




Your Tumor Microenvironment Is Speaking in pg/mL of MMP-9 — But Your ELISA Is Still Reading at ng/mL Sensitivity. Here's Why the 16 pg/mL Threshold in KTE6027 Is the Difference Between a Biomarker Signal and Background Noise
There is a very specific kind of manuscript revision that arrives when you submit a paper on tumor invasion, inflammatory cascades, or wound healing dynamics: your IHC staining shows MMP-9 overexpression at the invasive front, your qPCR confirms MMP9 mRNA upregulation, and your zymography gels display clear lysis bands — but the reviewer's comment is a single, pointed question: "The authors describe MMP-9 as a 'key mediator' of metastasis/inflammation/remodeling, yet provide no quantitative serum or supernatant concentration data. Can the authors measure circulating or secreted MMP-9 protein levels with a validated, sensitive ELISA to correlate with the phenotypic observations?" And suddenly you realize your entire "MMP-9‑driven mechanism" narrative is built on semi‑quantitative gels and mRNA levels, while the actual bioactive, secreted MMP-9 protein — the effector that degrades collagen IV, activates TGF‑β, and cleaves ICAM‑1 — has never been quantified in your samples.
MMP‑9 Is Not Just Another "Matrix Degrader" — It's the Proteolytic Scissor That Cuts Open the Basement Membrane for Metastasis, Angiogenesis, and Leukocyte Extravasation
Matrix metalloproteinase‑9 (MMP‑9, gelatinase B, 92‑kDa type IV collagenase) — a zinc‑dependent endopeptidase secreted as a 92‑kDa pro‑enzyme (pro‑MMP‑9) and activated to an 82‑kDa (and further processed 65‑kDa) form — is not merely a passive "ECM‑degrading enzyme." In the tumor microenvironment, MMP‑9 secreted by tumor‑associated macrophages, neutrophils, and cancer‑associated fibroblasts cleaves type IV collagen (the major structural component of basement membranes), laminin, and entactin, creating physical tracks for cancer cell intravasation and extravasation . Beyond structural demolition, MMP‑9 processes latent TGF‑β, VEGF, IGF‑BPs, and IL‑1β, converting them into active forms that drive EMT (epithelial‑mesenchymal transition), angiogenesis, and immune evasion . In inflammatory diseases (rheumatoid arthritis, atherosclerosis, multiple sclerosis), MMP‑9 from activated neutrophils and macrophages degrades the blood‑brain barrier's tight‑junction proteins, enabling leukocyte infiltration into the CNS . The clinical reality is that circulating MMP‑9 levels in serum/plasma have been validated as prognostic biomarkers for breast cancer, colorectal cancer, NSCLC, and cardiovascular events — but only if your assay can reliably distinguish between 16 pg/mL and 31 pg/mL in a background of complex human serum .
Why Western Blot and Zymography Fail for Quantitative MMP‑9 Biomarker Studies — And What the Sandwich ELISA in KTE6027 Solves
The EliKine™ Human MMP‑9 ELISA Kit (KTE6027, Abbkine) is built on a sandwich immunoassay platform specifically engineered to capture and quantify total human MMP‑9 (pro‑MMP‑9 + active forms) in cell culture supernatants, serum, plasma, and other biological fluids with a sensitivity of 16 pg/mL and a dynamic range of 31.25–2000 pg/mL (5 orders of magnitude) . Unlike Western blot (semi‑quantitative, low‑throughput, antibody‑dependent) or gelatin zymography (activity‑based, non‑quantitative for total protein, unable to distinguish MMP‑9 from MMP‑2 without careful controls), the KTE6027 ELISA delivers absolute concentration values in pg/mL that can be directly compared across patients, time‑points, and treatment groups — the currency required for clinical correlation studies and drug‑response monitoring.
