




Your Breast Cancer & Reproductive Biology Figures Live or Die by the Nuclear Transcription Factor You're Treating Like a "Generic Loads-Control" — Here's Why ABP0086 Is the ERα Polyclonal That Stops Embarrassing You at the Reviewer Stage
If you've ever had that stomach-drop moment when Reviewer #2 notes "The authors should validate the specificity of the ERα antibody used, particularly given the widespread issues with cross-reactivity among nuclear hormone receptors," you already know: Estrogen Receptor α (ESR1, UniProt P03372) is not a "nice-to-have" band at ~66 kDa — it's the gatekeeper of every estrogen-driven phenotype you're claiming. Whether you work on MCF-7/LCC1 endocrine resistance, endometrial hyperplasia, or the bone-sparing effects of SERMs, your entire mechanism collapses if your anti-ERα reagent is lighting up ERβ (ESR2), PR (PGR), or just random nuclear proteins that happen to run near 60–66 kDa. The dirty truth? Most labs grab whatever "anti-ERα" is in the -20°C box, run it at 1:200, get a smear, and call it a day. And then the revision letter arrives.
ERα Isn't Just "A Hormone Receptor" — It's a Ligand-Activated Transcription Factor That Demands Epitope Discipline
ESR1 encodes the classic nuclear estrogen receptor α, a modular ligand-activated transcription factor composed of an N-terminal AF-1 domain, a highly conserved DNA-binding domain (DBD, C domain), a hinge region (D), and the C-terminal LBD/activation-function-2 (AF-2, E domain) that binds estradiol (E2) and selective modulators (SERMs/SARMs). It localizes to the nucleus — functioning as a homodimer (or heterodimeric partner with ERβ) — and drives expression of progesterone receptor (PGR), cyclin D1 (CCND1), cathepsin D, pS2/TFF1, and a dozen other proliferation/apoptosis/metabolic genes.
The flip side is clinical: ~70% of breast cancers are ERα-positive at diagnosis, and ESR1 missense mutations (most famously Y537S and D538G in the LBD) are the dominant driver of acquired aromatase-inhibitor and tamoxifen resistance. So when you probe ERα levels across your tamoxifen-sensitive vs. resistant clones, or your E2-dose-response in ovariectomized mouse uterus, your antibody isn't decorative. It's the analytical foundation of your entire endocrine story.
The Detection Problem: ERα Shares ~60% DBD Identity with ERβ — and Most Polyclonals Can't Tell Them Apart Cleanly
Here's what burns people: the DNA-binding domain of steroid/nuclear receptors is the most conserved region, so any polyclonal raised against "whole ERα protein" or a DBD-heavy fragment will happily cross-react with ERβ (ESR2), glucocorticoid receptor fragments, or unrelated nuclear DNA-binding proteins. What you need is an immunogen that targets unique, non-overlapping sequence — ideally in the LBD/AF-2 (E-domain) or a C-terminal region where ERα diverges from ERβ by ~30–40%.
That's exactly what ABP0086 (ERα Polyclonal Antibody, Abbkine) is built around:
Parameter ABP0086 Specification
Target ERα / Estrogen Receptor α / ESR1 (UniProt P03372, Gene ID 2099)
Aliases ESR1 · ESR · NR3A1 · Estradiol receptor · Estrogen receptor 1 · ER-alpha
Host / Isotype Rabbit · IgG · Polyclonal
Immunogen Synthetic peptide derived from human ERα (sequence-unique region, not the conserved DBD)
Reactivity Human, Mouse, Rat (H/M/R cross-validated)
Subcellular locale Nucleus (ligand-activated transcription factor)
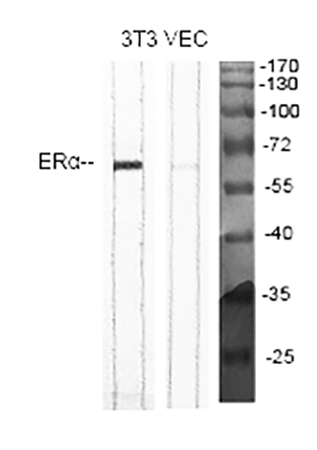
Observed MW ~66 kDa (the classic, full-length ERα band)
Validated Apps & Starting Dilutions WB: 1:500–2,000 · IHC-P: 1:100–300 · ELISA: ~1:20,000
Format / Conc. Liquid, 1 mg/mL in PBS pH 7.4 + 1% BSA (or carrier protein), 0.02% NaN₃ + 50% glycerol
Storage / Ship -20°C (1-year stable from ship date); centrifuge before opening; aliquot to avoid freeze–thaw; ships blue-ice gel pack
Status For research use only; not for human/clinical diagnostic use
The differentiator is the same word that keeps appearing across every antibody we've covered: epitope specificity born from a synthetic-peptide immunogen strategy, not "inject a GST-fusion and hope the bleed-serum likes the right face." The result is an ERα band at ~66 kDa that actually belongs to ESR1, not a nuclear neighbor.
