proteins like frameshifted Mucin‑1 (MUC1‑fs) in the early secretory pathway, leading to toxic aggregates that drive Mucin‑1 kidney disease (MKD) . Beyond MKD, TMED9‑mediated misfolded‑protein retention is implicated in neurodegenerative disorders (Alzheimer's, Parkinson's) and cancers where secretory pathway overload occurs . Quantifying TMED9 levels thus provides a window into cellular protein‑quality‑control efficiency, ER‑stress responses, and disease‑associated trafficking defects .
Why Western Blots and Generic Immunoassays Fail to Capture TMED9 Dynamics — And How the Abbkine ELISA Kit (KTE60300) Delivers Specific, Sensitive, and Reproducible Quantification in Complex Biological Matrices
The Abbkine Human TMED9 ELISA Kit (KTE60300) is a colorimetric sandwich ELISA designed for the in‑vitro quantitative measurement of human TMED9 in tissue homogenates, cell lysates, serum, plasma, and other biological fluids . The assay employs a pre‑coated monoclonal anti‑TMED9 capture antibody that binds TMED9 from samples; after washing, a biotin‑conjugated detection antibody binds a different epitope on the captured TMED9; then streptavidin‑HRP and TMB substrate are added to generate a color signal proportional to TMED9 concentration, measured at 450 nm . Unlike Western blotting, which suffers from semi‑quantitative results, high sample‑volume requirements, and inability to process many samples in parallel, this ELISA kit offers true quantification, high throughput (96‑well format), and a sensitivity of <0.188 ng/mL — critical because TMED9 is a low‑abundance membrane protein often expressed at ng/mL levels in biological samples . Moreover, the kit's matched antibody pair shows no significant cross‑reactivity with TMED2, TMED10, or other TMED family members, ensuring specificity for TMED9 even in samples containing related p24 proteins .
Challenge in TMED9 Detection Limitation of Conventional Methods How KTE60300 Addresses It
Low abundance TMED9 is a membrane protein with low copy numbers; Western blot may fail to detect it without overexposure or large sample loads Sensitivity <0.188 ng/mL enables detection of TMED9 in normal tissue lysates and cell supernatants without amplification .
Membrane localization TMED9 resides in ER, ERGIC, and Golgi membranes; extraction requires detergent‑based lysis, which can interfere with immunoassays The kit is validated for tissue homogenates and cell lysates prepared with mild detergents (e.g., RIPA buffer); the assay buffer minimizes detergent interference.
Cross‑reactivity with other p24 proteins Polyclonal antibodies often recognize conserved epitopes shared among TMED family members (TMED2, TMED10, etc.) Uses monoclonal antibodies selected for TMED9‑specific epitopes; cross‑reactivity testing shows no detectable binding to TMED2, TMED10, or other analogues .
Sample‑to‑sample variability Differences in lysis efficiency, protein extraction, and membrane enrichment lead to inconsistent results The kit includes a lyophilized TMED9 standard for generating a calibration curve (0.313–20 ng/mL); samples are diluted to fall within the linear range, normalizing variability.
Throughput limitations Western blotting is low‑throughput, unsuitable for screening large sample sets (e.g., clinical cohorts, drug‑treated cells) 96‑well plate format allows simultaneous processing of up to 40 samples in duplicate within ~4.5 hours, ideal for high‑throughput studies.
Quantification accuracy Western blot band densitometry is semi‑quantitative and prone to saturation errors Colorimetric readout with a 4‑parameter logistic (4PL) standard curve provides precise concentration values (ng/mL) with intra‑assay CV <8% and inter‑assay CV <10% .
Sample type flexibility Many assays are optimized only for cell lysates, not for serum/plasma or tissue homogenates Validated for serum, plasma, tissue homogenates, and cell culture supernatants; includes sample diluent to reduce matrix effects in complex fluids.
The kit is supplied as a complete set containing pre‑coated 96‑well microplate, TMED9 standard, biotin‑labeled detection antibody, streptavidin‑HRP, TMB substrate, stop solution, wash buffer, and assay diluent, stored at 4°C (lyophilized standard at ‑20°C). The 6‑month shelf life and ready‑to‑use reagents make it suitable for both routine lab use and large‑scale screening projects .
From Sample to Data in 4.5 Hours: The Step‑by‑Step Protocol That Turns TMED9 Quantification into a Routine Assay
- Sample Preparation
• Cell lysates: Harvest cells, wash with PBS, lyse in RIPA buffer (with protease inhibitors) on ice for 30 minutes. Centrifuge at 12,000 × g for 15 min at 4°C; collect supernatant; determine protein concentration (e.g., BCA assay). Dilute lysates with assay diluent to a total protein concentration of 1–2 mg/mL (or as optimized).