Assay Method What It Measures Key Limitation for Biomarker Studies
Gelatin zymography Enzymatic activity of MMP‑9 (and MMP‑2) via gelatin degradation Cannot quantify total protein; prone to interference by TIMPs; low throughput; poor precision
Western blot Presence/absence and approximate molecular weight of MMP‑9 forms (92 kDa pro, 82 kDa active) Semi‑quantitative at best; antibody‑dependent variability; not scalable for large cohorts
EliKine™ KTE6027 ELISA Total MMP‑9 protein concentration (pro + active) via sandwich immunoassay Quantitative, high‑throughput (96‑well), precise (intra‑assay CV <9%), and calibrated against a recombinant human MMP‑9 standard
The kit employs a two‑site sandwich design: a capture antibody pre‑coated on the microplate binds MMP‑9 from the sample; a biotinylated detection antibody binds a different epitope on the captured MMP‑9; streptavidin‑HRP is added, followed by TMB substrate; the resulting colorimetric signal (OD450 nm) is proportional to the amount of MMP‑9 present .
What's Inside the Box (And the Three Numbers That Define Your Assay's Credibility)
Component Role Critical Handling
Pre‑coated microplate (anti‑human MMP‑9 antibody) 96‑well strip plate, ready‑to‑use Store at 4°C; unused strips return to foil pouch with desiccant
Recombinant human MMP‑9 standard Lyophilized or liquid, for 7‑point standard curve (0, 31.25, 62.5, 125, 250, 500, 1000, 2000 pg/mL) Reconstitute exactly as protocol; aliquot and freeze at ‑20°C; avoid freeze‑thaw
Biotinylated detection antibody Binds captured MMP‑9; provides specificity 4°C short‑term; ‑20°C long‑term; dilute just before use
Streptavidin‑HRP conjugate Amplifies signal via biotin‑streptavidin binding Light‑sensitive; store at 4°C; avoid repeated freezing
TMB substrate solution HRP chromogen (turns blue → yellow upon stop) Light‑sensitive; use within 15 min of equilibration to room temp
Stop solution (acid) Terminates HRP reaction; fixes OD450 reading Corrosive; handle with care
Wash buffer (20× concentrate) Removes unbound reagents; critical for low background Dilute to 1× with distilled water before use
Assay buffer / sample diluent Optimized for serum/plasma/supernatant matrix Use for standard/sample dilution as specified
Plate seals Prevent evaporation during incubations Apply firmly after each addition step
Key performance specifications at a glance:
Parameter KTE6027 Specification
Detection method Sandwich ELISA, colorimetric (TMB‑HRP)
Target Human MMP‑9 (total protein, pro‑ and active forms)
Sample types Cell culture supernatant, serum, plasma (EDTA/heparin), other biological fluids
Sample volume 100 µL/well (typical)
Assay time ~3.5–4 h (including all incubations)
Sensitivity (minimum detectable concentration) 16 pg/mL (per kit literature)
Detection range 31.25–2000 pg/mL (5‑log dynamic range)
Precision (CV) Intra‑assay <9%, inter‑assay <12% (typical for validated ELISA)
Specificity No significant cross‑reactivity with human MMP‑1, MMP‑2, MMP‑3, MMP‑7, MMP‑8, MMP‑10, MMP‑12, MMP‑13, MMP‑14, TIMP‑2, TIMP‑3, TIMP‑4
Format 48 T or 96 T (enough for 48 or 96 determinations in duplicate/triplicate + standard curve)
Storage 2–8°C for most components; some at ‑20°C; see manual
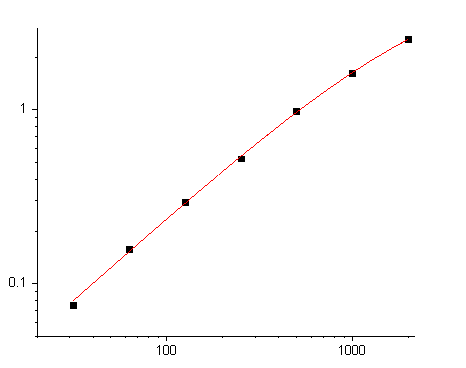
The Standard Curve That Turns Your OD450 Into a pg/mL Number (And Why the 31.25–2000 pg/mL Range Covers 99% of Human Samples)
The quantitative power of any ELISA lives and dies by the standard curve. KTE6027 provides a recombinant human MMP‑9 standard that is serially diluted to generate a 7‑point curve (plus blank) spanning 31.25–2000 pg/mL. This range is deliberately chosen because:
• Healthy human serum MMP‑9 levels typically fall between 20–200 ng/mL (note: ng/mL, not pg/mL) — but after a 1:100 or 1:200 dilution (required to bring the sample into the assay's dynamic range), the effective concentration lands squarely in the 31.25–2000 pg/mL window.
