




The 17-kDa "Th1 Signature" That's Actually a Macrophage Wake-Up Call: Why Your Mouse IFN-γ Readout Deserves a 16 pg/mL Floor — And How KTE7003 Puts the Gold-Standard Sandwich on Your Supernatant Plate
If there is one cytokine that has carried more immunology papers than any other — appearing in figure panels from Listeria infection to tumor-infiltrating-lymphocyte exhaustion to autoimmune colitis — it is IFN-γ (interferon gamma, gene symbol Ifng, UniProt: P01580, Gene ID: 15978). And yet, the irony is that most labs still treat it like a checkbox: "We did intracellular FACS for TNF-α/IFN-γ, got ~12% Th1, looks good." But IFN-γ isn't just a T-box transcription marker or a pie-chart slice of CD4 subsets — it's a 143-aa, ~14–17 kDa secreted glycoprotein (mature secreted form ~14.2 kDa non-glycosylated core, migrates ~15–17 kDa on reducing gel) that functions as the master switch of classical macrophage activation (M1 polarization), the antiviral/intracellular bacterial defense gate, and the disease-promoting driver of nearly every IFN-γ-signature autoimmune model on the shelf. The EliKine™ Mouse IFN-γ ELISA Kit (KTE7003) from Abbkine is the reagent that takes this cytokine off your flow-compensation tab and puts it on a quantitative, two-site sandwich ELISA curve — 31.25 to 2000 pg/mL, LOD 16 pg/mL — so your T-cell-restimulation, infection-timecourse, or checkpoint-blockade paper rests on a plate-read pg/mL number with < 8% CV, not a "we saw a few spots on the ELISPOT."
IFN-γ in One Paragraph: The Dimer That Tells Macrophages to Eat, Not Heal
Unlike its namesake type I interferons (IFN-α/β, which bind IFNAR and are the antiviral branch), IFN-γ is the sole type II interferon — and it does completely different jobs:
Property Detail
Gene Ifng (mouse Chr 10, human Chr 12q14.1 syntenic region)
Mature secreted protein 143 aa, 14.3 kDa core, glycosylated forms run ~15–17 kDa, functions as a non-covalent homodimer (30–34 kDa) in solution
Receptor IFN-γR1 (IFNGR1) + IFN-γR2 (IFNGR2) → Janus kinases (JAK1/JAK2) → STAT1 → IRF-1 → GAS promoters
Producer cells CD4⁺ Th1, CD8⁺ Tc1, NK cells (primary), NKT, γδ T, some innate cells
Effector axis ↑ MHC-I/II expression, ↑iNOS/NO (NOS2), ↑CIITA (MHC transcription), ↑IRF-1, ↑CXCL9/10/11 (CXCR3 ligands), ↑autophagolysosomal pathogen-killing — collectively called classical / M1 activation
Shadow side Chronic IFN-γ → macrophage hyperactivation → tissue granuloma (TB, sarcoidosis models), DC over-maturation → T-cell exhaustion, or — when unchecked — autoimmune β-cell destruction (T1D models), EAE/neuromyelitis, and colitis
The number everyone writing a Methods section should respect: mouse IFN-γ in naïve/resting supernatants is often < 50–100 pg/mL, and only spikes into the 500–2000+ pg/mL range after TCR re-stimulation (anti-CD3/anti-CD28, PMA/ionomycin, peptide-pulsed APC) or acute infection (LCMV, Listeria, M. tuberculosis). That's exactly why your assay needs a 16 pg/mL LOD — to see the whisper before the spike.
Why a Sandwich ELISA — And Why "ELISPOT Counts" and "Flow %" Are Not Enough
Three practical reasons IFN-γ lives or dies by its secreted, soluble mass:
- Intracellular FACS / ELISPOT tells you which cell made it, but not how much accumulated in the environment — and in any supernatants-or-early-serum context (ex vivo bleed, microculture), the concentration that bathes neighboring cells is what drives paracrine polarization (especially M1 macrophage programming). You need the pg/mL, not just the spot count.
- IFN-γ is stable at 4°C and even -20°C for months (unlike, say, active TGF-β or labile peptides), which means it's one of the safest cytokines to run as a batched plate assay rather than a same-day-only flow chase.
- The sandwich format requires two murine-IFN-γ-specific epitopes — and because mature IFN-γ is ~143 aa with defined structural loops, a well-selected capture (pre-coated) + biotinylated detection (different face) gives you true two-site quantitation, not a polyclonal "something stuck" assumption.
