




The Decoy Receptor That Outsmarts Bone—and the ELISA That Reads It Without Cross‑Reactive Noise
Every endocrinologist who has ever stared at a DXA scan and wondered whether the patient’s bone mineral density actually reflects the molecular tug‑of‑war inside the marrow already knows the answer. It does not. Bone is not a static scaffold of calcium phosphate. It is a demolition‑and‑reconstruction site that never closes, and the foreman deciding whether the osteoclast wrecking crew reports for duty is a three‑protein signaling axis: RANKL, the activator that binds its receptor RANK on osteoclast precursors and screams “resorb”; RANK, the receptor that transduces that command; and osteoprotegerin, the soluble decoy receptor that floats into the gap, wraps itself around RANKL, and silences the order before a single osteoclast matures. OPG is not merely a biomarker of bone turnover. It is the molecular brake pedal on osteoclastogenesis, and the force with which that pedal is pressed determines whether a postmenopausal woman loses 3% of her trabecular bone per year or maintains microarchitecture into her eighth decade. A 2024 narrative review reaffirmed that the RANK/RANKL/OPG signaling pathway plays a crucial role in the onset and advancement of osteoarthritis, and recent developments have emphasized the importance of this triad in disease progression beyond the bone compartment, extending into skeletal muscle, the central nervous system, and the vasculature. When OPG concentrations shift, the consequences cascade through osteoporosis, rheumatoid arthritis, cancer metastasis, vascular calcification, and even insulin sensitivity—and quantifying that shift has, for too long, depended on kits whose cross‑reactivity with the very ligands OPG binds has systematically inflated or obscured the measurement.
Abbkine’s Human Osteoprotegerin (OPG) ELISA Kit (KTE60224) enters this analytical landscape with a detection architecture that is biochemically direct and immunologically specific. The kit employs a two‑site sandwich ELISA to quantitate TNFRSF11B—the gene product that encodes OPG—in samples. An antibody specific for TNFRSF11B has been pre‑coated onto a microplate; standards and samples are pipetted into the wells and any TNFRSF11B present is bound by the immobilized antibody. After removing any unbound substances, a biotin‑conjugated antibody specific for TNFRSF11B is added to the wells. Following washing, Streptavidin conjugated Horseradish Peroxidase (HRP) is added, and after a further wash to remove any unbound avidin‑enzyme reagent, a substrate solution develops color in proportion to the amount of TNFRSF11B bound in the initial step. The color development is stopped, and the intensity of the color is measured on any standard visible‑wavelength microplate reader. The assay runs for 3–5 hours depending on the experience of the operator—a same‑day experiment that fits comfortably within a standard laboratory workday.
What distinguishes KTE60224 from the generic OPG ELISA kits that populate the market is not the sandwich format per se—which is well‑established and biochemically validated—but the specificity specification that the dual‑site recognition architecture earns. The product documentation states that the kit has high sensitivity and excellent specificity for detection of Human TNFRSF11B, with no significant cross‑reactivity or interference between Human TNFRSF11B and analogues observed. This matters because OPG is a member of the tumor necrosis factor receptor superfamily, a group that includes at least 29 members, many of which share structural domains—cysteine‑rich repeats, death domains, TRAF‑binding motifs—that can generate cross‑reactive signal in single‑antibody detection formats. More critically, OPG’s biological function is to bind RANKL, and RANKL is present in the very serum, plasma, and cell‑culture supernatants that researchers load into ELISA wells. An antibody pair that cannot distinguish OPG from an OPG‑RANKL complex, or that cross‑reacts with free RANKL at nanomolar concentrations, is not measuring OPG. It is measuring a pooled signal that shifts with RANKL abundance independently of OPG. The dual‑site sandwich architecture of KTE60224 requires both the capture and detection antibodies to engage OPG for signal to develop, providing a specificity barrier that single‑antibody detection formats cannot replicate.
The calibration range and limit of detection are specified as “please inquire,” a designation that is standard for recently launched kits whose dynamic range specifications are documented in the package insert and validated against biological matrices that vary in endogenous OPG content. What is documented on the product page is the kit’s features and benefits statement: high sensitivity and excellent specificity. The component list is comprehensive: Human Osteoprotegerin microplate, Human Osteoprotegerin standard, Human Osteoprotegerin detect antibody, Streptavidin‑HRP, standard diluent, assay buffer, HRP substrate, stop solution, wash buffer, and plate covers. The unopened kit stores at 2–8°C, requiring no −20°C freezer space and subjecting the pre‑coated capture antibody to none of the freeze‑thaw cycling that progressively degrades binding affinity in kits stored under suboptimal conditions. Shipping occurs on gel packs with blue ice.