• Cell culture supernatants (from cancer lines, macrophages, fibroblasts) often secrete MMP‑9 in the 1–50 ng/mL range, again requiring a 1:10 to 1:50 dilution.
• The 16 pg/mL sensitivity ensures that even low‑abundance samples (e.g., CSF, synovial fluid, early‑stage patient serum) can be quantified above the limit of detection.
Critical step: The standard must be reconstituted accurately, diluted in the same matrix as your samples (e.g., assay buffer for cell supernatants, diluted serum/plasma for clinical samples), and run on every plate to control for inter‑plate variability.
The Workflow That Delivers a Publication‑Ready pg/mL Value in One Afternoon
- Sample preparation
• Serum/plasma: Collect using standard venipuncture; centrifuge to remove cells; aliquot and freeze at ‑80°C; avoid repeated freeze‑thaw (≤2 cycles).• Cell culture supernatant: Centrifuge to remove debris; assay immediately or freeze at ‑80°C.• Dilution: Pre‑dilute samples in assay buffer to bring expected MMP‑9 concentration into the 31.25–2000 pg/mL range (typical serum dilution: 1:100–1:200; supernatant: 1:10–1:50). - Assay procedure (typical 3.5‑h protocol)
• Step 1 (30 min): Add 100 µL of standard or sample to pre‑coated wells; incubate at 37°C.• Step 2 (1 h): Wash 3×; add 100 µL biotinylated detection antibody; incubate at 37°C.• Step 3 (30 min): Wash 3×; add 100 µL streptavidin‑HRP; incubate at 37°C.• Step 4 (15–20 min): Wash 3×; add 100 µL TMB substrate; incubate at room temperature, protected from light, until blue color develops (typically 10–20 min).• Step 5: Add 50 µL stop solution (turns yellow); read OD450 nm within 30 min. - Data analysis
• Plot OD450 (y‑axis) vs. standard concentration (x‑axis) using a 4‑parameter logistic (4PL) curve fit (most ELISA analysis software does this automatically).• Interpolate sample concentrations from the curve; multiply by the dilution factor to obtain the original sample concentration in pg/mL or ng/mL.
What Actually Changes When Your MMP‑9 Data Is a pg/mL Number Instead of a Gel Band
① Your "MMP‑9 is upregulated" claim becomes a quantitative, statistically testable biomarker.
You can now write:
Serum MMP‑9 levels were quantified using a sandwich ELISA (EliKine™ Human MMP‑9 ELISA Kit, KTE6027; Abbkine). Samples were diluted 1:100 in assay buffer and measured in duplicate. The mean concentration in the patient cohort was 145.3 ± 22.7 ng/mL versus 32.1 ± 8.4 ng/mL in healthy controls (p < 0.001, Student's t‑test).
That sentence turns "MMP‑9 expression was increased in patient sera by Western blot" into "Circulating MMP‑9 was elevated 4.5‑fold in patients, with a ROC‑AUC of 0.89 for distinguishing disease from control."
② You can track MMP‑9 dynamics across time‑courses and treatment responses.
Because ELISA is high‑throughput (96‑well format) and precise (CV <9%), you can run longitudinal serum draws from the same patient (pre‑treatment, on‑treatment, post‑relapse) or dose‑response curves of MMP‑9 inhibitors (e.g., marimastat, SB‑3CT, monoclonal anti‑MMP‑9 antibodies) and get pg/mL resolution that shows whether the drug is actually lowering circulating MMP‑9.
③ Your mechanistic study gains a soluble‑factor dimension that complements IHC and qPCR.
