




Your NF-κB p65 Band Has a Smear Again—Here's Why Your Current Antibody Is Sabotaging the Translocation Story (And How ABM40111 Fixes It for WB, IHC-P, and IF)
Every signaling lab that works on innate immunity, cytokine responses, or tumor-promoting inflammation has experienced this particular flavor of frustration: you treat your HeLa or RAW 264.7 cells with TNF-α, you know p65 (RELA) is supposed to abandon its IκB tether in the cytoplasm and pile into the nucleus within 30 minutes, and yet the Western blot you run with your "bargain" anti-p65 antibody gives you a fat ~65 kDa smudge flanked by three mystery bands that make your "cytoplasmic vs. nuclear fraction" argument look… charitable at best. The embarrassing part isn't the experiment. It's that NF-κB p65 (RELA, UniProt Q04206, Gene ID 5970) is one of the most heavily characterized transcription factors in existence—if your antibody can't give you a single, clean, nuclear-translocation-proving band and a crisp IHC-P readout, the problem isn't your fractionation skill. It's the reagent.
Why p65 Is the Gateway Readout—and Why It Punishes Sloppy Antibodies
The NF-κB family governs everything reviewers care about right now: TLR/NOD signaling, TNF-α cytotoxicity vs. survival decisions, IL-1β priming, PD-L1 promoter regulation in TME, and the senescence-associated secretory phenotype (SASP). The canonical heterodimer everyone tracks is p50 (NFKB1) ↔ p65 (RELA), held inert in the cytoplasm by IκBs, released when IKK phosphorylates IκBα → proteasomal degradation → p65 nuclear import → κB-site-driven transcription.
The experimental problem is structural: p65 is ~60 kDa calculated / ~65 kDa observed, runs in a crowded cytoplasmic region, and its activation state = subcellular location, not just "more or less protein." That means your antibody needs to do three things simultaneously:
- Recognize native + denatured p65 specifically (no cross-reactivity with RELB, c-Rel, or non-specific nuclear phosphoproteins of similar mass)
- Give a single clean band at ~65 kDa across human, mouse, and rat
- Work in IHC-P on paraffin so you can prove where p65 lives in the actual tissue, not just the lysate
A polyclonal serum might bind p65. A good monoclonal proves it—because one epitope = one predictable band = one defensible figure.
Enter NFκB p65 Monoclonal Antibody — ABM40111 (Abbkine)
This is a mouse IgG₁ monoclonal (clone 9C4) raised against recombinant human p65/RELA protein, affinity-purified from mouse ascites by antigen-specific affinity chromatography—a meaningful distinction from crude serum or Na₂SO₄-precipitated "IgG fractions" that drag non-specific IgM and proteases into your blot.
Parameter ABM40111 Specification
Target NF-κB p65 / RELA (UniProt Q04206, Gene ID 5970)
Alias NFKB3 · Transcription factor p65 · Nuclear factor of kappa light polypeptide gene enhancer in B-cells 3
Clone / Isotype 9C4 · Mouse IgG₁ (κ) · Monoclonal
Immunogen Recombinant protein (specific epitope within p65/RELA)
Reactivity Human · Mouse · Rat (H/M/R cross-validated)
Applications & starter dilutions WB: 1:1,000–3,000 · IHC-P: 1:50–200 · IF/ICC: ~1:200 · IP: 1:200
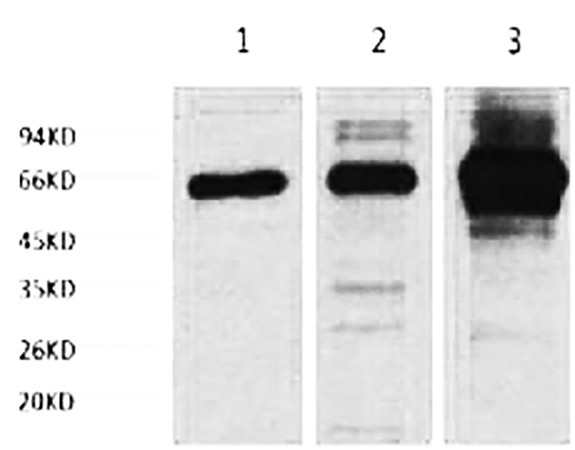
Observed MW ~65 kDa (calculated ~60 kDa; runs slightly high on SDS-PAGE)
Cellular localization Cytoplasm (inactive, IκB-bound) → Nucleus (upon TNF-α / LPS / cytokine induction)
Format / Conc. Liquid, 1 mg/mL in PBS pH 7.4 + 0.02% NaN₃ + 50% glycerol
Storage / Transport -20°C (1-year stable from ship date) · aliquot to avoid freeze–thaw · centrifuge before opening · ship blue-ice gel pack
Status For research use only; not for human/clinical diagnostic use
The real differentiator is the monoclonal epitope discipline. Where a polyclonal might give you a bright ~65 kDa band plus a fainter companion band that you'll spend two paragraphs apologizing for ("likely a post-translationally modified form or cross-reactive species"), ABM40111 is built to give you one decisive band at the right molecular weight across HeLa, rat heart, and mouse spleen — the exact validation trio Abbkine documents — and to carry that same specificity into IHC-P on human appendix FFPE and IF without the background snowstorm.
