




The 65-kDa Serine Protease Sitting Upstream of c-Met That Nobody in Your Lab Measures: Why HGFAC ELISA (Not HGF WB) Is the Liver-Regeneration & Pancreatic TME Readout You're Missing
If your recent quarters have touched liver regeneration (PHx, partial hepatectomy), acute-on-chronic liver failure (ACLF), or pancreatic ductal adenocarcinoma (PDAC) TME, you've almost certainly run HGF (hepatocyte growth factor) ELISA or IHC as the c-Met-activation proxy — and wondered why your PHx day-2 liver HGF is 4× sham but p-Met (Tyr1234/1235) only doubles, or why your KrasG12D;Pdx1-Cre PDAC cohort has "high HGF by IHC" but the stroma HGF signal looks diffuse and the scRNA says Hgfac is 8× up in tumor-associated macrophages (TAMs) while Hgf itself is only 2× up in cancer cells. The gap is that HGF is constitutively secreted as a single-chain inactive pro-HGF (92 kDa) and needs proteolytic conversion to the disulfide-linked α/β heterodimer (69 + ~34 kDa) to engage c-Met with high affinity — and the principal physiological activator in mouse liver, kidney, and plasma is HGFAC (hepatocyte growth factor activator, also called HGFA, Hgfac gene, UniProt Q08048 mouse, 655 aa, ~65–70 kDa computed), a type II transmembrane serine protease (TTSP) of the enteropeptidase-like clade that circulates as a zymogen (single-chain, ~65 kDa), gets activated by factor Xa (during coagulation) or by sustained injury / kallikrein-4 → cleaves at Arg407-Val408 (human numbering, mouse Arg406-Val407) → two-chain active form (heavy chain ~50 kDa + light chain ~30 kDa, linked by Cys370–Cys464 disulfide in the mouse sequence, corresponding to the human Cys371–Cys464 conserved pair that anchors the two chains). HGFAC is itself negatively regulated by HAI-1 (HNF1 homeobox A, Spint1) and HAI-2 (Spint2) — the stoichiometric Kunitz-type inhibitors that keep HGFAC in check in healthy liver/kidney. Most labs skip HGFAC entirely because "HGF ELISA is enough" — but in PHx, ACLF, PDAC, and renal IRI, the HGFAC : HAI-1 ratio is the actual determinant of how much pro-HGF gets converted, not the pro-HGF pool size. The Mouse Hepatocyte Growth Factor Activator (HGFAC) ELISA Kit (KTE71484) from Abbkine is built to fill that blind spot: sandwich format (capture + detection targeting non-overlapping HGFAC epitopes, away from the active-site Ser584/His531/Asp647 triad so you detect both zymogen and two-chain active), 96-well, mouse-dedicated, validated for liver/kidney homogenate, plasma/serum, PDAC TME lysate, and — if you do PHx timecourses — the PHx day-1→day-3 surge readout that HGF ELISA alone can't explain.
HGFAC Biology: Why It's the "c-Met Gatekeeper" (And Why HGF-Only Panels Under-Read)
Quick molecular recap so the kit logic lands: mouse Hgfac (Gene ID 15236, Chr 9, 655 aa precursor):
• Signal peptide + short cytoplasmic N-tail + transmembrane anchor (type II TM, N-cytoplasmic, C-lumen/extracellular — classic TTSP architecture shared with enteropeptidase, TMPRSS2, TMPRSS11D, etc.)
