




Stop Letting “Noisy IL-6” Kill Your Paper’s Impact: Why Abbkine’s EliKine™ Human IL-6 ELISA Kit (KTE6017) Is the Sandwich Assay Your Inflammasome & Sepsis Panels Deserve
If you’ve ever watched a reviewer tear into a cytokine panel because the IL-6 scatterplot looks like shotgun spray, you already know the dirty secret of the field: IL-6 is easy to detect and annoying to quantify well. It’s a central hub for infection, trauma, autoimmune flare, NLRP3-driven pyroptosis, CAR-T cytokine release, and even tumor-promoting inflammation—yet the difference between a crisp, defensible dose–response and a “borderline significant” disaster usually comes down to one boring thing nobody puts on a poster: assay architecture + plate consistency.
Too many labs learn the hard way that “we ran an IL-6 ELISA” isn’t a method—it’s a gamble—when the kit relies on hand-coated plates, loosely defined buffers, and “good enough” wash steps. The result? Baseline drift, inflated CVs, and that painful revise-and-resubmit loop where you’re asked to prove your 4–8 pg/mL numbers aren’t just plate noise.
Why IL-6 keeps humbling otherwise excellent experiments
IL-6 (UniProt P05231, gene IL6 / ID 3569) is famously pleiotropic: B-cell stimulatory factor-2 activity, CTL differentiation support, acute-phase inducer, fever mediator, and a core readout for danger-associated signaling. That importance is exactly why your quantification bar is higher.
The problems that actually sink datasets are rarely conceptual—they’re operational:
• Surface inconsistency: Manual coating or uneven plate storage creates well-to-well binding differences you can’t normalize away.
• Wash sensitivity: IL-6 is often measured at low pg/mL in basal or clinical-baseline samples; sloppy aspiration/over-drying ruins the floor.
• Lot cross-contamination: Using reagents from different batches (or “topping up” with someone else’s bottle) injects a low-level systematic error that looks random to statistics but isn’t.
• Timing & mixing: Sandwich ELISAs reward boring discipline—consistent incubations, thorough but gentle resuspension, and no “quick vortex-and-pray” steps.
In short, your IL-6 readout is often less about IL-6 biology and more about whether your reagents behave the same way on Monday and Thursday.
Enter EliKine™ Human IL-6 ELISA Kit (KTE6017) — purpose-built sandwich, not repackaged generic
Abbkine’s EliKine™ Human IL-6 ELISA Kit (Cat# KTE6017) is a quantitative two-site sandwich ELISA designed to take the variability out of the parts you shouldn’t be improvising:
• A pre-coated 96-well microplate with a human IL-6–specific capture antibody, so plate-to-plate binding variance is dramatically reduced compared to do-it-yourself coating.
• A biotinylated anti-IL-6 detection antibody (binding a second epitope) → EliKine™ Streptavidin-HRP amplification → TMB substrate → stop solution → 450 nm read (620–650 nm reference optional).
• Supplied IL-6 standard so you’re interpolating unknowns from a kit-calibrated curve, not leaning on heroic assumptions.
Key performance envelope you’ll want in your Methods line :
Parameter KTE6017 (as specified by the product listing)
Assay type Quantitative sandwich ELISA (two-site)
Reactivity Human (IL6; UniProt P05231)
Sample types Cell culture supernatants · serum · plasma · other biological fluids
Sensitivity (LOD) ~2 pg/mL
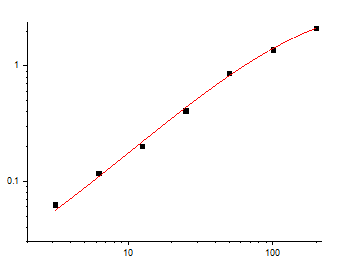
Typical calibration range ~3.125 – 200 pg/mL (standard-dependent; follow your kit’s current sheet)
Detection Colorimetric TMB → stop → 450 nm
Storage (unopened) 2–8°C; ship blue-ice; Research use only
Core components Pre-coated plate · IL-6 standard · biotin-anti-IL-6 detection Ab · EliKine™ Streptavidin-HRP · diluents/buffers · TMB · stop soln · wash buffer · seals
Where KTE6017 earns its keep (the experiments people actually reject)
If your story touches any of the following, IL-6 isn’t a “bonus panel item”—it’s the hinge between mechanism and phenotype:
• Infectious / systemic inflammation models (LPS, polymicrobial sepsis, cytokine storm readouts) where you must distinguish true low-basal from assay floor noise.
• NLRP3 / inflammasome work (LPS ± nigericin, MSU crystals, etc.): IL-6 pairs with IL-1β, but it’s often easier to kill with a bad wash than IL-1β because you’re chasing a broader dynamic spread.
• Immuno-oncology & cell therapy QC: conditioning regimens, checkpoint combos, and CAR-T / TIL release assays where reproducible pg/mL-level resolution is what lets you claim safety margins.
• Metaflammation / metabolic-disease models: diet-induced obesity, steatohepatitis, adipokine cross-talk—where IL-6 trends are real but small unless the assay is tight.
The advantage of the pre-coated, lot-controlled sandwich format is simple: your CV becomes a function of biology + pipetting, not “who coated the plate and whether the TMB sat too long last Tuesday.”
Bench-level rules that keep KTE6017 bulletproof (and your supplementals reviewer-proof)
• Balance temp before you start: Bring all components to room temperature (≥30 min) before opening the sealed plate pouch; immediately reseal unused strips with the desiccant returned to 2–8°C.
• Never mix lot numbers, and don’t “borrow” wash buffer or streptavidin-HRP from another kit/batch—this is the single most common source of mysterious plate drift.
• Treat washes like a protocol, not a vibe: consistent aspirate, no over-drying of wells, recommended wash volumes/cycles per the manual.
• Replicates are cheap insurance: run duplicates or triplicates for standards and samples; it’s the easiest way to spot a bubble or a tip-click error before it becomes a rejected figure.
• Mix gently but thoroughly: low-speed oscillation or a careful tap every ~10 min during incubations is often recommended for even binding—never “vigorous vortex the plate.”
TL;DR for your Methods paragraph
Human IL-6 was quantified using a quantitative sandwich ELISA (EliKine™ Human IL-6 ELISA Kit, KTE6017; Abbkine), according to the manufacturer’s protocol. A pre-coated anti-IL-6 capture antibody microplate was used; after sample/standard incubation and washing, a biotinylated anti-IL-6 detection antibody followed by Streptavidin-HRP was applied, developed with TMB, stopped, and read at 450 nm (reference 620–650 nm). Values were interpolated from the supplied IL-6 standard curve.
Explore the EliKine™ Human IL-6 ELISA Kit (KTE6017) here:
https://www.abbkine.com/product/elikine-human-il-6-elisa-kit-kte6017/
(For research use only; not for human clinical diagnostic use.)





