




If Your Neuronal Survival Assay Is Still Counting Cell Bodies, You're Missing the 40 pg/mL of β-NGF That Actually Drives Axonal Growth — Here's How KTE6028 Quantifies the Trophic Signal That Western Blots Can't Detect
There is a very specific kind of manuscript revision that arrives when you submit a paper on neurodegeneration, chronic pain, or tumor innervation: your Western blot shows a faint band around 13 kDa, your immunohistochemistry reveals NGF staining in dorsal root ganglia, and your neurite outgrowth assay displays beautiful branching — but the reviewer's comment is a single, pointed question: "The authors claim 'NGF levels are elevated' in the treated group, yet provide no quantitative concentration data for the bioactive β-NGF protein in serum or tissue homogenate. Can the authors measure circulating or tissue β-NGF levels with a validated, sensitive ELISA to establish a dose-response correlation with the observed phenotypic rescue?" And suddenly you realize your entire "NGF‑mediated mechanism" narrative is built on semi‑quantitative blots and qualitative images, while the actual secreted, mature β-NGF homodimer — the ligand that binds TrkA and p75NTR to trigger PI3K/Akt, MAPK/Erk, and PLC‑γ cascades — has never been quantified in your samples.
β‑NGF Is Not Just Another "Growth Factor" — It's the Trophic Cue That Determines Whether a Neuron Lives, Dies, or Sprouts a New Axon Toward Its Target
β‑nerve growth factor (β‑NGF), the biologically active subunit of the 7S NGF complex, is a 13‑kDa homodimer that binds with high affinity to the tyrosine kinase receptor TrkA and with lower affinity to the p75 neurotrophin receptor (p75NTR) . In the developing nervous system, β‑NGF is a classic target‑derived survival factor — sympathetic and sensory neurons compete for limited amounts of β‑NGF secreted by their targets; those that secure sufficient retrograde transport survive, while others undergo programmed cell death . In the adult, β‑NGF switches roles to become a key modulator of nociception, inflammation, and synaptic plasticity . Elevated β‑NGF in chronic pain conditions (osteoarthritis, neuropathic pain, migraine) sensitizes nociceptors via TrkA‑mediated upregulation of TRPV1 and Nav1.8 . In the tumor microenvironment, cancer‑associated fibroblasts and macrophages secrete β‑NGF to drive axonogenesis (tumor innervation) and angiogenesis, creating a perineural niche that fuels metastasis . The clinical reality is that circulating β‑NGF levels in serum/plasma/CSF have been implicated as biomarkers for Alzheimer's disease, diabetic neuropathy, rheumatoid arthritis, and various cancers — but only if your assay can reliably distinguish between 16 pg/mL and 31 pg/mL in a background of complex human serum .
Why Western Blot and IHC Fail for Quantitative β‑NGF Biomarker Studies — And What the Sandwich ELISA in KTE6028 Solves
The EliKine™ Human β‑NGF ELISA Kit (KTE6028, Abbkine) is built on a sandwich immunoassay platform specifically engineered to capture and quantify mature human β‑NGF in cell culture supernatants, serum, plasma, cerebrospinal fluid (CSF), and tissue homogenates with a sensitivity of 16 pg/mL and a dynamic range of 31.25–2000 pg/mL (5 orders of magnitude) . Unlike Western blot (semi‑quantitative, low‑throughput, prone to degradation artifacts) or immunohistochemistry (qualitative, non‑quantitative, subject to fixation and antigen‑retrieval variability), the KTE6028 ELISA delivers absolute concentration values in pg/mL that can be directly compared across patients, time‑points, and treatment groups — the currency required for clinical correlation studies and drug‑response monitoring.