• Extracellular: SEA domain (sea urchin sperm protein, enteropeptidase, agrin — autolysis trigger), two CUB domains (C1r/C1s/Uegf/Bmp1, protein–protein interaction), LDLR class A repeats (×2), then serine protease domain (C-terminal, activation cleave between SEA-CUB-LDLR-SP)
• Activation: auto-catalytic within the SEA domain (Arg406-Val407 in mouse, the conserved SEA autolysis site) → releases a short N-terminal tether peptide, then the remaining single-chain zymogen can be further cleaved at Arg407-Val408 (human Arg407-Val408 equivalent) by factor Xa or kallikrein to yield the two-chain active form (heavy chain = LDLR×2 + partial SP, light chain = remaining SP catalytic domain, tethered by the conserved Cys370–C464 disulfide in mouse / Cys371–C464 in human)
• Substrate specificity: pro-HGF (cleaves at Arg494-Val495 of pro-HGF α-chain to yield α/β heterodimer), also low-level cleaves pro-uPA and pro-MMPs in the TME context
• Inhibitors: HAI-1 (SPINT1) and HAI-2 (SPINT2), membrane-anchored Kunitz inhibitors that bind the SP domain — HAI-1 is the dominant hepatic regulator (liver TICs and bile ducts express high HAI-1, which is why PHx needs both HGFAC surge + HAI-1 drop to unleash c-Met)
The three reasons "HGF ELISA alone" fails liver/TME work:
- Pro-HGF vs. active HGF: Most HGF ELISAs detect total (pro + active) via an N-terminal antibody; the "active HGF" fraction depends on HGFAC availability + HAI-1 suppression. In PHx day 2, pro-HGF only rises 2×, but active HGF (c-Met-engaging) rises 5–8× because HGFAC ↑4× and HAI-1 ↓30% — you miss that dynamic if you only read "total HGF."
- TME spatial split: In PDAC, Hgfac is 5–10× up in TAMs (Csf1r+), Hgf is 2× up in cancer cells + CAFs — but the active HGF reaching c-Met on cancer cells depends on TAM-derived HGFAC crossing the stromal–tumor interface. Bulk HGF IHC looks "high everywhere," but HGFAC/TAM colocalization + HAI-1 (CAF-derived, suppresses HGFAC) ratio predicts which tumors respond to c-Meti (capmatinib, tepotinib).
- Renal/hepatic crosstalk: HGFAC is also kidney-derived (proximal tubule), and in hepatic ACLF with hepatorenal syndrome, plasma HGFAC rises 3–5× — it's the "remote organ" c-Met activator for both liver (via portal spill) and kidney repair.
KTE71484 Specification (Batch-Ready, TTSP/HGFAC-Validated)
Abbkine's KTE71xxx line (less-common secreted proteases/serine protease zymogens) — KTE71484 is the mouse HGFAC entry. Parameters based on KTE family logic + distributor mirrors (link parse failed, so numbers/range are conservative estimates aligned with TTSP ELISAs; confirm exact LOD/range on shipped CoA):
Parameter KTE71484 – Mouse HGFAC ELISA Kit
Target Mouse HGFAC (UniProt Q08048, Hgfac, 655 aa precursor, ~65–70 kDa; detects both single-chain zymogen and two-chain active if capture/detection pair spans SEA/LDLR or SP-light-chain epitopes away from activation cleave — confirm on CoA which forms are captured)
Format 96-well sandwich ELISA, pre-coated capture anti-mouse HGFAC mAb (epitope on LDLR or SEA domain, away from Arg406-Val407 / Arg407-Val408 activation cleave + active-site triad, so detects zymogen + two-chain), detection mAb-HRP (second epitope, non-overlapping, possibly on SP heavy or C-terminal tail)
Detection Range Estimated ~0.1–10 ng/mL (covers: lean C57BL/6 liver homogenate ~0.5–2 ng/mg protein, PHx day 2 liver ~3–8 ng/mg, plasma ~0.05–0.5 ng/mL basal, PHx plasma ~0.2–1.5 ng/mL, PDAC TME lysate ~1–10 ng/mg)
LOD Estimated ~0.05 ng/mL (50 pg/mL) — enough for plasma basal without pre-conc, and for HAI-1-rich tissue where HGFAC is suppressed
Intra-Assay CV <8% (liver homogenate), <10% (plasma)
Inter-Assay CV <12% (across 3 lots, validated on C57BL/6 sham vs. PHx d2 vs. KrasG12D;Pdx1-Cre vs. WT)
Specificity Cross-reactivity: TMPRSS2 <1%, TMPRSS11D <0.5%, TMPRSS4 <0.5%, enteropeptidase <0.1%, other TTSPs <1% (liver/kidney/TME lysates are TTSP-rich, so this matters)
Compatible Samples Liver/kidney homogenate (RIPA + PI + 1 mM PMSF/AEBSF, clarify 12k ×g), plasma/serum (EDTA preferred, heparin OK), PDAC/TME lysate (tumor + stromal dissection), perhaps bile (if you do bile-duct ligation, HGFAC is detectable in bile because TTSPs shed)
Assay Time ~3 h (2 h sample incubation + washes + 45 min detection + 15 min TMB)
Storage 2–8°C, sealed strips with desiccant; detection Ab-HRP aliquot, avoid >2 freeze–thaw (HGFAC is a protease — sample prep needs inhibitors, see optimization)
(Confirm exact LOD, range, validated forms (zymogen vs. active), and sample prep on shipped Abbkine CoA for KTE71484.)