• Tissue homogenates: Homogenize 50–100 mg of fresh or frozen tissue in 1 mL of cold PBS or RIPA buffer using a tissue homogenizer. Centrifuge at 5000 × g for 10 min; collect supernatant; dilute as needed.
• Serum/plasma: Collect blood in serum separator tubes or EDTA/heparin tubes; separate by centrifugation at 1000 × g for 20 min. Aliquot and store at ‑80°C; avoid repeated freeze‑thaw cycles. Dilute 1:2 to 1:10 with assay diluent before assay.
- Reagent Preparation
• Bring all reagents to room temperature (30 min before assay).
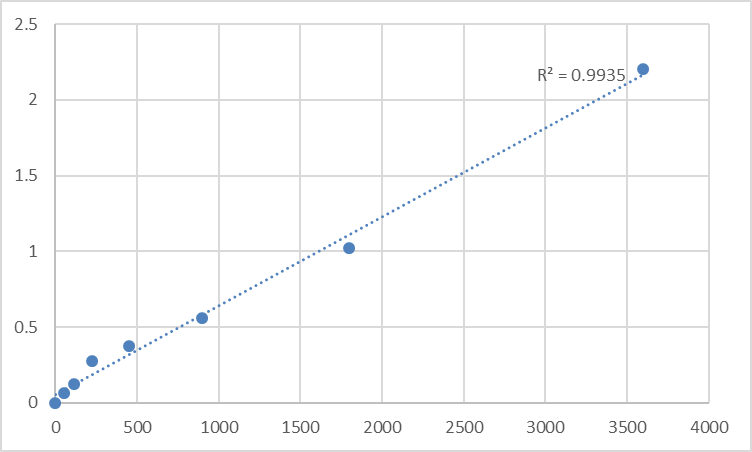
• Reconstitute the lyophilized TMED9 standard with 1.0 mL of assay diluent to generate a stock solution (e.g., 20 ng/mL). Perform serial 1:2 dilutions to create a 7‑point standard curve (20, 10, 5, 2.5, 1.25, 0.625, 0.313 ng/mL). Include a zero standard (assay diluent only).
• Prepare 1× wash buffer by diluting the 20× concentrate with distilled water.
• Prepare working detection antibody and streptavidin‑HRP solutions according to the kit instructions.
- Assay Procedure
• Add 100 µL of standard or diluted sample to each well of the pre‑coated plate. Cover with plate sealer; incubate at 37°C for 90 minutes.
• Discard liquid; wash each well 4 times with 300 µL of 1× wash buffer (soak for 30 seconds per wash).
• Add 100 µL of biotin‑labeled detection antibody to each well. Cover; incubate at 37°C for 60 minutes.
• Wash 4 times as above.
• Add 100 µL of streptavidin‑HRP to each well. Cover; incubate at 37°C for 30 minutes.
• Wash 4 times.
• Add 100 µL of TMB substrate to each well. Incubate in the dark at room temperature for 15–30 minutes (until blue color develops).
• Add 50 µL of stop solution to each well; gently tap plate to mix. Read absorbance at 450 nm within 30 minutes.
- Data Analysis
• Subtract the average absorbance of the zero standard from all readings.
• Plot standard curve using log TMED9 concentration vs. absorbance; fit a 4‑parameter logistic (4PL) curve.
• Interpolate sample concentrations from the curve.
• Multiply by the dilution factor to obtain the original concentration (ng/mL or ng/mg protein).
Critical Notes
• Avoid hemolyzed or lipemic serum/plasma samples, as they may interfere.
• For tissue samples, include a protein‑content normalization (e.g., express as ng TMED9/mg total protein).
• Run samples in duplicate and include a quality‑control sample (e.g., a pooled cell lysate) to monitor inter‑assay precision.
• The linear range is 0.313–20 ng/mL; samples with higher concentrations should be further diluted.
Where TMED9 Quantification Becomes Indispensable: From Basic Trafficking Studies to Clinical Biomarker Discovery
Research Area Why TMED9 Measurement Matters Typical Sample Types
Secretory pathway & protein trafficking TMED9 is essential for COPII‑mediated anterograde transport and COPI‑mediated retrograde retrieval; its levels correlate with ER‑exit‑site formation and Golgi integrity . Cell lysates (HeLa, HEK293, COS‑7), tissue homogenates (liver, kidney), subcellular fractions (ER, Golgi).
