




The 290-kDa Molybdenum Engine That Crystallizes Kidneys and Colors Your Mouse's Pee Yellow: Why Tracking XDH/XOR Protein Mass — Not Just Uric Acid — Changes the Entire Ischemia–Reperfusion Story
Every mouse model of cardiac arrest, renal I/R, or hyperuricemia eventually runs the same lazy sentence: "uric acid levels were elevated, confirming xanthine oxidase activity." But that sentence buries the real problem — because uric acid is the exhaust of the reaction, not the enzyme that made it, and unless you know how much XDH/XOR (xanthine dehydrogenase/oxidase, often called XO, XOR, or XOD) protein was actually there, your "↑UA" could mean more enzyme, sulfhydryl-converted enzyme, or just more substrate backing up from ATP catabolism. The enzyme in question is a ~290–300 kDa homodimer (each ~1333-aa subunit = UniProt Q00519, Gene ID 22436 / Xdh, Chr 17) carrying three absurdly exotic cofactors — molybdopterin (Mo), FAD, and two [2Fe-2S] clusters — that let it run the two-step late-purine ladder: hypoxanthine → xanthine → uric acid, while also leaking superoxide (O₂⁻) and H₂O₂ through the oxidase (O₂-acceptor) mode that makes it the single most cited source of reperfusion ROS in cardiovascular and renal pathophysiology. The Mouse Xanthine dehydrogenase/oxidase (XDH) ELISA Kit (KTE70003) from Abbkine gives you this molybdoprotein as a calibrated sandwich-ELISA variable (0.156–10 ng/mL, LOD ~0.078 ng/mL) — so your I/R, gout-model, or allopurinol/drug-screen paper finally has the enzyme-mass denominator instead of a yellow pigment proxy.
XDH/XOR in One Paragraph: The Mo–FAD–[2Fe-2S] Homodimer That Is Both NAD⁺-Saver and ROS-Faucet
The systematic name is xanthine oxidoreductase (XOR), because the same polypeptide exists in two interconvertible states:
State EC # Electron Acceptor Localization / Trigger What It Means
XDH (dehydrogenase, "good" form) 1.17.1.4 NAD⁺ → NADH (at a pterin-loop site adjacent to the molybdenum center) Baseline: Cys⁵³¹ (mouse numbering context) in the flexible "hinge" peptide is reduced / intact, keeping the enzyme tethered to NAD⁺ Produces uric acid without directly handing electrons to O₂
XO (oxidase, "bad" form) 1.17.3.2 O₂ → O₂⁻/H₂O₂ Triggered by reversible sulfhydryl oxidation (Cys–SO₂⁻/SO₃⁻) or irreversible proteolytic cleavage of the hinge peptide (calpains, cathepsins, trypsin-like proteases activated during ischemia/inflammation) Now every purine it processes bleeds superoxide into the cytosol/mitochondrial fringe → amplifies reperfusion injury
The three substrates/products everyone memorizes:
Hypoxanthine + H₂O + NAD⁺ → xanthine + NADH + H⁺ (D1)
Xanthine + H₂O + NAD⁺ → uric acid + NADH + H⁺ (D2)
Switch to XO mode: same reactions, but O₂ replaces NAD⁺ as acceptor → net O₂⁻ + H₂O₂ per turnover.
Subcellularly, XOR is synthesized as a 146 kDa monomer (computed, highly glycosylated in mature forms), assembles into the functional homodimer (290–300 kDa), and distributes across cytosol, peroxisome-associated pools, and a small secretable/extracellular fraction (it can be detected in plasma at trace levels, partly from endothelial/hepatic release, partly from cell turnover).
Why a Sandwich ELISA — And Why "Uric Acid = XO Activity" Is the Original Category Error
Three reasons the gel/WB-only approach fails here:
- XDH and XO are the same polypeptide — the only difference is post-translational redox state + hinge cleavage. A UA dipstick can't tell you whether the pool is native XDH (NAD⁺-coupled) vs. converted XO (ROS-leaking); you need either activity-ratio assays (NAD⁺ vs. O₂ acceptor, inhibitor-sensitive) or the total XOR protein mass as the canvas those activities paint on.
- XDH runs at the ~130–150 kDa monomer zone (dimer ~290) near the heavy membrane/glycoprotein smear; "band vs. actin" densitometry is fine for a figure but not for a 40-sample cohort with CVs you can defend.
- Your experiment is a time-course (0 h, 2 h, 6 h, 24 h post-clamp/reperfusion, or allopurinol 50 mg/kg vs. febuxostat 10 mg/kg) — that needs plate numbers, not a gel-strip.