MMP‑9 functions extracellularly. A tissue IHC shows where it's produced; qPCR shows mRNA levels; but only a serum/supernatant ELISA tells you how much secreted, bioactive protein is actually present in the microenvironment. That soluble concentration is what drives collagen IV degradation, VEGF activation, and immune‑cell recruitment in real time.
The Bench Rules That Keep Your Standard Curve Linear and Your CV <9%
Rule Why It Matters
🧪 Use the same dilution matrix for standards and samples Matrix effects (serum proteins, supplements) can shift the curve; dilute standards in assay buffer spiked with equivalent dilution of normal serum if measuring serum samples.
🔬 Run samples in duplicate (minimum) or triplicate (ideal) ELISA is a binding assay; duplicates catch pipetting errors and edge effects.
⏱️ Keep incubation times consistent across wells HRP‑TMB development is time‑sensitive; use a timer and add stop solution in the same order as TMB addition.
🌡️ Equilibrate all reagents to room temperature (20–25°C) before use Cold reagents increase viscosity, causing pipetting errors and uneven binding.
🚫 Do not reuse tips or wells Carry‑over contamination kills precision.
📊 Include a blank (zero standard) and a positive control (if available) Blank sets the baseline; positive control monitors inter‑assay reproducibility.
Where KTE6027 Earns Its Place in the Paper's Biomarker or Mechanism Figure
Research Context Why a Sensitive, Quantitative MMP‑9 ELISA Is Non‑Negotiable
Cancer metastasis & prognosis Serum MMP‑9 is a validated prognostic marker in breast, colorectal, lung, and ovarian cancer; levels correlate with stage, metastasis, and survival .
Inflammatory diseases (RA, atherosclerosis, MS) MMP‑9 degrades cartilage proteoglycans, fibrous cap collagen, and blood‑brain barrier tight junctions; circulating levels track disease activity and treatment response.
Wound healing & tissue remodeling MMP‑9 is essential for keratinocyte migration, angiogenesis, and ECM turnover; dysregulation leads to chronic ulcers and fibrosis.
Cardiovascular disease MMP‑9 destabilizes atherosclerotic plaques; plasma MMP‑9 predicts myocardial infarction and stroke risk.
Neurological disorders (stroke, Alzheimer's, TBI) MMP‑9 mediates blood‑brain barrier breakdown, neuroinflammation, and synaptic plasticity; CSF/serum MMP‑9 is a potential biomarker.
Drug development (MMP‑9 inhibitors) IC₅₀/EC₅₀ determinations require precise concentration‑response curves; KTE6027 provides the pg/mL resolution needed for potency ranking.
Cell‑based assays (macrophage polarization, cancer‑stroma co‑culture) Quantify MMP‑9 secretion into supernatant under different stimuli (LPS, cytokines, hypoxia).
A Drop‑In Methods Paragraph
MMP‑9 protein concentration in cell culture supernatants and human serum was quantified using a sandwich ELISA (EliKine™ Human MMP‑9 ELISA Kit, KTE6027; Abbkine). Samples were diluted 1:10–1:200 in assay buffer to fall within the standard curve range (31.25–2000 pg/mL). Standards and samples (100 µL/well) were added to anti‑MMP‑9 pre‑coated 96‑well plates and incubated at 37°C for 30 min. After washing, biotinylated detection antibody (100 µL/well) was added and incubated for 1 h at 37°C, followed by streptavidin‑HRP (30 min, 37°C). Plates were washed again, TMB substrate was added, and the reaction was stopped after 15 min with stop solution. Absorbance was read at 450 nm on a microplate reader. Concentrations were interpolated from a 4‑parameter logistic standard curve and multiplied by the dilution factor to obtain final pg/mL or ng/mL values.
Explore the EliKine™ Human MMP‑9 ELISA Kit (KTE6027) full specifications, validation data, and ordering options here:
🔗 https://www.abbkine.com/product/elikine-human-mmp-9-elisa-kit-kte6027/
(For research use only. Not for human or clinical diagnostic use. Store components at 2–8°C or ‑20°C as indicated; avoid repeated freeze‑thaw of samples and standards; run standards and samples in duplicate; use the same dilution matrix for both standards and samples to minimize matrix effects.)