What Actually Changes in Your Figures When the Antibody Behaves
① Your cytoplasmic/nuclear fractionation finally looks like translocation.
p65 is the textbook case: IκB-bound in the cytosol → IKK releases it → nuclear accumulation within 15–60 min of TNF-α/LPS. With a 1:2,000–3,000 WB dilution that still gives you a strong, low-background ~65 kDa band, your GAPDH (cytosol) / Lamin B1 or HDAC1 (nucleus) normalization becomes visually undeniable — which is exactly what a reviewer scanning your Fig. 3 wants.
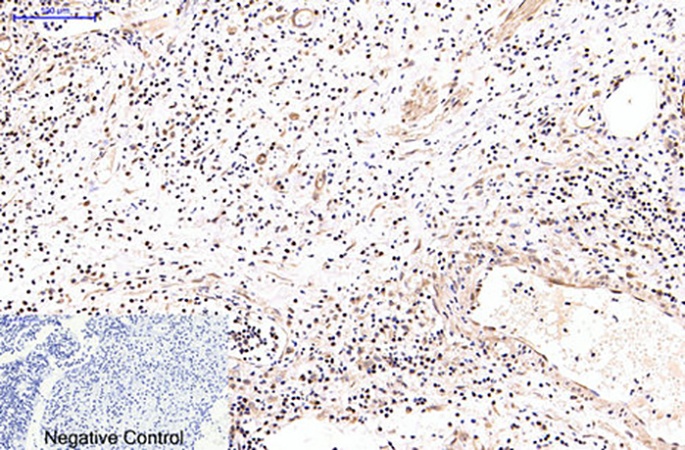
② Your IHC-P stops being a "brown-stain-everywhere" disappointment.
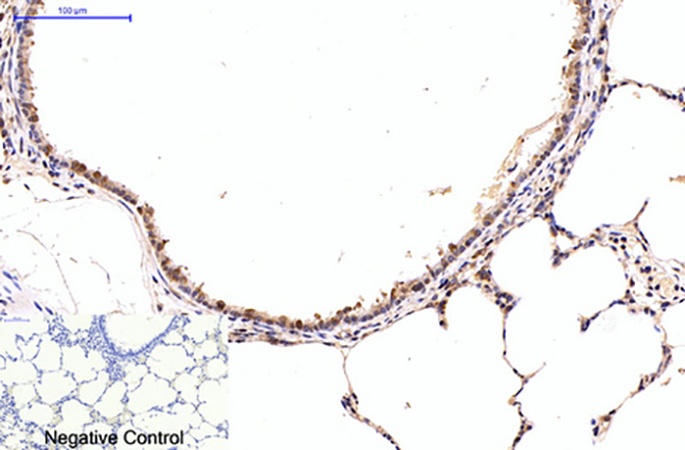
p65 IHC on FFPE (human appendix is the documented validation tissue) should read cytoplasmic-restricted in resting zones and nuclear-intense in TNF-rich inflammatory zones. A monoclonal that was purified for one p65 epitope preserves that contrast instead of lighting up stromal debris and giving you the "diffuse tan" look that screams non-specific.