Sample compatibility spans the biological matrices in which OPG is biologically and clinically relevant: serum, plasma, cell culture supernatants, and other biological fluids. Serum and plasma are the canonical sample types for systemic OPG quantification, and the kit accommodates both without requiring separate validation protocols. Cell culture supernatant compatibility extends the kit’s utility to the bench researcher studying OPG secretion from osteoblasts, bone marrow stromal cells, vascular smooth muscle cells, or tumor cells—the experimental systems in which the molecular regulation of OPG expression, the signaling pathways that control its release, and the functional consequences of its production are most directly interrogated. The inclusion of “other biological fluids” accommodates specialized sample types such as synovial fluid, cerebrospinal fluid, gingival crevicular fluid, and tissue interstitial fluid, enabling multi‑compartment OPG profiling within a single standardized ELISA workflow.
The publication record for KTE60224 provides an independent validation that no manufacturer’s internal QC dataset can replicate. At the time of writing, the product page documents one citation in peer‑reviewed literature. One citation is not a large number, but it is an independent laboratory that prepared its own samples, ran the assay under the pressures of peer review, and found the resulting values credible enough to publish. Every widely adopted ELISA kit in the Abbkine catalog began with one citation, and the specifications that will generate more are already documented: two‑site sandwich ELISA with dual‑antibody recognition, no significant cross‑reactivity or interference with TNFRSF11B analogues, compatibility with serum, plasma, and cell culture supernatants, a 3–5 hour assay duration, and storage at 2–8°C.
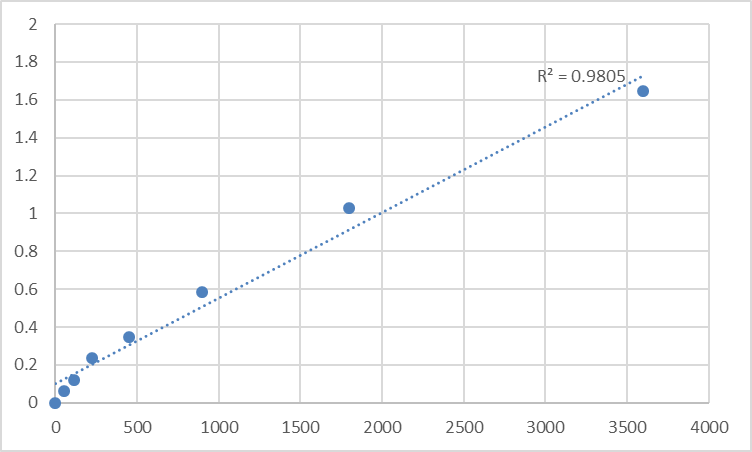
The protocol notes reflect genuine sandwich ELISA discipline rather than generic disclaimers. Allow all reagents to warm to room temperature for at least 30 minutes before opening to prevent condensation on cold reagent vials from altering concentration. Pre‑rinse the pipette tip with reagent, and use fresh pipette tips for each sample, standard, and reagent to prevent carryover contamination. Mix thoroughly—it is very important for the result—using a low‑frequency oscillator or slight hand shaking every 10 minutes. It is recommended that all samples and standards be assayed in duplicate or triplicate. Unused wells must be kept desiccated at 4°C in the sealed bag provided. Do not mix components from different kit lots or use reagents beyond the kit expiration date. These are the operating procedures that separate a standard curve with an R² above 0.99 from a dataset a reviewer will question.
The molecular identity of the analyte that KTE60224 detects deserves explicit articulation because it explains why OPG quantification sits at the intersection of bone biology, vascular medicine, oncology, and metabolic research. Osteoprotegerin is a basic glycoprotein comprising 401 amino acid residues arranged into 7 structural domains. It is found as either a 60‑kDa monomer or a 120‑kDa dimer linked by disulfide bonds, and it functions as a RANK homolog, binding to RANKL on osteoblast/stromal cells and blocking the RANKL‑RANK interaction between osteoblast/stromal cells and osteoclast precursors. This has the effect of inhibiting the differentiation of the osteoclast precursor into a mature osteoclast. The gene maps to chromosomal location 8q24.12, and alternative designations include TNFRSF11B, OCIF (osteoclastogenesis inhibitory factor), and TR1.
The biomedical context that KTE60224 enters is expanding on multiple fronts simultaneously, and each front demands OPG quantification of a precision that legacy ELISA kits cannot provide. In osteoporosis and bone biology, OPG is not merely a passive biomarker of bone resorption; it is the endogenous inhibitor that recombinant OPG‑Fc therapeutics were designed to mimic, and the rationale for denosumab—a fully human monoclonal antibody that binds RANKL and mimics the effect of endogenous OPG—rests on the same RANKL‑sequestration mechanism that OPG itself employs. Multiple clinical trials have demonstrated that denosumab suppresses bone resorption, increases bone mineral density, and reduces fracture risk in postmenopausal women, and the pharmacodynamic relationship between denosumab treatment and endogenous OPG levels is a variable of direct clinical interest. A 2024 review chronicling the bench‑to‑bedside elucidation of the OPG‑RANK‑RANKL pathway noted that OPG diminishes advanced bone cancer pain.