The KTE70003 kit uses the field-standard two-site architecture:
- Microplate pre-coated with capture anti-mouse XDH/XOR (directed at a linear/conformational epitope conserved across the dehydrogenase/oxidase forms — so it reads total XOR immunoreactive mass, regardless of sulfhydryl state).
- Standards (recombinant/standardized mouse Xdh) + samples — serum, plasma, tissue homogenates, cell culture supernatants/lysates — added → XDH bound.
- Wash → biotinylated anti-XDH detection (different epitope) → Streptavidin–HRP → TMB → color ∝ bound XDH.
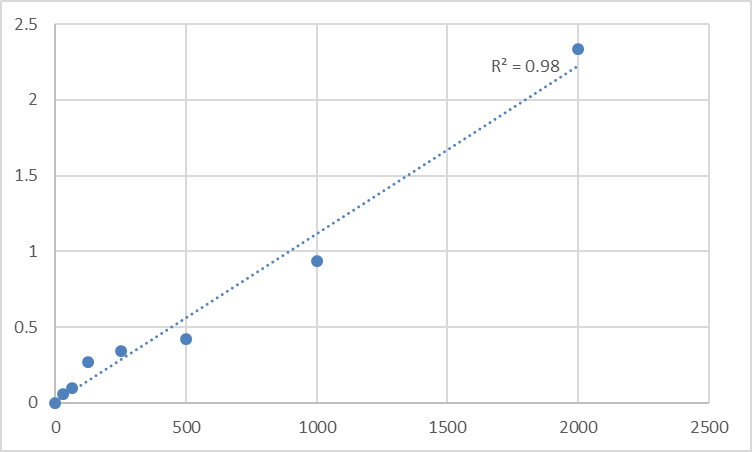
- Stop → 450 nm → interpolate ng/mL from the standard curve.
Consolidated specification envelope from the distributor/technical records aligned with KTE70003:
Parameter KTE70003-class Specification
Target Mouse XDH/XOR (Xanthine dehydrogenase/oxidase, XO/XOR/XOD; UniProt Q00519, Gene Xdh / 22436)
Format 96-well sandwich ELISA, pre-coated capture (夹心法)
Detection Biotin-Ab → SA–HRP → TMB, 450 nm
Dynamic Range 0.156 – 10 ng/mL (equivalently 31.2 – 2,000 pg/mL)
Sensitivity / LOD 0.078 ng/mL (15.6 pg/mL / ~12.1 pg/mL)
Intra-Assay CV < 8%
Inter-Assay CV < 10–10.2%
Specificity No significant cross-reactivity with other mouse oxidoreductases/analogues at physiological levels
Samples Serum, plasma (EDTA/heparin), tissue homogenates, cell culture supernatants/lysates, other biological fluids
Assay time ~3–5 hours
(Confirm exact dilution scheme, standard identity/traceability, and lot-specific recovery on the shipped Abbkine datasheet/CoA for KTE70003.)
The Prep Rule: XOR Is Cytoplasmic, ~300 kDa, and Loves Its Cofactors — So Respect the Buffer
Because XOR is large, glycosylated, and cofactor-rich, gentle is better:
• For tissue (heart, kidney cortex/medulla, liver): homogenize cold in 50 mM Tris pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100/NP-40 + protease inhibitors, keep on ice, optional brief sonication (low power, 2–3 pulses), spin 12,000–16,000 ×g, 15 min, 4°C → supernatant = your XOR-accessible pool → BCA → ng XDH / mg total protein.
• For serum/plasma: collect in EDTA (preferred), spin cold, aliquot, -80°C, avoid >1 freeze–thaw. XOR is stable enough, but prolonged RT causes the XDH→XO conversion to creep along ex vivo (exactly what you don't want artefactually inflating the "XO" fraction before you measure).
• Express as ng XDH / mg protein for tissue, or ng/mL for fluids.
Where XDH/XOR Quantification Actually Carries the Paper
- Ischemia–Reperfusion Injury (Heart, Kidney, Liver): The Original XO–ROS Narrative
This is the canonical. The sequence is: normoxia → ischemic ATP depletion → AMP/IMP buildup → purine catabolism to hypoxanthine (substrate accumulates) + Ca²⁺ rise → proteases activated → XOR hinge peptide cleaved/oxidized → XDH → XO conversion → reperfusion brings O₂ back → XO now has substrate (hypoxanthine/xanthine) + O₂ = superoxide/peroxynitrite party.
The rigorous figure set is:
• Total XOR protein (KTE70003, ng/mg) — the enzyme pool that exists to do damage
• XDH→XO ratio (activity assay: NAD⁺-dependent vs. O₂-dependent, ± allopurinol/wortmannin)
• MPO/TUNEL/infarct size or sCr/BUN (kidney)
• SOD2/MnSOD + GPx + GSH (antioxidant buffering)
That linkage — enzyme mass → conversion state → ROS → necrosis — is what upgrades a cardiac paper from "we gave oxypurinol and it improved" to "we measured the machinery that made the ROS."