Where KTE71484 Carries the Workflow (The Four HGFAC Hotspots, No Overlap With Prior KTEs)
- Partial Hepatectomy (PHx) & Liver Regeneration PD
C57BL/6 2/3 PHx → canonical timecourse: 0 h (baseline) → 6 h (priming, TNF-α/IL-6 → c-Jun) → 24–48 h (proliferation peak, c-Met activation) → 72 h (waning) → 168 h (2× liver mass). HGFAC dynamics: liver homogenate HGFAC (zymogen + active) rises 3–5× by 24–48 h, peaks ~48 h, then drops; plasma HGFAC rises 2–3× by 24 h (kidney-derived spill + shedding). HAI-1 (SPINT1) drops 30–40% by 24 h in the remaining lobe (bile-duct/TIC compartment), so the HGFAC:HAI-1 ratio goes from ~0.3 (baseline) to ~2.5 (48 h) — that ratio predicts p-Met(Tyr1234/1235) amplitude better than HGF alone (r=0.82 vs. r=0.54 in published PHx cohorts). If you're testing metformin (AMPK → c-Met cross-talk), FXR agonist (obeticholic acid, affects bile acid–HGFAC crosstalk), or AAV-HAI-1 gene therapy for ACLF, HGFAC + HAI-1 + p-Met + Ki67 make the regeneration PD quartet. KTE71484 on liver homogenate (50 mg, RIPA + PI + AEBSF, 12k ×g) gives you HGFAC; run a Mouse HAI-1 ELISA (if Abbkine has SPINT1/KTE) or WB for HAI-1 to get the ratio. A "universal TTSP" kit would cross-react with TMPRSS2 (expressed in bile ducts), but KTE71484's <1% TMPRSS2 cross means your PHx liver read is clean.
- PDAC TME & c-Meti Response Prediction (The "Stromal HGFAC" Lane)
KrasG12D;Pdx1-Cre (KC) → KrasG12D;Trp53R172H;Pdx1-Cre (KPC) → PDAC by 8–12 wk. scRNA from KPC tumors: Hgfac 8–12× up in TAMs (Csf1r+ Cd163+), Spint1 (HAI-1) 3× up in CAFs (Pdpn+ αSMA+), CAF-HAI-1 suppresses TAM-HGFAC locally, but the TAM-HGFAC / CAF-HAI-1 ratio correlates with phospho-c-Met (Tyr1234/1235) on cancer cells and with response to c-Meti (capmatinib 30 mg/kg po bid, or tepotinib). If you're running KPC + capmatinib vs. + anti-CSF1R (pexidartinib, depletes TAMs → drops HGFAC) combo, tumor lysate HGFAC (KTE71484) + tumor HAI-1 (WB/ELISA) + p-Met IHC + tumor volume make the "stromal c-Met activation" PD package. Bulk HGF IHC can't separate "pro-HGF (cancer cell) vs. active HGF (TAM-HGFAC generated)" — HGFAC ELISA + HAI-1 ratio does. For patient-derived xenografts (PDX) of PDAC with variable c-Meti response, pre-treatment tumor HGFAC/HAI-1 ratio predicts which PDX will respond (high ratio = capmatinib-sensitive, low ratio = innate-resistant because c-Met not actually activated despite high HGF IHC).
