




The 28-kDa Heterodimer That Diagnoses With a Single Decimal: Why TSH's Shared-Alpha-Subunit Trick Makes the Sandwich ELISA a Precision Instrument — And How KTE6905 Finally Lets You Trust the "Sensitive" in Sensitive TSH
There is exactly one number that decides whether your thyroid workup lives in the subclinical gray zone (TSH 4.5–10 mIU/L, patient feels vaguely awful, imaging is equivocal) or unambiguously crosses into overt hypothyroidism (TSH > 10, T4 already slipping) — and that number is not T4, not T3, and certainly not a "low-energy" self-diagnosis. It's Thyroid-Stimulating Hormone (TSH / thyrotropin), the ~28 kDa heterodimeric glycoprotein secreted by the basophilic thyrotrophs of the anterior pituitary, whose entire evolutionary job is to act as the ultra-sensitive inverse voltmeter of circulating free thyroid hormone: FT4 ↓ → pituitary upregulates TRH → TSH ↑ (sometimes 10–100× normal before FT4 is even clearly abnormal); FT4 ↑ → TSH suppressed → feedback loop closes. What trips most people up, though, is the structural twist: TSH shares its α-subunit (92 aa, identical to LH, FSH, and hCG) with every other pituitary glycoprotein hormone — which means any immunoassay that accidentally grabs the α-face instead of the TSH-unique β-subunit (118 aa, Gene ID: 1081 / TSHB, UniProt P01215) is a specificity disaster. The EliKine™ Human TSH ELISA Kit (KTE6905) from Abbkine is engineered specifically around that β-subunit discrimination: a double-antibody sandwich ELISA with pre-coated anti-TSH capture mAb → HRP-labeled detection Ab → TMB → 450 nm, delivering a 0.3–12 mIU/L working range with LOD ~0.1 mIU/L, so your subclinical detection, environmental thyroid-disruptor screen, or longitudinal endocrine panel rests on a plate-interpolated mIU/L, not a "TSH looked high on the chemiluminescence printout" that you can't reproduce at your own bench.
TSH in One Paragraph: The α/β Heterodimer Whose "Secret Identity" Is Hidden in Plain Sight
TSH (thyrotropin, TRH → pituitary thyrotroph → stored in secretory granules → basophilic staining) is a member of the cysteine-knot glycoprotein hormone family:
Feature Detail Why It Matters for Assay Design
α-subunit (92 aa, ~14.5 kDa) Identical sequence to LH, FSH, hCG (gene: CGA, UniProt P01160) This is the trap — any antibody that sees only α can't tell TSH from hCG/LH/FSH
β-subunit (TSHB, 118 aa, ~15 kDa, glycosylated ~18–22 kDa) Unique to TSH — its folded surface determines receptor binding (TSHR) The only safe immunoassay target for specificity
Heterodimer (α+β, non-covalent, ~28 kDa total, heavily sialylated) Carbohydrate ~15–20% by weight → pI ~4.5–5.0 Glycoform micro-heterogeneity makes "one MW" misleading; epitope accessibility matters more
The hypothalamic–pituitary–thyroid (HPT) logic is the tightest endocrine negative-feedback loop in the body:
Cold / low FT4 → paraventricular nucleus releases TRH → thyrotrophs release TSH (pulsatile, ~8–12 pulses/night, amplitude ↑ in primary failure) → TSH binds TSHR on thyroid follicular cells → cAMP/PKA → TG iodination → T3/T4 release → FT4/FT3 inhibit TRH & TSH.
The clinical numbers everyone memorizes — and the reason "sensitivity" is everything for this assay:
State Serum TSH (mIU/L) Interpretation
Suppressed (exogenous T4, Graves, central hypopituitarism) < 0.1–0.4 The 0.1 mIU/L floor is exactly why your kit LOD must be ≤ 0.1
Euthyroid reference (population median) ~0.5–2.5 (lab-specific, ~0.4–4.0 acceptance)
Subclinical hypothyroidism 4.5–10 (FT4 still normal) The diagnostic controversy zone
Overt primary hypothyroidism > 10 (often > 50–100) Clear-cut; levothyroxine indicated
Why the "Shared α-Subunit" Architecture Demands a β-Subunit–Specific Sandwich (And Why KTE6905 Is Built That Way)
The specificity problem is not theoretical — it's structural. LH, FSH, hCG, and TSH all display the same α-subunit on their surface. Any capture/detection pair that recognizes an α-common epitope will report TSH + LH + hCG + FSH = nonsense in pregnancy or mid-cycle.
