




Your IL-1β Data Looks "Almost Significant"—But Is It the Biology or Your ELISA? Here's Why KTE6013 Is the Fix Every Inflammasome Lab Needs
There's a special kind of frustration unique to cytokine work: you've run your LPS challenge, treated your THP-1s with nigericin, confirmed NLRP3 assembly by Western—and then your IL-1β ELISA gives you a scatterplot that looks more like modern art than publishable data. The usual suspects? A sandwich kit with drifting baseline, cross-reactivity that shouldn't exist, or a detection floor so high you can't tell whether your 10 pg/mL sample is real signal or just plate noise.
Here's the uncomfortable truth most "high-sensitivity" marketing copy won't tell you: IL-1β is one of the hardest cytokines to quantify cleanly because it circulates at extremely low basal levels (often <5 pg/mL in healthy human serum) and then spikes 100–1000× during an inflammasome flare. If your assay's detection floor is 10 pg/mL, you're blind to the basal state—and your fold-changes are built on sand.
Why IL-1β Demands More Than a Generic Sandwich ELISA
IL-1β (gene symbol IL1B; UniProt P01584; ~17 kDa pro-form, cleaved by caspase-1 to its active mature form) is the canonical effector of the NLRP3 inflammasome—the gateway cytokine driving pyroptosis, sterile inflammation, atherosclerosis, neurodegeneration (AD microglia activation), gout, and the cytokine release syndrome everyone's been obsessing over since 2020. It's also the readout that makes or breaks drug screening on NLRP3 inhibitors, PBMC donor variability studies, and macrophage polarization panels.
The problem with cut-rate or cross-purposed ELISA kits is that IL-1β's structural relatives—IL-1α (IL1A), IL-33, and other IL-1 superfamily members—share enough topology that a poorly selected capture/detection pair will quietly bleed signal. When reviewers see a Methods section that just says "IL-1β measured by ELISA," they're going to look hard at your supplementary figures. Your assay needs to be specific, sensitive below 5 pg/mL, and reproducible across plates.
Enter EliKine™ Human IL-1β ELISA Kit (KTE6013) — Purpose-Built, Not Repackaged
Abbkine's EliKine™ Human IL-1β ELISA Kit (KTE6013) is engineered around a true two-site sandwich architecture that closes the three loopholes that destroy cytokine data:
• Pre-Coated Microplate — 96-well strips coated with a human IL-1β–specific capture antibody, eliminating manual coating variability (the #1 source of plate-to-plate drift).
• Biotin-Conjugated Detection Antibody — binds a second, non-overlapping epitope on captured IL-1β, forming the sandwich.
• EliKine™ Streptavidin-HRP — delivers amplified, enzyme-linked signal.
• TMB Substrate → 450 nm read (620–650 nm optional reference) — standard, spectrophotometrically clean, and compatible with every plate reader in every core facility.
The performance envelope that actually matters on a Methods line:
Parameter KTE6013 Specification
Method Sandwich ELISA (double-antibody, two-site)
Reactivity Human (Homo sapiens, Gene ID 3553 / UniProt P01584)
Sample types Cell culture supernatants · Serum · Plasma (EDTA/heparin) · Other biological fluids
Sensitivity (LOD) 4 pg/mL
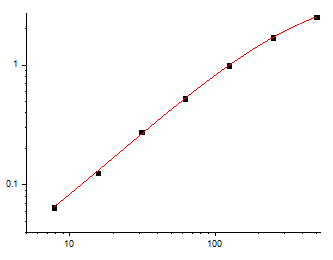
Dynamic range 7.8 – 500 pg/mL (5-parameter or linear regression per standard curve)
Specificity No significant cross-reactivity with IL-1α, IL-1ra, or related IL-1 superfamily ligands (validated)
Components included Pre-coated anti-IL-1β 96-well plate · IL-1β protein standard · Biotin-anti-IL-1β detection Ab · EliKine™ Streptavidin-HRP · Standard/sample diluents · Wash buffer · TMB substrate · Stop solution · Sealing films
Storage / Ship 2–8°C (unopened); ship blue-ice gel pack; research use only
What Changes in Your Lab When Your Floor Drops to 4 pg/mL
The difference between a "maybe" and a defensible figure comes down to three things this kit gets right:
- You stop discarding your most informative data points.