Protein‑quality‑control & ER‑stress TMED9 oligomerization entraps misfolded proteins (e.g., MUC1‑fs, mutant CFTR) in the early secretory pathway; quantifying TMED9 helps assess ER‑stress response and clearance efficiency . Cell lysates from ER‑stress‑induced models (tunicamycin, thapsigargin treatment), patient‑derived fibroblasts.
Mucin‑1 kidney disease (MKD) TMED9 is required for MUC1‑fs entrapment in cis‑Golgi/COPI compartments; TMED9 levels may serve as a biomarker for disease progression or therapeutic response . Patient serum, urine, kidney biopsy homogenates.
Neurodegenerative proteinopathies TMED9‑mediated retention of misfolded α‑synuclein, tau, or Aβ could contribute to Parkinson's and Alzheimer's pathology; TMED9 quantification in CSF or brain tissue may inform disease mechanisms. Cerebrospinal fluid (CSF), post‑mortem brain homogenates, neuronal cell lysates.
Cancer biology TMED9 regulates Wnt signaling receptor trafficking and growth‑factor receptor localization; altered TMED9 expression is reported in breast, colorectal, and pancreatic cancers . Tumor tissue lysates, cancer cell lines (MCF‑7, SW480, PANC‑1), patient serum.
Drug screening & target validation Small‑molecule inhibitors of TMED9 (e.g., BRD4780) are being explored for MKD and other proteinopathies; ELISA enables pharmacodynamic monitoring of TMED9 modulation . Cell lysates from compound‑treated cultures, animal tissue homogenates.
Golgi organization & membrane dynamics TMED9 depletion disrupts Golgi structure and COPI recruitment; measuring TMED9 helps study Golgi fragmentation in trafficking mutants or disease models . Cell lysates from siRNA‑ or CRISPR‑mediated TMED9 knockdown/knockout lines.
Unconventional protein secretion (UPS) TMED9 participates in ER‑to‑plasma‑ membrane UPS of CFTR and SARS‑CoV‑2 spike protein during ER stress; quantification assesses UPS pathway activity . Cell culture supernatants, membrane fractions, stress‑induced cell lysates.
A Ready‑to‑Use Methods Paragraph for Your Paper
TMED9 protein levels were quantified using the Abbkine Human Transmembrane emp24 domain‑containing protein 9 (TMED9) ELISA Kit (KTE60300) following the manufacturer's protocol. Briefly, cell lysates (prepared in RIPA buffer with protease inhibitors) or recombinant TMED9 standard (0.313–20 ng/mL) were added to a pre‑coated 96‑well plate (100 µL/well) and incubated at 37°C for 90 minutes. After washing, 100 µL of biotin‑labeled detection antibody was added and incubated at 37°C for 60 minutes. Following another wash, 100 µL of streptavidin‑HRP was added and incubated at 37°C for 30 minutes. After a final wash, 100 µL of TMB substrate was added and incubated in the dark for 20 minutes. The reaction was stopped with 50 µL of stop solution, and absorbance was measured at 450 nm using a microplate reader (Bio‑Rad iMark). TMED9 concentration was determined by interpolating from a 4‑parameter logistic standard curve. All samples were assayed in duplicate, and the intra‑assay coefficient of variation (CV) was <10%.
The Five Bench Rules That Ensure Reliable TMED9 ELISA Results
Rule Rationale
Always include a fresh standard curve in every run (7 points in duplicate) TMED9 standard is lyophilized; reconstituted standard degrades over time. Never reuse curves from previous assays.
Read absorbance within 30 minutes after adding stop solution The yellow color may fade or precipitate, leading to inaccurate OD readings.
Store samples at –80°C and avoid repeated freeze‑thaw cycles TMED9 is a membrane protein prone to degradation; aliquot samples to minimize freeze‑thaw.
Include a sample blank (assay diluent) and a negative control (untransfected cell lysate) Correct for background absorbance and non‑specific binding.
Optimize sample dilution to ensure readings fall within 0.313–20 ng/mL Samples with TMED9 >20 ng/mL may require further dilution to avoid the hook effect.
Use low‑binding tubes and tips for sample handling TMED9 may adsorb to plastic surfaces; siliconized or low‑binding consumables minimize loss.
For tissue samples, normalize to total protein content Express results as ng TMED9/mg total protein to account for extraction efficiency differences.
Avoid hemolyzed serum/plasma samples Hemolysis releases proteases and hemoglobin that can interfere with antibody binding.