The solution is the same one clinical immunoassay engineers have used since the third-gen TSH assays arrived in the 1990s:
Direct both capture and detection antibodies (or at minimum the detection arm) toward the TSHB-unique β-subunit conformational/linear epitopes, so the readout sees TSH and ignores the α-sharing crowd.
The KTE6905 architecture does exactly this via the classic sandwich:
- Microplate pre-coated with a high-affinity anti-human TSH mAb (β-subunit–directed, optimized to capture the intact α/β heterodimer without cross-grabbing free α or other glycoprotein hormones).
- Standard (WHO-standard-traceable human TSH) + samples — serum, plasma (EDTA/heparin/citrate), other biological fluids — added → TSH captured.
- Wash → HRP-labeled anti-TSH detection antibody (different β-subunit epitope) → TMB → stop → 450 nm → interpolate TSH concentration (mIU/L) from the 4-PL standard curve.
- Kit components (per distributed specs): pre-coated plate, lyophilized/liquid TSH standard gradient, detection Ab–HRP, substrate A/B, stop solution, wash buffer, plate sealer.
From the consolidated Abbkine / distributor data for KTE6905 :
Parameter KTE6905 / EliKine™ Specification
Target Human TSH / Thyrotropin (α+β heterodimer; TSHB UniProt P01215, Gene ID 1081)
Format Double-antibody sandwich ELISA, pre-coated capture (夹心法)
Detection HRP-conjugate detection Ab → TMB, 450 nm
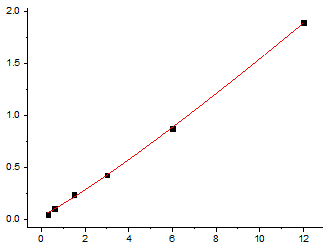
Dynamic Range 0.3 – 12 mIU/L
Sensitivity / LOD ~0.1 mIU/L
Intra-Assay CV < 8%
Inter-Assay CV < 10%
Specificity No significant cross-reactivity with LH, FSH, hCG at physiological levels (β-subunit–specific recognition)
Samples Serum, plasma (EDTA / heparin / sodium citrate), other biological fluids / cell culture supernatants
Assay time ~2.5–3.5 hours
Storage 2–8°C, sealed plate strips 4°C, lyophilized standard stable until reconstitution
(Confirm exact dilution factors, standard traceability (NIBSC/WHO 81/565 or equivalent), and lot-specific recovery on the shipped CoA/datasheet for KTE6905.)
The Collection Rule: Serum First, EDTA OK, Citrate Acceptable — But Never a Hemolyzed Mess
TSH is stable at 4°C for 24–48 h and at -20°C for months (it's a glycoprotein, not a fragile 1-kDa peptide), but the practical enemies are:
- Hemolysis — free hemoglobin can mildly interfere with some peroxidase readouts and shifts baseline OD if you're careless.
- Prolonged room-temp standing — not because TSH degrades fast, but because cellular metabolism in unspun blood can micro-shift other analytes that contextualize your endocrine panel.
- Fasting? Strictly speaking TSH is not fasting-dependent the way insulin is — but labs standardise it because circadian rhythm matters: TSH pulses are higher nocturnally / pre-dawn (02:00–06:00) and trough around afternoon; a 08:00 standardized draw is the universal default.
Quick protocol:
• Serum preferred (clot tube, spin ≥ 2,000 ×g, 10 min, 4°C, aliquot, -20/ -80°C).
• EDTA plasma works and is often used in research cohorts already drawn for other panels.
• Warm kit reagents ≥ 30 min RT before opening; protect TMB; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate.
Where TSH Quantification Actually Carries the Paper
- Subclinical Hypothyroidism & the 4.5–10 mIU/L Gray Zone (Where Most Diagnoses Live or Die)
This is the real-world battleground. Population data (NHANES and European lab consensus) keeps shifting the upper-limit reference downward — from 5.0 → 4.5 → even 2.5 in some "functional" definitions — which means the 0.1 mIU/L sensitivity of KTE6905 isn't academic; it's what lets you reliably score samples in the suppressed range (< 0.1–0.4) versus the equivocal fence (2.5–4.5) without the signal drowning in noise. If your study claims "10% of this cohort was subclinical," the CVs behind that claim better be < 8%.