- Hyperuricemia / Gout Models (Potassium Oxonate / Hx Loading & Allopurinol vs. Febuxostat)
The potassium oxonate (inhibits uricase → urate can't break down further in rodents, so UA accumulates visibly) + hypoxanthine diet is the classic mouse hyperuricemia model. But if you're testing a URAT1 inhibitor, febuxostat (non-purine XO selective), or SLC2A9/Glut9 transporter modifier, you need the XDH mass to show the model actually loaded the enzyme — not just "UA is high because we poisoned the liver." ELISA-quantified XDH in liver homogenate + kidney cortex (ng/mg) next to serum UA (uricase-inhibited model) is the biochemical floor.
- DMSO / Ethanol Toxicity & the "XOR-Shed" Hepatorenal Signal
DMSO is a quirky solvent in mouse work — at high % it stresses hepatocytes and can shift purine flux; ethanol metabolism (acetaldehyde → NADH ↑) pushes the purine salvage/degradation equilibrium. Tracking liver XDH mass + serum UA + ALT across vehicle vs. solvent-control groups is the 10-second sanity check that prevents "the drug did something" from secretly being "the solvent spiked purine catabolism."
- Tumor Metabolism & the Purine Catabolism–ROS Feedback (Emerging, Not Core Textbook Yet)
Some aggressive tumors upregulate XOR as part of a purine-scavenging + ROS-signaling loop (local ROS from XO-mode acts as a pro-angiogenic/EDHF-modulating signal at the tumor–stromal interface). Measuring tumor-lysate XDH (ng/mg) alongside HIF-1α, VEGF, and 8-OHdG frames the "ROS = bad" dogma more precisely: sometimes the tumor keeps an XOR pool deliberately.
- Genetic Models: Xdh⁺/⁻ Heterozygotes, Pdha Interactions, and Mitochondrial–Cytosol Redox Coupling
Editing Xdh is embryonically lethal (purine salvage collapses), so mouse work uses heterozygotes, AAV-knockdown, or chemical modifiers (allopurinol/febuxostat/tungsten pretreatment). Report % XDH protein remaining ± SEM from the calibrated curve (ng/mg), and — this is the key — pair it with AMP/ATP ratio (luciferin-luminescence or LC-MS) and IMP/Hx/Xa/UA so the purine economy is closed, not just "an enzyme moved."
- Endothelial / Lung I/R & ARDS Models
Endothelial XOR is a major O₂⁻ source during reperfusion (pulmonary artery clamp, lung transplant preservation, CPB models). Measuring XDH in lung homogenates (ng/mg) plus BAL protein/PMN count + wet/dry ratio gives you the enzymatic hinge between "clamp released" and "edema formed."
A Minimal Workflow You Can Paste Into Methods
- Tissue: homogenize cold in 50 mM Tris pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100 + protease inhibitors, keep on ice, spin 12,000–16,000 ×g, 15 min, 4°C → supernatant → BCA → ng XDH / mg total protein.
- Serum/plasma: EDTA, cold chain, spin promptly, aliquot, -80°C, single thaw.
- Warm reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate.
The Bottom Line
XDH/XOR is the ~290 kDa homodimeric molybdoprotein (Mo-cofactor + FAD + [2Fe-2S]₂) that runs the last two steps of purine catabolism — hypoxanthine → xanthine → uric acid — and whose reversible sulfhydryl oxidation / proteolytic hinge cleavage converts it from an NAD⁺-sparing dehydrogenase into a ROS-leaking xanthine oxidase (XO) that drives the superoxide surge of reperfusion injury, hyperuricemia-associated endothelial stress, and crystal–inflammatory amplifications. Measuring it as a calibrated sandwich-ELISA variable instead of inferring it from a UA colorimetric kit changes your mouse paper from associative to causative. The Mouse Xanthine dehydrogenase/oxidase (XDH) ELISA Kit — KTE70003 from Abbkine gives you that variable: pre-coated anti-XDH capture → biotin detection → HRP–TMB → 450 nm → ng/mL, over a 0.156–10 ng/mL working range with LOD ~0.078 ng/mL, in a ~3–5 hour workflow that scales across I/R timecourses, hyperuricemia panels, and drug-screens without chaining you to a gel.
Product Reference: KTE70003 – Mouse Xanthine dehydrogenase/oxidase (XDH) ELISA Kit
Learn more and order: https://www.abbkine.com/product/mouse-xanthine-dehydrogenase-oxidase-xdh-elisa-kit-kte70003/
(For Research Use Only; not for diagnostic procedures in humans.)