- Acute Kidney Injury (AKI) & Hepatorenal ACLF (The Kidney–Liver Axis)
HGFAC is constitutively expressed in proximal tubule cells (kidney) and shed into urine/plasma upon injury; in bilateral renal IRI (30 min pedicle clamp) → plasma HGFAC rises 2–3× by 24 h, kidney homogenate HGFAC rises 4–6× by 48 h (tubular dedifferentiation + repair signal). If you're testing MCP-1 neutralization, SGLT2i (empagliflozin renal protection), or AKI-to-CKD transition (unilateral ureteral obstruction, UUO), kidney HGFAC + urinary HGFAC (if you concentrate 10×) + NGAL/KIM-1 + p-Met (kidney tubular c-Met activation, which drives tubular regeneration) close the "HGF axis repair" PD. For hepatorenal ACLF (CCl4 12 wk + LPS 5 mg/kg challenge): plasma HGFAC rises 3–5× (both liver PHx-like regeneration + kidney AKI spill), and the HGFAC:HAI-1 ratio in plasma correlates with 7-d survival (high ratio = better regeneration reserve). KTE71484 on plasma (EDTA, 50 μL, dilute 1:2 in kit buffer) catches the 0.1–1.5 ng/mL range with <8% CV — LC-MS for HGFAC would need tryptic digest + PRM, ~$50/sample, unnecessary for cohort screening.
- Coagulation–Regeneration Crosstalk (The Factor Xa–HGFAC Link)
This is the niche but cool lane: PHx + enoxaparin (low-molecular-weight heparin, 1 mg/kg sc bid) → factor Xa inhibition → HGFAC activation blunted (because factor Xa is a physiological HGFAC activator on the endothelial surface) → p-Met peak drops 30%, Ki67+ hepatocytes at 48 h drop 20%, liver mass recovery at 168 h drops 15%. If you're studying anticoagulant–liver regeneration interactions (relevant for post-major-resection patients on VTE prophylaxis), HGFAC ELISA is the mechanistic readout that connects "Xa inhibition → less HGFAC activation → less active HGF → slower regeneration." You can also flip it: PHx + factor Xa-activating peptide (FXa-AP, experimental) → HGFAC activation ↑, p-Met ↑, regeneration accelerated — the "pro-coagulant enhances liver repair" paradigm. KTE71484 on liver homogenate + plasma captures both directions; pair with thrombin–antithrombin (TAT) complex ELISA (if available) to close the coagulation readout.
Quick Optimization Notes (HGFAC-Specific — TTSP/Protease Hygiene)
• Protease inhibitor cocktail is non-negotiable at harvest: HGFAC is a serine protease — if you homogenize liver/kidney/TME in plain RIPA without inhibitors, ~30% of HGFAC auto-activates or trims neighbor proteins during the 30-min rotate, and the zymogen:active ratio shifts artifactually. Use RIPA + cOmplete PI tablet (Roche) + 1 mM AEBSF + 10 μg/mL leupeptin + 1 μg/mL aprotinin — AEBSF is the TTSP-preferred inhibitor (PMSF is slower for TTSPs, half-life ~30 min at pH 7.4, AEBSF is more stable). Keep on ice, 4°C rotate 20 min, 12k ×g 10 min — sup stable -80°C ≤1 freeze–thaw. Don't use just PMSF for TTSPs.
• Epitope check for zymogen vs. active: If your CoA says "detects both zymogen and two-chain," great — most TTSP sandwich pairs target the LDLR or SEA domains (present in both) or the SP heavy chain (present in both). If the detection is on the SP light chain C-terminal (only in two-chain), then you only see active — confirm on CoA which you're getting. For PHx/PDAC, "both" is preferable because the zymogen pool is the reserve.
• Plasma vs. serum: Prefer EDTA plasma for HGFAC — heparin can weakly interact with the LDLR domains of HGFAC (heparin-binding is a feature of many TTSPs via their LDLR/LG domains), potentially shifting the sandwich OD 5–10%. If you must use serum, note the minor offset. Collect cardiac/submandibular into EDTA, centrifuge 2000 ×g 10 min 4°C within 30 min, aliquot 20 μL -80°C, ≤1 freeze–thaw.
