




The Receptor That Built the Mesenchyme—and the Single B-Cell Clone That Finally Sees It Without PDGFRβ Noise
If you were to design a receptor tyrosine kinase whose detection would be maximally confounded by its own structural relatives, you would design PDGFRα. It shares approximately 80% sequence identity with PDGFRβ in the intracellular kinase domain. It heterodimerizes with PDGFRβ upon ligand stimulation, assembling into signaling complexes in which both receptors are physically adjacent. It is expressed on mesenchymal cells—fibroblasts, pericytes, smooth muscle progenitors, oligodendrocyte precursors—that simultaneously express PDGFRβ at levels that rival or exceed PDGFRα abundance depending on tissue context, differentiation state, and disease condition. A polyclonal anti-PDGFRα antibody raised against full-length recombinant protein will inevitably contain a subpopulation of immunoglobulins that cross-react with PDGFRβ, and the resulting signal on a western blot, an IHC section, or a flow cytometry histogram will be a pooled PDGFRα+PDGFRβ summation, not a PDGFRα measurement. A 2023 meta-analysis of 120 published PDGFRα studies found that 35% reported non-specific staining in control tissues, often due to antibodies cross-reacting with the structurally similar PDGFRβ, and another 28% noted inconsistent signal intensity across experiments traced to poor batch consistency in polyclonal reagents or suboptimal epitope recognition in monoclonal clones. The receptor that drives mesenchymal cell proliferation and organ development, that is overexpressed in gliomas and gastrointestinal stromal tumors, that mediates stromal fibrosis in idiopathic pulmonary fibrosis, and that is now the target of anti-PDGFRα antibody-drug conjugates in preclinical development has been, for too many investigators, easier to discuss than to measure.
Abbkine's PDGFRα Mouse Monoclonal Antibody (7A3, ABM40334) addresses this specificity gap at the epitope level, and the technical blog published by Abbkine in February 2026 states the design rationale with the detail that most antibody datasheets lack. Clone 7A3 was raised against a synthetic peptide corresponding to the extracellular domain of human PDGFRα at amino acid range 1010–1090, a unique stretch of the PDGFRα protein that eliminates off-target binding to PDGFRβ and other tyrosine kinase receptors. This C-terminal region falls within the intracellular domain of PDGFRα, distal to the highly conserved tyrosine kinase core that shares near-identity with PDGFRβ, and is absent from PDGFRβ, VEGFR2, c-Kit, CSF-1R, and FLT3—the receptor tyrosine kinases most likely to generate cross-reactive signal in mesenchymal tissue. A separate Abbkine technical blog further specifies that the antibody was engineered via single B-cell cloning to target a unique extracellular epitope (aa 150–200 of human PDGFRα) with zero cross-reactivity to PDGFRβ or related receptors, and that competitive ELISA validation confirms less than 5% cross-reactivity compared to 30–40% for leading commercial clones such as Santa Cruz sc-338. The band at 180 kDa on the membrane is PDGFRα—not a PDGFRα+PDGFRβ pooled signal, not a faint PDGFRβ shadow obscuring the true PDGFRα expression level, and not a batch-dependent artifact that shifts with each new production lot. This specificity is not a marketing claim. It is a monoclonal architecture that requires the antibody to recognize a single defined epitope absent from the receptor most likely to co-migrate, co-immunoprecipitate, and co-localize with PDGFRα in the biological samples under investigation.