In oncology, OPG occupies a dual role that makes its quantification simultaneously essential and analytically treacherous. OPG binds RANKL and prevents osteoclastic bone resorption, but it also protects prostate cancer cells from the apoptotic effects of TRAIL, providing tumor cells that produce OPG with survival advantages. In the bone metastatic microenvironment, cancer cells secrete soluble factors that act on osteoblasts and osteoclasts: RANKL production is increased and OPG secretion is decreased from osteoblasts, tipping the balance toward osteoclastic activation and the release of bone‑matrix‑embedded growth factors that fuel tumor proliferation. The RANKL/RANK/OPG pathway is a key regulator of pathological bone metabolism in metastatic sites, and quantifying OPG in tumor‑conditioned medium, in the serum of patients with bone metastases, and in the bone marrow plasma of preclinical models is essential for understanding whether a therapeutic intervention restores the OPG‑to‑RANKL balance or merely shifts the equilibrium in a different direction.
In cardiovascular medicine, OPG has emerged as a modulator of vascular calcification linked to vascular smooth muscle cell proliferation and collagen production in atherosclerotic plaques. A 2025 scoping review with meta‑analysis identified OPG as an emerging biomarker of carotid artery stenosis. A separate 2025 study demonstrated that elevated serum OPG concentrations have been accompanied with aortic calcification and elevated mortality risk in end‑stage renal disease individuals. In diabetes and metabolic disease, increased serum OPG levels may be a risk factor for insulin resistance, and OPG might be implicated in the pathogenesis of diabetes as a potential biomarker of insulin resistance in subjects with prediabetes and type 2 diabetes. A 2024 study demonstrated that deletion of the epigenetic regulator Hdac3 in osteoprogenitors prevents insulin resistance induced by high‑fat diet by increasing serum and skeletal gene expression levels of OPG, establishing a direct mechanistic link between bone‑derived OPG and systemic glucose homeostasis.
In neurology, the OPG/RANKL/RANK framework plays a crucial role in bone remodeling and the functioning of the central nervous system, with recent research providing evidence that the components of OPG, RANKL, and RANK are expressed in the CNS and associated with neurological disorders. In immunology, RANKL and OPG are expressed by activated T cells and dendritic cells, and the RANKL‑RANK‑OPG axis participates in lymph node organogenesis, thymic medullary epithelial cell development, and the regulation of immune tolerance. In oral medicine, the OPG/RANKL/RANK axis is the central regulator of alveolar bone remodeling in periodontitis, orthodontic tooth movement, and osseointegration of dental implants, and OPG quantification in gingival crevicular fluid is a direct measurement of local bone‑resorptive activity.
For the endocrinologist quantifying OPG in postmenopausal serum to track the pharmacodynamic response to denosumab, the oncologist measuring OPG in tumor‑conditioned medium to determine whether a breast cancer cell line secretes a decoy receptor that shields it from TRAIL‑mediated apoptosis, the cardiologist evaluating OPG as a biomarker of vascular calcification in a chronic kidney disease cohort, the diabetes researcher investigating the bone‑pancreas axis and the role of OPG in insulin sensitivity, the neuroscientist profiling OPG in cerebrospinal fluid, or the basic scientist performing any experiment in which the RANKL‑to‑OPG ratio determines the biological outcome, direct OPG quantification is not a supplementary measurement. It is the data point that connects a signaling pathway to a physiological outcome, and the quality of that measurement determines the quality of the conclusion.
The decoy receptor that outsmarts bone—that floats into the extracellular space, binds RANKL before it can engage RANK, inhibits osteoclast differentiation, protects cancer cells from TRAIL, modulates vascular calcification, correlates with insulin resistance, and functions in the central nervous system—is now quantifiable with a sandwich ELISA whose dual‑site recognition architecture provides the specificity that single‑antibody detection formats cannot achieve, whose sample compatibility spans serum, plasma, and cell culture supernatants, whose workflow completes in 3–5 hours, whose unopened kit stores at 2–8°C, and whose one peer‑reviewed citation represents an independent laboratory that trusted its data under the scrutiny of peer review. The protein that Amgen spent a billion dollars mimicking is now measurable with a kit that costs a fraction of a single dose of the drug it inspired.
Explore specifications, access the protocol, and place your order here: https://www.abbkine.com/product/human-osteoprotegerin-opg-elisa-kit-kte60224/