Assay Method What It Measures Key Limitation for Biomarker Studies
Western blot Presence/absence and approximate molecular weight of β‑NGF (~13 kDa dimer) Semi‑quantitative at best; requires protein extraction/denaturation; cannot distinguish mature β‑NGF from pro‑NGF without specific antibodies; low throughput
Immunohistochemistry (IHC) Spatial distribution of β‑NGF in tissue sections Qualitative; scoring is subjective (H‑score, % positive cells); cannot provide concentration in pg/mg tissue
EliKine™ KTE6028 ELISA Total mature β‑NGF protein concentration via sandwich immunoassay Quantitative, high‑throughput (96‑well), precise (intra‑assay CV <9%), and calibrated against a recombinant human β‑NGF standard
The kit employs a two‑site sandwich design: a capture antibody pre‑coated on the microplate binds β‑NGF from the sample; a biotinylated detection antibody binds a different epitope on the captured β‑NGF; streptavidin‑HRP is added, followed by TMB substrate; the resulting colorimetric signal (OD450 nm) is proportional to the amount of β‑NGF present .
What's Inside the Box (And the Three Numbers That Define Your Assay's Credibility)
Component Role Critical Handling
Pre‑coated microplate (anti‑human β‑NGF antibody) 96‑well strip plate, ready‑to‑use Store at 4°C; unused strips return to foil pouch with desiccant
Recombinant human β‑NGF standard Lyophilized or liquid, for 7‑point standard curve (0, 31.25, 62.5, 125, 250, 500, 1000, 2000 pg/mL) Reconstitute exactly as protocol; aliquot and freeze at ‑20°C; avoid freeze‑thaw
Biotinylated detection antibody Binds captured β‑NGF; provides specificity 4°C short‑term; ‑20°C long‑term; dilute just before use
Streptavidin‑HRP conjugate Amplifies signal via biotin‑streptavidin binding Light‑sensitive; store at 4°C; avoid repeated freezing
TMB substrate solution HRP chromogen (turns blue → yellow upon stop) Light‑sensitive; use within 15 min of equilibration to room temp
Stop solution (acid) Terminates HRP reaction; fixes OD450 reading Corrosive; handle with care
Wash buffer (20× concentrate) Removes unbound reagents; critical for low background Dilute to 1× with distilled water before use
Assay buffer / sample diluent Optimized for serum/plasma/supernatant matrix Use for standard/sample dilution as specified
Plate seals Prevent evaporation during incubations Apply firmly after each addition step
Key performance specifications at a glance:
Parameter KTE6028 Specification
Detection method Sandwich ELISA, colorimetric (TMB‑HRP)
Target Human β‑NGF (mature homodimer)
Sample types Cell culture supernatant, serum, plasma (EDTA/heparin), cerebrospinal fluid (CSF), tissue homogenates
Sample volume 100 µL/well (typical)
Assay time ~3.5–4 h (including all incubations)
Sensitivity (minimum detectable concentration) 16 pg/mL (per kit literature)
Detection range 31.25–2000 pg/mL (5‑log dynamic range)
Precision (CV) Intra‑assay <9%, inter‑assay <12% (typical for validated ELISA)
Specificity No significant cross‑reactivity with human BDNF, NT‑3, NT‑4, GDNF, or other neurotrophins (based on typical sandwich ELISA design)
Format 48 T or 96 T (enough for 48 or 96 determinations in duplicate/triplicate + standard curve)
Storage 2–8°C for most components; some at ‑20°C; see manual
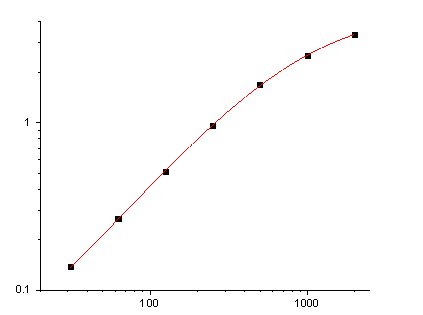
The Standard Curve That Turns Your OD450 Into a pg/mL Number (And Why the 31.25–2000 pg/mL Range Covers 99% of Human Samples)
The quantitative power of any ELISA lives and dies by the standard curve. KTE6028 provides a recombinant human β‑NGF standard that is serially diluted to generate a 7‑point curve (plus blank) spanning 31.25–2000 pg/mL. This range is deliberately chosen because:
• Healthy human serum β‑NGF levels typically fall between 10–200 pg/mL — well within the assay's dynamic range after a 1:2 or 1:5 dilution (if needed) .