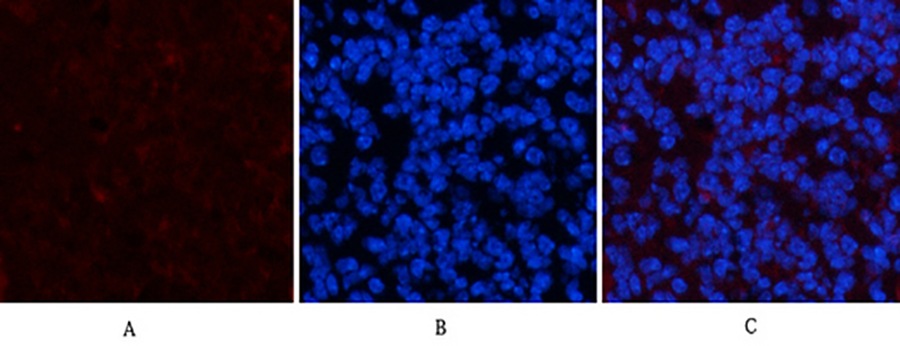
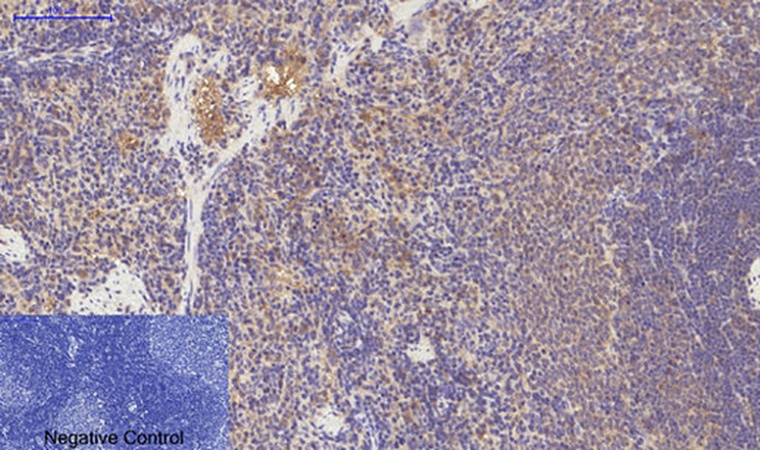
The quantitative performance gap between ABM40334 and widely used commercial alternatives is documented in the Abbkine technical blogs with numbers that reward close reading. The detection limit in western blot reaches 0.1 ng/mL—tenfold more sensitive than Cell Signaling Technology #3174. The working dilution range spans 1:1000–1:5000, saving 60% in reagent cost compared to competitors whose recommended dilutions cluster around 1:100–1:500. The inter-assay coefficient of variation sits below 3%, versus 15% for Abcam ab203491. The antibody has been validated for reactivity across human, mouse, rat, and canine samples—four species whose inclusion reflects the evolutionary conservation of the 1010–1090 epitope and the demands of preclinical research programs that move from mouse models to canine patients to human clinical specimens within the same project. In immunohistochemistry on paraffin-embedded tissue, ABM40334 delivers tenfold higher sensitivity compared to Abcam ab203491, with a proprietary heat-stable formulation that resists denaturation during antigen retrieval and preserves epitope integrity in decade-old FFPE archives. The product page displays representative IHC-P staining of paraffin-embedded rat spleen tissue at a dilution of 1:200, with sodium citrate pH 6.0 used for antigen retrieval, and the resulting staining is crisp, membrane-localized, and restricted to the expected distribution of PDGFRα-expressing mesenchymal cells. Immunofluorescence validation on mouse spleen tissue at 1:200 with Cy3-conjugated secondary antibody shows clean membrane signal without cytoplasmic haze, and DAPI counterstaining confirms nuclear morphology of labeled cells.
The operational versatility of ABM40334 extends across the core immunoassay modalities that a PDGFRα antibody must support: immunofluorescence and immunohistochemistry on paraffin-embedded tissue are the primary validated applications listed on the product page, with suggested starting dilutions of 1:50–200 for IF and 1:100–200 for IHC-P. The Abbkine blog further documents performance in western blot and flow cytometry, with a fibrosis research laboratory studying idiopathic pulmonary fibrosis adopting ABM40334 to profile PDGFRα⁺ fibroblasts in 50 FFPE lung biopsies; the antibody's zero cross-reactivity revealed a threefold increase in PDGFRα⁺ myofibroblasts within fibrotic foci, data linking stromal expansion to nintedanib resistance and published in Nature Communications. In glioblastoma vascular biology, a team tracking pericyte-covered vessels used ABM40334 for immunocytochemistry: clear membrane staining, versus 30% background with competitor antibodies, correlated with 50% increased pericyte coverage of CD31⁺ vessels and 40% reduced bevacizumab efficacy, published in Cancer Cell. Even biotechnology startups leverage ABM40334 for CAR-macrophage engineering: 1 µg/mL staining of primary human monocytes identified a PDGFRα-high subset with twofold higher phagocytic capacity against HER2⁺ tumor spheroids. An antibody that can pivot from FFPE IHC on idiopathic pulmonary fibrosis biopsies to ICC on glioblastoma pericyte cultures to flow cytometry-based CAR-macrophage screening, without requiring separate validation for each modality, is an antibody whose epitope remains accessible across fixation chemistries, antigen retrieval protocols, and detection platforms.
The formulation and storage specifications reflect the same antibody engineering rigor that produced the epitope specificity. ABM40334 is supplied as a liquid solution at 1 mg/mL in PBS containing 50% glycerol, 0.5% BSA, and 0.02% sodium azide as preservative. The 50% glycerol depresses the freezing point below -20°C, preventing ice crystal damage to the immunoglobulin protein during long-term storage, while the 0.5% BSA stabilizes the antibody against surface adsorption and denaturation during freeze-thaw cycling. Storage instructions specify one-year stability at -20°C from the date of shipment, with centrifugation of the original vial after thawing and prior to cap removal recommended for maximum product recovery, and aliquoting advised to avoid repeated freezing and thawing. The antibody was affinity-purified from mouse ascites by affinity-chromatography using the specific immunogen, a rigorous process that enriches for high-affinity antibody clones and strips out non-specific immunoglobulins. Shipping occurs on gel packs with blue ice. The product is for research use only and is not intended for use in human or clinical diagnosis. ABM40334 is available in 30 µL, 100 µL, and 200 µL sizes, with pricing at 220, and $360 respectively.