The KTE7003 architecture is the canonical two-site build documented across Abbkine/Clinisciences/chem17 listings:
- Microplate pre-coated with a mouse IFN-γ-specific capture antibody (pre-coated, no DIY coating buffer headaches).
- Standards (NIBSC-traceable mouse IFN-γ calibrator) + samples — cell culture supernatants, serum, plasma (EDTA/heparin), other biological fluids — added → IFN-γ binds.
- Wash → biotinylated anti-mouse IFN-γ detection antibody (different epitope) → EliKine™ Streptavidin–HRP → TMB → color ∝ bound IFN-γ.
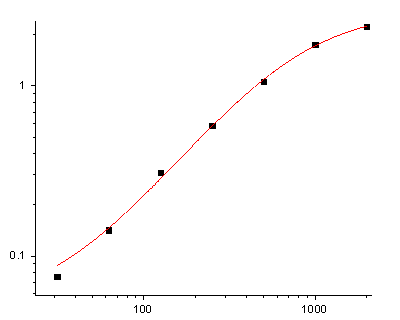
- Stop → 450 nm → interpolate pg/mL from a four-parameter logistic (4-PL) fit of the 8-point standard curve (31.25–2000 pg/mL).
Parameter KTE7003 – EliKine™ Specification
Target Mouse IFN-γ / IFNG (UniProt P01580, Gene 15978)
Format Sandwich ELISA, pre-coated capture (夹心法/双抗体夹心)
Detection Biotin-Ab → EliKine™ Streptavidin–HRP → TMB, 450 nm
Dynamic Range 31.25 – 2000 pg/mL
Sensitivity / LOD 16 pg/mL
Intra-Assay CV < 8%
Inter-Assay CV < 10%
Specificity No significant cross-reactivity with mouse IL-4, TNF-α, IL-10, IL-2, IL-6, IFN-α/β at physiological levels
Samples Cell culture supernatants, serum, plasma (EDTA/heparin), other biological fluids
Assay time ~3–5 hours
Storage (unopened) 2–8°C, sealed plate strips at 4°C with desiccant
(Confirm exact standard traceability on your shipped Abbkine CoA/datasheet; many lots use an NIBSC-traceable reference.)
The Prep Rule That Keeps Your 16 pg/mL Real
IFN-γ is fairly robust, but the small-volume, low-pg reality means:
• Cell culture supernatants: collect serum-free or 1–2% FBS (FBS is IFN-γ free from most sources, but high-FBS backgrounds can subtly shift OD — keep it low). Centrifuge ≥ 10,000 ×g, 5–10 min, 4°C, take clear sup, store -80°C, avoid >1 freeze–thaw.
• Serum/plasma: EDTA preferred, cold chain, spin promptly, aliquot, -80°C, single thaw.
• Restimulation plates (splenocytes/MLN/IEL): 48–72 h harvest → spin → SUP → straight into kit buffer dilution (most protocols land 1:1–1:4 neat sup inside the 31–2000 pg/mL window; follow your lot's advised dilution).
Warm reagents ≥ 30 min RT before opening; protect TMB; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate — and — this is the quiet hero — mix thoroughly but gently at every addition (low-frequency orbital rocker or manual tap-every-10-min).
Where Mouse IFN-γ ELISA Actually Carries the Paper (Beyond "Th1 Was Higher")
- Infection Immunology: The Listeria/LCMV/Toxo Kinetic That Is the Reason IFN-γ Exists
This is the textbook birthplace. Day 3–5 post-L. monocytogenes iv → CFU in spleen/liver peaks → IFN-γ in serum ~500–2000 pg/mL → if you neutralize it (anti-IFN-γ mAb XMG1.2), mice die of uncontrolled bacterial spread; if you KO Ifngr1, same fate. Running KTE7003 on tail-bleed EDTA plasma (0 h, 24 h, 48 h, 72 h, day 5, day 7) gives you the systemic-amplification curve that links bacterial burden → immune response → outcome — not just "CFU went down."
- Checkpoint Blockade & Tumor Immunity: The TME Cytokine Budget
Anti-PD-1/anti-CTLA-4 dogma hinges on reviving exhausted CD8⁺ T cells that re-secrete IFN-γ into the tumor microenvironment — but the cynical reality is that many papers only show ICOS ↑, Tim-3 ↓, and a token IFN-γ intracellular dot plot. Adding tumor-lysate-conditioned media or tumor-excised interstitial fluid (pg/mL IFN-γ, ELISA) alongside CXCL9/10 (GAS-driven) and NOS2/iNOS ties the T-cell re-activation to the actual chemokine/activation gradient the macrophage/stromal cell sees. It's the difference between "T cell looked less tired" and "the tumor milieu was chemically rewritten."