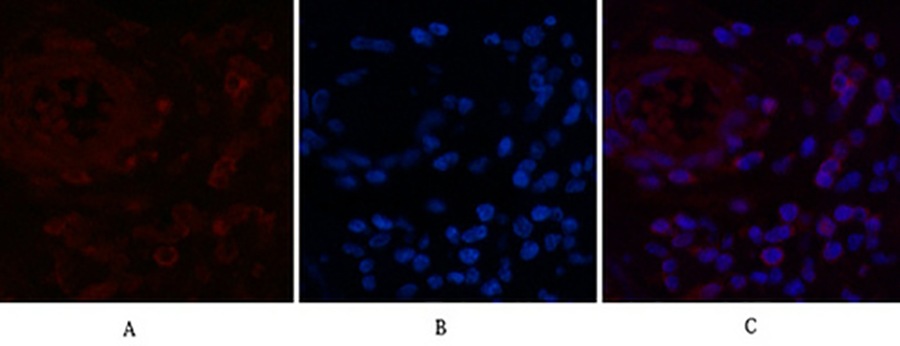
③ One antibody, four platforms, zero reinvention.
Because ABM40111 covers WB + IHC-P + IF + IP, your biochemical fractionation (WB), tissue cohort (IHC-P), cellular localization (IF), and DNA-binding-complex pull-down (IP/ChIP-adjacent) all ride the same clone. Your Methods section shrinks. Your batch-consistency problem disappears.
Bench Rules That Protect Your Signal (and Your Timeline)
• Centrifuge before opening. The stock is 1 mg/mL in 50% glycerol/PBS — dense. Brief spin-down recovers every µL from the cap/septum area.
• Aliquot on Day 1. The -20°C / glycerol format tolerates one accidental thaw, but repeat freeze–thaw is what degrades IgG₁ epitope accessibility. 5–10 µL aliquots save the stock and your experiment.
• Mind the NaN₃. 0.02% sodium azide in the storage buffer inhibits HRP — so if you're doing WB with an HRP-conjugate secondary, give the membrane 3–4 thorough TBST washes after blocking/primary incubation before the secondary step. It's basic, but it's the #1 reason someone says "my band is faint."
• For WB dilution scouting: start at 1:2,000 on a TNF-treated HeLa or RAW lysate. The documented validation goes up to 1:2,000 on HeLa with a clean ~65 kDa band — so your optimization range is narrow and confident.
• For IHC-P retrieval: standard citrate pH 6.0 or Tris-EDTA pH 9.0 protocols (your lab's existing epoch) generally work; the antibody has been validated on human appendix FFPE, so the epitope survives formalin fixation — just keep your retrieval time consistent across your cohort to avoid "patchy nucleus" artifacts.
Where ABM40111 Earns Its Line in Real, Published Work
Research Context Why p65/RELA (and This Clone) Is the Right Call
Innate immune signaling (TLR2/4, NOD2, TNF-α, IL-1β priming) Nuclear translocation is the readout; WB + IF with one monoclonal makes the translocation story airtight
Cancer signaling & TME (p65-driven PD-L1, survivin, cyclin D1, IL-6) IHC-P on cohort TMA → cytoplasmic vs. nuclear scoring; WB on xenograft lysates → clean ~65 kDa
Senescence / SASP (DNA damage → persistent NF-κB) p65 nuclear permanence distinguishes true SASP from transient inflammation; IP capability lets you check complex composition
Drug rescue screens (proteasome inhibitors, IKKβ blockers like ML120B, dexamethasone) Reversible p65 nuclear exclusion is the pharmacodynamic biomarker — needs a reproducible, dilution-tolerant primary
A Clean Methods Paragraph You Can Drop In
NF-κB p65 (RELA) protein was detected with a mouse monoclonal antibody (clone 9C4, ABM40111; Abbkine) at 1:2,000 dilution for Western blot (observed ~65 kDa, UniProt Q04206) and 1:100 for IHC-P on FFPE sections, following standard antigen retrieval (citrate, pH 6.0), per the manufacturer's recommendations. For cellular localization, IF was performed at 1:200. Membranes were washed thoroughly prior to HRP-secondary incubation to remove residual azide from the antibody storage buffer.
Explore the full specification sheet and ordering options for NFkB p65 Monoclonal Antibody (ABM40111) here:
🔗 https://www.abbkine.com/product/nfkb-p65-monoclonal-antibody-abm40111/
(For research use only. Not for human or clinical diagnostic use.)