Basal IL-1β in unstimulated human PBMC supernatants or healthy donor serum routinely sits at 1–5 pg/mL. With a 4 pg/mL floor and a validated 7.8 pg/mL lower quant limit, you can actually measure the baseline instead of coding it as "<LOD" and praying your stats package handles left-censored data correctly. - Your NLRP3 inhibitor dose–response curves stop looking like noise.
When you're screening MCC950 analogues or screening CRISPR hits for inflammasome negative regulators, the dynamic range (7.8 → 500 pg/mL, ~64-fold span) captures both the unstimulated floor and the LPS+nigericin ceiling in a single standard curve—no split-dilution acrobatics required. - Multi-donor/clinical correlation studies become viable.
Because the plate is pre-coated and the standard is built-in, your inter-assay CV becomes something you can state with confidence in your Methods. That's the difference between a paper that clears review in one round and one that spends three months in revise-and-resubmit hell over "concerns regarding cytokine quantification methodology."
The Bench-Level Workflow (Fast, Predictable, Zero "Artisanal" Steps)
Step 1 — Thaw & Balance: Bring all components to room temperature (≥30 min) before opening. Keep unused strips in the original sealed pouch with desiccant at 2–8°C.
Step 2 — Load: Add Standards and Samples (typically undiluted or 1:2–1:10 depending on expected range) to duplicate wells. Incubate.
Step 3 — Detect: Wash → add Biotin-anti-IL-1β → wash → add Streptavidin-HRP → wash → add TMB (develop, protected from light) → stop with provided stop solution.
Step 4 — Read: 450 nm (reference 620–650 nm optional). Plot standard curve, interpolate unknowns, correct for dilution.
Non-negotiable housekeeping rules from the protocol notes:
• ⚠️ Never mix reagents across different lot numbers or expired kits. Your standard curve is lot-specific.
• ⚠️ Use fresh pipette tips for every transfer—cytokine carryover is silent and lethal to your data.
• ⚠️ Resuspend/reconstitute and mix thoroughly (low-frequency shaker or hand-tap every ~10 min during incubations).
• ⚠️ Seal unused wells immediately; return to 2–8°C in the resealed foil bag.
Where KTE6013 Earns Its Spot in the -20°C Box
Research Context Why IL-1β (and This Kit) Is the Right Call
NLRP3 inflammasome drug discovery Primary readout for caspase-1–dependent secretion; 4 pg/mL sensitivity catches partial inhibition others miss
Macrophage / microglia polarization Distinguishes M1 (IL-1β-high) from M2 states in conditioned media without burning 500 µL/well
Sepsis / systemic inflammation biomarker panels Works on human serum & plasma; plays nicely in multi-cytokine pipelines (run TNF-α, IL-6, then IL-1β on parallel pre-coated formats)
PBMC donor-variability / clinical cohort pilots Pre-coated format = low CV across plates; you can actually compare Donor 1 (Monday) with Donor 12 (Thursday)
The bottom line is blunt: IL-1β isn't a "bonus figure" you tack onto a macrophage paper—it's often the mechanistic hinge your entire argument rests on. If you're going to hang a story on NLRP3 activation, pyroptosis, or sterile inflammatory signaling, your quantification needs to survive a methods-savvy reviewer. The EliKine™ Human IL-1β ELISA Kit (KTE6013) is built exactly for that standard—sandwich-specific, 4 pg/mL-sensitive, pre-coated, and formatted for the 96-well reality every real lab actually lives in.
Explore the EliKine™ Human IL-1β ELISA Kit (KTE6013) here:
🔗 https://www.abbkine.com/product/elikine-human-il-1%ce%b2-elisa-kit-kte6013/
(For research use only. Not for human or clinical diagnostic use.)