- Autoimmunity & the IFN-γ / IL-17 Seesaw (EAE, T1D, Colitis)
In MOG₃₅₋₅₅ EAE, disease onset correlates tightly with splenocyte IFN-γ production upon MOG recall; during CD45.1→CD45.2 adoptive-transfer colitis (CD4⁺CD62L⁺ naive → Rag⁻¹⁻/⁻), the same recall supernatants tell you whether your Treg expansion or IL-10 delivery actually suppressed Th1 effector mass. The ELISA lets you run 15–20 conditions × 4 timepoints in one plate with CVs — impossible with intracellular FACS alone.
- Vaccine Adjuvant & T-Cell Memory Screens (The "Did the Peptide Prime?" Question)
Peptide emulsions, mRNA-LNPs, recombinant VSV, or VSV-G pseudotypes — the gold-standard proof of priming is: ex vivo splenocyte/MLN restimulation (10 µg/mL peptide, 48–72 h) → harvest → KTE7003 → IFN-γ pg/mL vs. naïve control. It's faster than ELISPOT counting (though the two are complementary), and the pg/mL value lets you rank adjuvants (MPLA vs. CpG vs. AddaVax vs. alum) quantitatively instead of "spots looked bigger."
- NK Cell & Innate Immunity Assays (The Pre-Adaptive Surge)
Day 1–2 of certain viral or poly(I:C) challenges, before adaptive T cells have clonally expanded, the NK → IFN-γ burst is the early defense signal. Purify or enrich NK (DX5⁺ MACS), plate 10⁴–10⁵/well with IL-2 ± IL-12/IL-18 priming, harvest 24 h → KTE7003 readout (pg/mL normalized to cell number) → innate-effector budget quantified.
- CRISPRi / Adoptive-Transfer Validation
If you're editing Tbx21 (T-bet), Stat1, Ifngr1, or Il12rb2 in CD4⁺/CD8⁺ cells: report % IFN-γ protein remaining ± SEM from the calibrated standard curve (pg/mL → normalized to cell input), and close with Chromium-51 release / in vivo Listeria clearance / T-bet IF so the edit's functional consequence is airtight.
A Minimal Protocol You Can Paste Into Materials & Methods
- Supernatants: harvest 48–72 h post-stimulation, spin ≥ 10,000 ×g, 5–10 min, 4°C, collect clear supernatant, store -80°C, avoid >1 freeze–thaw.
- Serum/plasma: EDTA tube, keep on wet ice, spin ≥ 2,000 ×g, 10 min, 4°C within 60 min, aliquot, snap -80°C.
- Dilute into kit assay buffer per manual (typically neat or 1:2–1:4 supernatant for stimulated cultures; serum/plasma similar).
- Warm all reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve on every plate; report as pg/mL IFN-γ.
The Bottom Line
IFN-γ is the 143-aa, ~14–17 kDa homodimeric type II interferon that is the signature effector of Th1/Tc1/NK immunity — driving classical macrophage activation, MHC/antigen-presentation machinery, and CXCR3-ligand chemokine recruitment — and whose chronic overproduction is the pathogenic engine of granulomatous inflammation, autoimmune demyelination, and colitis. Measuring it as a calibrated sandwich-ELISA variable instead of a spot-count or a flow-percentage makes your infection/tumor/autoimmunity paper mechanically honest: it tells you how much of the messenger actually accumulated in the environment. The EliKine™ Mouse IFN-γ ELISA Kit — KTE7003 from Abbkine gives you that messenger: pre-coated anti-IFN-γ capture → biotin detection → EliKine™ SA–HRP → TMB → 450 nm → pg/mL, over a 31.25–2000 pg/mL working range with LOD 16 pg/mL (Intra CV < 8%, Inter CV < 10%), in a ~3–5 hour workflow that scales from a 48-well T-cell restimulation to a 20-mouse timecourse without chaining you to a spot-counter.
Product Reference: KTE7003 – EliKine™ Mouse IFN-γ (IFN gamma) ELISA Kit
Learn more and order: https://www.abbkine.com/product/elikine-mouse-ifn-%ce%b3-elisa-kit-kte7003/
(For Research Use Only; not for diagnostic procedures in humans.)