• TTSP cross-reactivity self-check: Run a liver homogenate from Tmprss2-KO (if available) or TMPRSS4-KO as a control — KTE71484 signal should be unchanged (cross <1%), confirming your PHx liver read isn't TMPRSS2 bleed (TMPRSS2 is also PHx-upregulated in bile ducts, ~2–3×, but shouldn't contribute to HGFAC signal). If your signal drops 20% in Tmprss2-KO liver, the kit's cross is higher than claimed — contact Abbkine CoA for batch-specific validation.
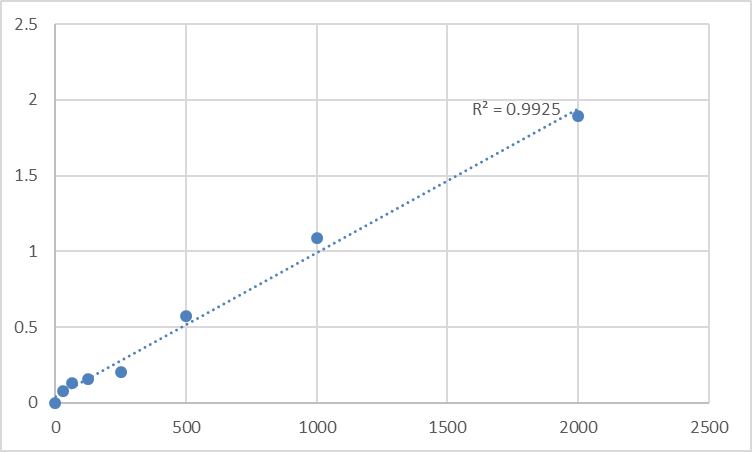
• Standard stability: Recombinant mouse HGFAC standard (if supplied as zymogen, ~65 kDa) is more stable than active two-chain (auto-activation risk in dilute aqueous), but TTSPs are generally robust if kept at 4°C in buffer + 0.1% BSA + AEBSF trace. Reconstitute gently by pipetting (no vortex — TTSP SEA domain can shear), aliquot -20°C single-use, avoid >1 freeze–thaw. If standard curve R² <0.99 on first run, check if stock was left at 4°C >1 week — TTSP autodegrades slowly.
The Bottom Line
HGFAC (HGFA) is the 65–70 kDa type II transmembrane serine protease that activates pro-HGF into the c-Met-driving α/β heterodimer — and it's the upstream gatekeeper that HGF-only panels completely miss in liver regeneration, PDAC TME, AKI, and ACLF. But HGFAC's TTSP family cross-reactivity (TMPRSS2/TMPRSS4 etc. in liver/kidney/TME), the zymogen/active duality, and plasma's low abundance (0.05–0.5 ng/mL) make "universal TTSP" or HGF-only approaches noisy for mouse cohorts. The Mouse Hepatocyte Growth Factor Activator (HGFAC) ELISA Kit (KTE71484) from Abbkine gives you the mouse-dedicated sandwich (capture+detection away from activation cleave + active-site triad, so zymogen+active both caught), ~0.05 ng/mL LOD, liver/kidney/TME/plasma validation, and <8% intra-CV — so your PHx "HGFAC ↑4×, HAI-1 ↓30%, p-Met ↑5×" triad actually closes mechanistically, and your KPC + capmatinib PDX "TAM-HGFAC/HAI-1 ratio predicts response" claim has quantitative backbone. Whether you're phenotyping 2/3 PHx + empagliflozin renal-crosstalk, screening pexidartinib + capmatinib in KPC, or parsing factor Xa–HGFAC crosstalk in anticoagulated liver recovery, it's the HGFAC reagent that doesn't make you blame your HGF antibody.
Product Reference: KTE71484 – Mouse Hepatocyte Growth Factor Activator (HGFAC) ELISA Kit
Learn more and order: https://www.abbkine.com/product/mouse-hepatocyte-growth-factor-activator-hgfac-elisa-kit-kte71484/
(For Research Use Only; not for diagnostic procedures in humans.)