What Actually Changes in Your Paper When ERα Behaves Instead of "Showing Up"
① Your endocrine-resistance Western stops needing three paragraphs of apology.
Run ABP0086 at 1:1,000–2,000 on MCF-7 (positive) vs. an ERα-knockdown/siESR1 or ER-negative line (MDA-MB-231, BT-20) as your negative control, and the ~66 kDa band speaks for itself. That positive/negative pair — documented once, shown in a supplementary lane — is exactly what shuts down the "how was specificity validated?" critique.
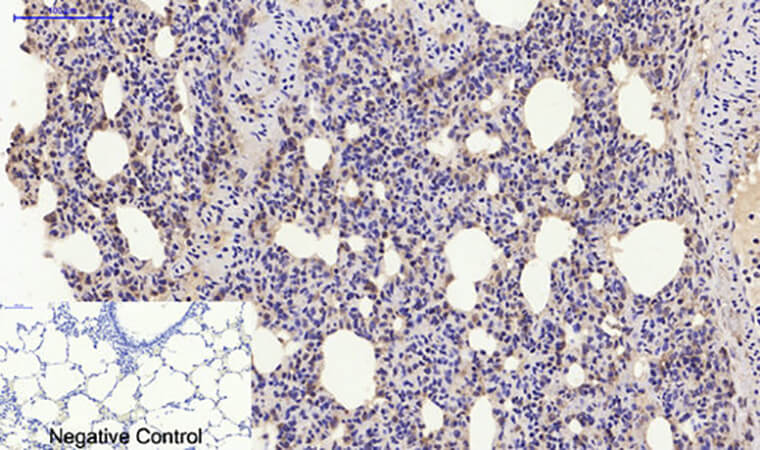
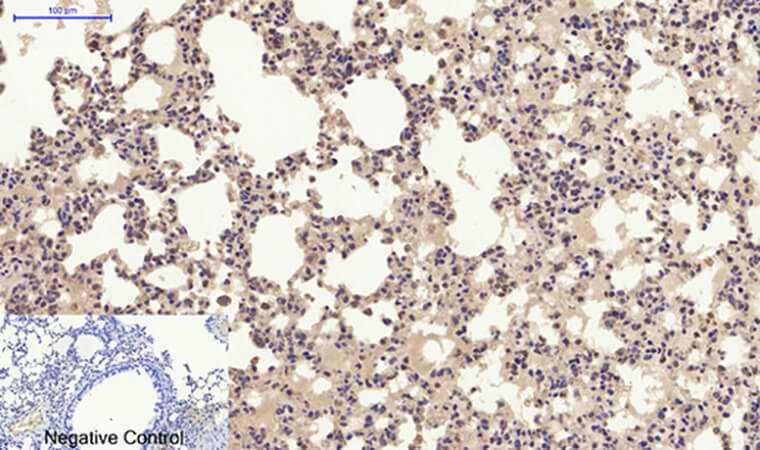
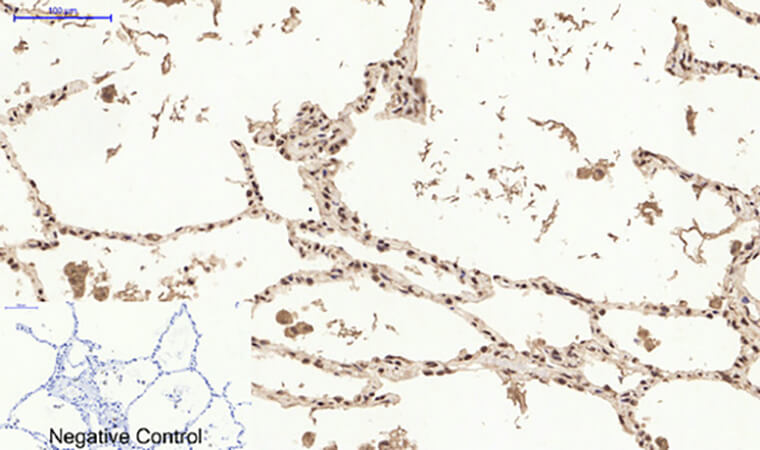
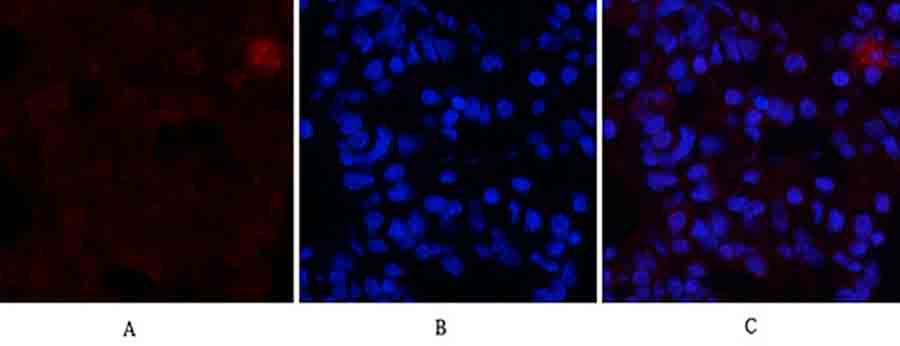
② Your IHC-P on FFPE patient cores / xenograft sections becomes publication-grade, not "brown nuclei everywhere."