Bring all reagents to room temperature before use Temperature fluctuations affect antibody‑antigen binding kinetics and enzymatic reaction rates.
Include a quality‑control sample (e.g., pooled cell lysate) in each plate Monitor inter‑assay precision and detect systematic drift.
What Changes When You Switch from Western Blot to the Abbkine TMED9 ELISA Kit
① You move from semi‑quantitative band densitometry to absolute quantification (ng/mL), because the ELISA provides a calibrated standard curve that translates absorbance into precise concentration values.
Western blotting only gives relative band intensity; the ELISA's lyophilized recombinant TMED9 standard enables absolute quantification, critical for comparing TMED9 levels across samples, time points, or treatment groups .
② You can process 40+ samples in duplicate in under 5 hours, instead of spending days running multiple gels, transferring, blocking, and developing blots.
The 96‑well plate format and streamlined protocol allow high‑throughput screening of drug‑treated cells, patient cohorts, or time‑course experiments that would be impractical with Western blotting.
③ You eliminate cross‑reactivity worries with other p24 family members, as the kit's monoclonal antibody pair is rigorously validated for TMED9 specificity.
Many commercial TMED9 antibodies cross‑react with TMED2, TMED10, or other EMP24‑family proteins; the Abbkine kit shows no detectable cross‑reactivity, ensuring you measure TMED9, not its homologs .
④ You gain sensitivity down to 0.188 ng/mL, enabling detection of TMED9 in low‑abundance samples like serum or primary cell lysates where Western blot often fails.
TMED9 is a low‑copy‑number membrane protein; the ELISA's signal amplification (biotin‑streptavidin‑HRP) and optimized buffers detect TMED9 at concentrations below 0.2 ng/mL, whereas Western blot may require 10–20 µg of total protein per lane and still yield faint bands.
⑤ Your data become reproducible across operators and labs, thanks to pre‑coated plates, lyophilized standards, and standardized reagents that minimize batch‑to‑batch variability.
Inter‑lab variability in Western blotting arises from different transfer efficiencies, antibody lots, and detection methods; the ELISA kit provides QC‑tested, pre‑coated plates and calibrated standards with inter‑assay CV <10% .
Three Common Pitfalls in TMED9 ELISA — And How to Avoid Them
Pitfall Consequence Solution
Incomplete cell/tissue lysis TMED9 remains membrane‑bound and under‑represented in the lysate, leading to underestimation. Use RIPA buffer with 1% Triton X‑100 or NP‑40; incubate on ice for 30 minutes with occasional vortexing; centrifuge at 12,000 × g for 15 min to remove debris.
Over‑dilution or under‑dilution of samples Absorbance falls outside the standard curve range (below 0.313 ng/mL or above 20 ng/mL), requiring re‑assay. Perform a pilot dilution series (e.g., 1:2, 1:5, 1:10) to identify the optimal dilution that places samples in the middle of the curve (2–10 ng/mL).
Inconsistent washing High background or low signal‑to‑noise ratio due to residual unbound reagents. Use an automated plate washer set to 350 µL/well for 4 washes; if washing manually, ensure each well is filled completely and aspirated thoroughly.
Prolonged TMB incubation Over‑development leads to saturation (OD >2.5) and non‑linear response. Monitor color development after 15 minutes; stop the reaction when the highest standard turns deep blue (typically 20–25 minutes).
Using hemolyzed or lipemic serum Hemoglobin or lipids interfere with antibody binding, causing false‑high or false‑low results. Centrifuge blood samples promptly; avoid hemolysis; for lipemic samples, consider ultracentrifugation or lipid removal columns before assay.
Skipping the protein‑content normalization for tissue/cell lysates Results cannot be compared across samples with different extraction efficiencies. Measure total protein concentration (BCA, Bradford) and express TMED9 as ng/mg total protein.
Storing reconstituted standard at 4°C for >1 week Standard degradation leads to inaccurate calibration. Aliquot reconstituted standard and store at ‑80°C; use each aliquot only once.
Explore the Abbkine Human Transmembrane emp24 domain‑containing protein 9 (TMED9) ELISA Kit (KTE60300) — with sensitivity <0.188 ng/mL, no cross‑reactivity, and validated for serum, plasma, tissue homogenates, and cell lysates — for your next trafficking, protein‑quality‑control, or biomarker study.
🔗 Product reference: KTE60300 (Abbkine)
(For research use only. Not for diagnostic or therapeutic procedures. Store at 4°C; bring reagents to room temperature before use; avoid repeated freeze‑thaw cycles; run a fresh standard curve with each assay.)