- Environmental Thyroid Disruptor Screens (EDCs, Bisphenols, PFAS, Perchlorate)
This is where the assay earns its research stripes. PFAS (PFOA/PFOS) and perchlorate (ClO₄⁻, iodide transport inhibitor) both act on the thyroid axis — often subtly, pushing TSH 1–3 mIU/L above baseline without crashing FT4 into overt territory. Running KTE6905 on banked EDTA plasma from exposed vs. referent communities (paired with FT4, FT3, urinary iodine, perchlorate/PFAS LC-MS) gives you the endocrine dose–response with TSH as the canary, not just a statistical residual.
- Pregnancy & the hCG Cross-Talk (Why β-Subunit Specificity Is Non-Negotiable)
First-trimester hCG peaks 50,000–100,000 mIU/mL — and because hCG shares the α-subunit and even has weak TSHR (thyrotropic) activity at those concentrations, a poorly designed TSH assay that sees α-common epitopes reads hCG as "fake TSH" and spuriously inflates the number. KTE6905's β-subunit–specific sandwich is what prevents that: it reads TSHB, not hCGβ/α, keeping the pregnancy first-trimester curve honest. The clinical context: gestational hypothyroidism / overt hyperthyroidism of pregnancy (hCG-induced thyrotoxicosis transient) — getting TSH right matters for fetal neurodevelopment (especially weeks 12–20 before fetal thyroid is independent).
- Central / Secondary Hypothyroidism (Pituitary–Axis Failure) — The Dangerous "Normal TSH" Trap
In Sheehan's, pituitary adenoma, hypothalamic surgery, or irradiation, the thyrotrophs die — so TSH is LOW or inappropriately normal despite FT4 being low. The only clue is the pattern: FT4 ↓ + TSH not ↑ (often < 0.5–1.0, and critically lack of pulsatile amplitude). An assay that can resolve 0.1 mIU/L increments and produce a plate-read number lets you track TRH-stimulation testing or recovery post-treatment (e.g., post-transsphenoidal resection) with actual digits instead of a qualitative "low."
- Longitudinal Aging & "Reference Range Creep" Studies
TSH increases ~0.03 mIU/L per year after age ~40–50 in many populations (reduced thyroid reserve, accumulated autoimmunity/TgAb/TPOAb, vascular micro-ischemia of thyrotrophs). Large cohort biobanks use plate-based TSH (with standardized draws and cold-chain) to model incident subclinical hypo and its link to dyslipidemia, depression, frailty, and cognitive decline — the kind of associational architecture that needs CVs you can defend.
- Assay Validation / Method-Comparison in Research Labs
If your lab is transitioning from a send-out CLIA chemiluminescence (Beckman Access / Roche Cobas / Abbott Architect) to in-house ELISA work (budget, batching, independence from analyzer contracts), KTE6905 gives you the correlation slope across 40–60 paired sera: ELISA mIU/L = slope × CLI_mIU/L + intercept, with Deming regression and Bland–Altman bias plot proving the home assay is fit for purpose. That's a one-page Methods/Supplementary that unlocks all your future thyroid work.
The Bottom Line
TSH is the ~28-kDa α/β heterodimeric glycoprotein whose α chain is a deliberate copy-paste shared with LH, FSH, and hCG — which means the only defensible immunoassay for it is one that locks onto the TSH-unique β-subunit (TSHB) with both capture and detection arms and ignores the crowd. The EliKine™ Human TSH ELISA Kit — KTE6905 from Abbkine is built exactly for that job: pre-coated anti-TSH capture (β-directed) → HRP detection Ab (second β epitope) → TMB → 450 nm → interpolated mIU/L, over a 0.3–12 mIU/L calibrated range with LOD ~0.1 mIU/L (Intra CV < 8%, Inter CV < 10%), in a ~2.5–3.5 hour workflow compatible with serum, EDTA/heparin/citrate plasma, and other biological fluids — so your subclinical thyroid, environmental disruptor, or pregnancy-screening paper stands on plate-read numbers, not a reference-lab printout you can't repeat.
Product Reference: KTE6905 – EliKine™ Human TSH (Thyroid Stimulating Hormone) ELISA Kit
Learn more and order: https://www.abbkine.com/product/elikine-human-tsh-elisa-kit-kte6905/
(For Research Use Only; not for diagnostic procedures in humans.)