Hormone-receptor IHC is notorious for non-specific nuclear staining when the antibody isn't affinity-purified or epitope-controlled. ABP0086 at 1:100–300 with standard citrate pH 6.0 retrieval gives you nuclear-restricted, ligand-responsive intensity gradients — the kind that make a TMA scoring session actually meaningful instead of "everything is 2+."
③ One vial, three platforms, zero reinvention.
Because it covers WB + IHC-P + ELISA, your cell-lysate screen → xenograft validation → FFPE-cohort scoring all ride the same rabbit polyclonal clone/epitope, keeping your Methods tight and your batch-consistency headache-free.
The Bench Rules That Protect Your ~66 kDa Band (and Your Friday Night)
ERα is a nuclear, DNA-binding, ligand-sensitive TF — and your prep respects it or pays for it:
• Centrifuge before opening. The stock is 1 mg/mL in 50% glycerol/PBS — dense. Brief spin-down recovers every µL from the cap/septum area.
• Aliquot on Day 1 into 5–10 µL tubes. The -20°C/glycerol format tolerates storage beautifully, but repeat freeze–thaw is what degrades IgG epitope accessibility and raises your background along the lane.
• Mind the NaN₃. 0.02% azide inhibits HRP — so after your primary incubation on the membrane, give it 3–4 thorough TBST washes before adding that HRP-conjugated anti-rabbit secondary. Basic, but it's the #1 reason someone says "my ERα band is faint."
• WB dilution scouting: start 1:1,000 on MCF-7 lysate (~20–30 µg total protein). Strong signal at 1:2,000 with clean nuclear-only background is the sweet spot. Run a negative control lane (MDA-MB-231 or siESR1) once to document.
• For IHC-P: standard citrate pH 6.0 microwave/steamer retrieval, peroxidase block (3% H₂O₂), and your lab's normal-serum block → 1:200 overnight at 4°C → HRP-secondary → DAB → hematoxylin counter. Document the retrieval time and keep it identical across your TMA/cohort so your intensity scores mean something.
• For ELISA coating/capture validation (1:20,000 starting dilution noted), keep in mind this is a polyclonal — if you're building a sandwich, you'd typically need a second, non-overlapping monoclonal for detection; for direct coating/blocking validation it works cleanly.
Where ABP0086 Earns Its Line in Real, Cited Work
Research Context Why ERα (ABP0086) Is the Pillar, Not an Afterthought
ER+ breast cancer / endocrine resistance (TAM → AI → ESR1-mut load) Clean ~66 kDa band + nuclear IHC = the diagnostic pairing pathology reports hinge on
Reproductive biology & bone (E2, SERMs/SARMs, osteoblast/osteoclast coupling) Nuclear ERα in osteoblasts & hypothalamus mediates non-reproductive E2 actions; specific detection avoids ERβ bleed
Endometrial hyperplasia / gynecologic pathology (E2-driver, unchecked proliferation) FFPE IHC scoring of ERα intensity/distribution = standard-of-care biomarker context
Xenograft & PDX models (tumor response to fulvestrant/Faslodex) Downstream PR (PGR) and CCND1 only make sense if your ERα readout is specific
Environmental endocrine disruptor screens (BPA, genistein, alkylphenol) Low-dose EDC effects are subtle — you need a 1:2,000 WB band with low bg to see a 15–20% shift
A Clean Methods Paragraph You Can Drop Straight In
Estrogen Receptor α (ERα/ESR1) was detected with a rabbit polyclonal anti-ERα (ABP0086; Abbkine), immunogen: synthetic peptide derived from human ERα, at 1:1,000–2,000 for Western blot (observed ~66 kDa, UniProt P03372) and 1:200 for IHC-P on FFPE sections following citrate pH 6.0 antigen retrieval, per the manufacturer's recommendations. Membranes were washed thoroughly prior to HRP-secondary incubation to remove residual azide from the antibody storage buffer. Specificity was confirmed using ERα-negative controls (e.g., MDA-MB-231 or ESR1-knockdown lysate) as appropriate.
Explore the ERα Polyclonal Antibody (ABP0086) full specs, datasheet & ordering options here:
🔗 https://www.abbkine.com/product/erα-polyclonal-antibody-abp0086/
(For research use only. Not for human or clinical diagnostic use. Centrifuge before opening; aliquot to avoid freeze–thaw; 0.02% NaN₃ present — rinse membranes thoroughly before HRP-secondary.)