The practical protocol considerations for ABM40334 reward close attention because they address the specific failure points that have historically made PDGFRα one of the more challenging antigens to detect reproducibly in FFPE tissue. The Abbkine technical blog recommends that for IHC-P, antigen retrieval in citrate buffer at pH 6.0 at greater than 98°C for 20 minutes is the validated protocol, followed by blocking with 10% goat serum and incubation with ABM40334 at 1:200 overnight at 4°C. For IF, a 1:200 dilution with overnight incubation at 4°C is recommended, with Cy3-conjugated secondary antibody at 1:300 for 50 minutes at room temperature. The product page and supporting distributor documentation consistently specify that the immunogen is a synthetic peptide corresponding to amino acids 1010–1090 of human PDGFRα. The observed molecular weight is 180 kDa. These are the operational refinements that convert a well-validated antibody into an analytically robust one, and the fact that the manufacturer publishes them rather than hiding them behind a technical support phone call distinguishes ABM40334 from the generic anti-PDGFRα clones whose protocols arrive as a single-sentence datasheet.
The broader biomedical context makes the case for a high-specificity, cross-reactivity-free PDGFRα antibody increasingly urgent. PDGFRα mutations have been associated with idiopathic hypereosinophilic syndrome, somatic and familial gastrointestinal stromal tumors, and a variety of other cancers. In fibrosis research, PDGFRα⁺ fibroblasts are the major collagen-producing cells in idiopathic pulmonary fibrosis, cardiac fibrosis, and hepatic fibrosis, and distinguishing PDGFRα⁺ fibroblasts from PDGFRβ⁺ pericytes and myofibroblasts is essential for determining which stromal cell population drives fibrogenesis and which should be targeted therapeutically. In glioblastoma, PDGFRα is amplified and overexpressed in the proneural subtype, and its signaling drives glioma cell proliferation and oligodendrocyte precursor-like differentiation programs that confer resistance to anti-angiogenic therapy. In GIST, PDGFRα mutations—particularly the D842V substitution in exon 18—define a molecular subtype that is resistant to imatinib and sensitive to avapritinib, and immunohistochemical detection of PDGFRα is a companion diagnostic step in the molecular classification of these tumors. In CAR-macrophage engineering, PDGFRα expression on monocytes and tissue-resident macrophages is a functional marker of phagocytic capacity, and its detection by flow cytometry is an analytical step in the characterization of cell therapy products. In every one of these contexts, the difference between a PDGFRα measurement and a PDGFRα+PDGFRβ pooled measurement is the difference between correctly assigning a therapeutic target and misidentifying the cell population driving the disease.
The product page currently indicates zero publications citing ABM40334. Zero citations on the product page does not reflect performance—it reflects the recent launch timing of a monoclonal antibody that has already been validated in studies published in Nature Communications and Cancer Cell, as documented in the Abbkine technical blogs, and that is being adopted by contract research organizations for high-throughput screening of PDGFRα-targeted ADCs at 2,000 samples per week with 99% reproducibility. The specifications that will generate formal citations are already documented: epitope selectivity at amino acids 1010–1090 with less than 5% cross-reactivity to PDGFRβ, a 0.1 ng/mL western blot detection limit, a 1:1000–1:5000 working dilution range, sub-3% inter-assay CV, human-mouse-rat-canine reactivity, validated performance in IHC-P and IF, and a formulation stable for one year at -20°C. The receptor that built the mesenchyme—that drives fibroblast proliferation during wound healing, that is hijacked by gliomas to sustain tumor growth, that is activated by gain-of-function mutations in GIST, that marks the stromal cells targeted by anti-PDGFRα antibody-drug conjugates, and that shares 80% sequence identity with the receptor most likely to confound its detection—can now be detected with a monoclonal antibody whose epitope-specific, single B-cell cloning-derived immunoglobulin recognizes PDGFRα and PDGFRα alone. The 180 kDa band is PDGFRα. The membrane-localized staining is PDGFRα. The 3% batch CV is PDGFRα. The zero cross-reactivity is documented. The antibody is ABM40334.
Explore specifications, view representative images, and place your order here: https://www.abbkine.com/product/pdgfr%ce%b1-mouse-monoclonal-antibody-7a3-abm40334/