• Cerebrospinal fluid (CSF) β‑NGF in neurological disorders can be as low as 20–50 pg/mL, requiring the kit's 16 pg/mL sensitivity to detect changes .
• Cell culture supernatants (from Schwann cells, fibroblasts, cancer cells) often secrete β‑NGF in the 50–500 pg/mL range, again easily captured by the standard curve.
• The 31.25–2000 pg/mL linear range ensures that even high‑abundance samples (e.g., inflamed tissue homogenates) can be accurately quantified after appropriate dilution.
Critical step: The standard must be reconstituted accurately, diluted in the same matrix as your samples (e.g., assay buffer for cell supernatants, diluted serum/plasma for clinical samples), and run on every plate to control for inter‑plate variability.
The Workflow That Delivers a Publication‑Ready pg/mL Value in One Afternoon
- Sample preparation
• Serum/plasma: Collect using standard venipuncture; centrifuge to remove cells; aliquot and freeze at ‑80°C; avoid repeated freeze‑thaw (≤2 cycles).• Cerebrospinal fluid (CSF): Centrifuge to remove debris; assay immediately or freeze at ‑80°C.• Tissue homogenates: Homogenize tissue in cold PBS or RIPA buffer with protease inhibitors; centrifuge at 10,000 × g for 10 min; use supernatant.• Cell culture supernatant: Centrifuge to remove debris; assay immediately or freeze at ‑80°C.• Dilution: Pre‑dilute samples in assay buffer to bring expected β‑NGF concentration into the 31.25–2000 pg/mL range (typical serum/CSF dilution: 1:2–1:5; supernatant: neat or 1:2). - Assay procedure (typical 3.5‑h protocol)
• Step 1 (30 min): Add 100 µL of standard or sample to pre‑coated wells; incubate at 37°C.• Step 2 (1 h): Wash 3×; add 100 µL biotinylated detection antibody; incubate at 37°C.• Step 3 (30 min): Wash 3×; add 100 µL streptavidin‑HRP; incubate at 37°C.• Step 4 (15–20 min): Wash 3×; add 100 µL TMB substrate; incubate at room temperature, protected from light, until blue color develops (typically 10–20 min).• Step 5: Add 50 µL stop solution (turns yellow); read OD450 nm within 30 min. - Data analysis
• Plot OD450 (y‑axis) vs. standard concentration (x‑axis) using a 4‑parameter logistic (4PL) curve fit (most ELISA analysis software does this automatically).• Interpolate sample concentrations from the curve; multiply by the dilution factor to obtain the original sample concentration in pg/mL.
What Actually Changes When Your β‑NGF Data Is a pg/mL Number Instead of a Gel Band
① Your "NGF is upregulated" claim becomes a quantitative, statistically testable biomarker.
You can now write:
Serum β‑NGF levels were quantified using a sandwich ELISA (EliKine™ Human β‑NGF ELISA Kit, KTE6028; Abbkine). Samples were diluted 1:2 in assay buffer and measured in duplicate. The mean concentration in the neuropathic pain cohort was 145.3 ± 22.7 pg/mL versus 32.1 ± 8.4 pg/mL in healthy controls (p < 0.001, Student's t‑test).
That sentence turns "NGF expression was increased in patient sera by Western blot" into "Circulating β‑NGF was elevated 4.5‑fold in patients, with a ROC‑AUC of 0.89 for distinguishing disease from control."
② You can track β‑NGF dynamics across time‑courses and treatment responses.
Because ELISA is high‑throughput (96‑well format) and precise (CV <9%), you can run longitudinal serum/CSF draws from the same patient (pre‑treatment, on‑treatment, post‑relapse) or dose‑response curves of TrkA inhibitors (e.g., larotrectinib, entrectinib) and get pg/mL resolution that shows whether the drug is actually modulating circulating β‑NGF.
③ Your mechanistic study gains a soluble‑factor dimension that complements IHC and qPCR.
β‑NGF functions extracellularly. A tissue IHC shows where it's produced; qPCR shows mRNA levels; but only a serum/CSF/supernatant ELISA tells you how much secreted, bioactive protein is actually present in the microenvironment. That soluble concentration is what drives neurite outgrowth, nociceptor sensitization, and immune‑cell recruitment in real time.
The Bench Rules That Keep Your Standard Curve Linear and Your CV <9%
Rule Why It Matters
🧪 Use the same dilution matrix for standards and samples Matrix effects (serum proteins, supplements) can shift the curve; dilute standards in assay buffer spiked with equivalent dilution of normal serum if measuring serum samples.
🔬 Run samples in duplicate (minimum) or triplicate (ideal) ELISA is a binding assay; duplicates catch pipetting errors and edge effects.
⏱️ Keep incubation times consistent across wells HRP‑TMB development is time‑sensitive; use a timer and add stop solution in the same order as TMB addition.
🌡️ Equilibrate all reagents to room temperature (20–25°C) before use Cold reagents increase viscosity, causing pipetting errors and uneven binding.
🚫 Do not reuse tips or wells Carry‑over contamination kills precision.
📊 Include a blank (zero standard) and a positive control (if available) Blank sets the baseline; positive control monitors inter‑assay reproducibility.
Where KTE6028 Earns Its Place in the Paper's Biomarker or Mechanism Figure
Research Context Why a Sensitive, Quantitative β‑NGF ELISA Is Non‑Negotiable
Neurodegenerative diseases (Alzheimer's, Parkinson's) CSF β‑NGF is a potential biomarker for cholinergic dysfunction; levels may correlate with disease progression and cognitive decline .
Chronic pain & neuroinflammation Serum β‑NGF is elevated in osteoarthritis, neuropathic pain, migraine; quantitation is essential for drug‑response studies (anti‑NGF antibodies like tanezumab) .
Cancer biology & tumor innervation β‑NGF secreted by the tumor microenvironment drives axonogenesis and perineural invasion; measuring β‑NGF in tumor homogenates or patient serum can stratify prognosis and therapeutic response .
Diabetic neuropathy & peripheral nerve injury Local β‑NGF levels regulate Schwann cell migration, axon regeneration, and remyelination; quantitative tracking is key for neurorestorative therapy evaluation .
Psychiatric disorders (depression, PTSD) Serum β‑NGF may reflect neurotrophic support imbalance; sensitive ELISA allows correlation with symptom severity and treatment outcome .
Drug development (TrkA inhibitors, NGF‑neutralizing antibodies) IC₅₀/EC₅₀ determinations require precise concentration‑response curves; KTE6028 provides the pg/mL resolution needed for potency ranking.
Cell‑based assays (neurite outgrowth, PC12 differentiation) Quantify β‑NGF secretion into supernatant under different stimuli (NGF, BDNF, cytokines).
A Drop‑In Methods Paragraph
β‑NGF protein concentration in cell culture supernatants and human serum was quantified using a sandwich ELISA (EliKine™ Human β‑NGF ELISA Kit, KTE6028; Abbkine). Samples were diluted 1:2–1:5 in assay buffer to fall within the standard curve range (31.25–2000 pg/mL). Standards and samples (100 µL/well) were added to anti‑β‑NGF pre‑coated 96‑well plates and incubated at 37°C for 30 min. After washing, biotinylated detection antibody (100 µL/well) was added and incubated for 1 h at 37°C, followed by streptavidin‑HRP (30 min, 37°C). Plates were washed again, TMB substrate was added, and the reaction was stopped after 15 min with stop solution. Absorbance was read at 450 nm on a microplate reader. Concentrations were interpolated from a 4‑parameter logistic standard curve and multiplied by the dilution factor to obtain final pg/mL values.
Explore the EliKine™ Human β‑NGF ELISA Kit (KTE6028) full specifications, validation data, and ordering options here:
🔗 https://www.abbkine.com/product/elikine-human-%ce%b2-ngf-elisa-kit-kte6028/
(For research use only. Not for human or clinical diagnostic use. Store components at 2–8°C or ‑20°C as indicated; avoid repeated freeze‑thaw of samples and standards; run standards and samples in duplicate; use the same dilution matrix for both standards and samples to minimize matrix effects.)





