




The Smallest Protein in the Largest Enzyme Complex—and the ELISA Kit That Finally Quantifies It
If you were to rank every protein in the human mitochondrial respiratory chain by molecular weight, one would sit alone at the bottom of the list, weighing just 6.4 kDa and comprising a mere 56 amino acids. That protein is cytochrome b-c1 complex subunit 10 (UQCR, also designated UQCR11 or QCR10), and it is not a vestigial peptide clinging to Complex III by evolutionary accident. It is the smallest known component of the ubiquinol-cytochrome c reductase complex—the 11-subunit, 1.1-megadalton oxidoreductase that occupies the middle position in the mitochondrial electron transport chain—and its functional assignment, established through decades of biochemical and genetic work, is to act as a binding factor that stabilizes the association of the Rieske iron-sulfur protein (UQCRFS1) with the core of the complex. When UQCR is absent or dysfunctional, the iron-sulfur protein dissociates, electron transfer from ubiquinol to cytochrome c stalls, the Q cycle collapses, and the entire respiratory chain upstream of Complex IV backs up with electrons that escape as superoxide. A protein weighing less than a tenth of an IgG light chain thus determines whether the inner mitochondrial membrane generates ATP or leaks radicals.
The biomedical significance of UQCR has expanded dramatically in the past five years, and the expansion has caught many metabolism laboratories without the quantitative tools to participate. A 2024 study published in Nature Communications demonstrated that the RNA acetyltransferase Nat10 suppresses Uqcr11 and Uqcrb expression independently of its ac4C catalytic activity, weakening mitochondrial respiration and enhancing glycolytic capacity in cardiomyocytes—a metabolic reprogramming event that directly reduces cardiac contractility and contributes to heart failure pathogenesis. The same year, an independent group identified a homozygous UQCR11 mutation as a novel cause of severe hypertrophic cardiomyopathy, with patient-derived data and UQCR11-deficient HeLa cells both showing lower basal and maximal oxygen consumption, pinpointing dysfunctional mitochondria when cells are forced to rely on oxidative phosphorylation. In oncology, quantitative proteomics identified UQCRQ—the subunit adjacent to UQCR in the Complex III low-molecular-weight subassembly—as one of three oxidative phosphorylation genes with clinical prognostic significance in gastric cancer, with higher expression positively correlated with better prognosis and implicating these proteins as novel candidate diagnostic and prognostic biomarkers. The Human Protein Atlas catalogues UQCR expression across cancer types, noting that most cancers display weak to moderate cytoplasmic positivity, while a subset of skin cancers, hepatocellular carcinomas, cervical, colorectal, and urothelial cancers are strongly stained. Irregular UQCR10 and UQCRQ expression may affect the assembly of the core subunit of Complex III, increase the risk of transient semiquinone leakage generated during the redox-dependent reaction, and ultimately enhance oxidative stress.
These discoveries share an analytical prerequisite that most of the laboratories pursuing them have not been equipped to satisfy: the ability to quantify UQCR protein concentration directly and specifically in biological samples. Northern blot analysis of human tissues has detected a UQCR transcript at high levels in energy-requiring tissues such as heart and skeletal muscle—tissue types that are among the most difficult to process for quantitative protein biochemistry because of their dense contractile apparatus, abundant endogenous peroxidases, and high mitochondrial content. Western blotting can confirm UQCR presence but generates semi-quantitative data that reviewers evaluating a study on mitochondrial complex stoichiometry or a drug mechanism manuscript will not accept as dose-response evidence. Mass spectrometry provides sequence-level identification but requires a dedicated proteomics core, isotopically labeled internal standards, and per-sample costs that rapidly become prohibitive across the sample numbers that clinical cohort studies demand. The gap between the biological importance of UQCR and the availability of a reliable, specific, and accessible quantitative tool has been, until now, a gap in the measurement rather than a gap in the biology.
Abbkine's Human Cytochrome b-c1 Complex Subunit 10 (UQCR) ELISA Kit (KTE60084) addresses that measurement gap at the level of antibody engineering. The kit employs a two-site sandwich ELISA architecture in which a capture antibody specific for human UQCR has been pre-coated onto a microplate. Standards and samples are pipetted into the wells, and any UQCR present is bound by the immobilized antibody. After removing unbound substances, a biotin-conjugated detection antibody specific for UQCR is added, followed by streptavidin-conjugated horseradish peroxidase. Following a wash to remove any unbound enzyme conjugate, a substrate solution develops color in direct proportion to the amount of UQCR bound in the initial step. The color development is stopped, and the absorbance intensity provides a quantitative readout of UQCR concentration in each well. The assay runs for 3–5 hours depending on operator experience, positioning it as a same-day experiment that fits comfortably within a standard laboratory workday.
The specificity specification is the dimension that most directly determines data quality in a mitochondrial protein ELISA. The product page states that no significant cross-reactivity or interference between Human UQCR and analogues was observed. This matters because Complex III is a multimeric enzyme composed of 11 subunits—cytochrome b, cytochrome c1, Rieske protein UQCRFS1, core proteins UQCRC1 and UQCRC2, and six low-molecular-weight subunits including UQCRH, UQCRB, UQCRQ, UQCR10, and the cleavage product of Rieske protein—many of which share structural motifs, co-migrate in immunoprecipitation experiments, and are co-regulated at the transcriptional level. An ELISA that cross-reacts with UQCRQ or UQCR10 is measuring a pooled low-molecular-weight subunit concentration rather than UQCR specifically, and a study that builds its conclusions on that pooled measurement is describing complex III subunit abundance in aggregate rather than UQCR concentration in particular. The dual-site sandwich architecture of KTE60084 ensures that both the capture and detection antibodies must engage the target for signal to develop, providing specificity that single-antibody detection formats cannot achieve.
Sample compatibility spans the biological matrices in which UQCR is biologically and clinically relevant: serum, plasma, cell culture supernatants, and other biological fluids. The inclusion of cell culture supernatants is particularly significant because mitochondrial proteins are not typically secreted—yet UQCR and other Complex III subunits can appear in the extracellular compartment following mitochondrial damage, mitophagy, or cell death, and their presence in conditioned medium or circulating biofluids has been proposed as a biomarker of mitochondrial stress. The inclusion of "other biological fluids" accommodates specialized sample types such as bronchoalveolar lavage fluid, cerebrospinal fluid, or tissue interstitial fluid, enabling multi-compartment UQCR profiling within a single standardized ELISA workflow.
The kit components ship as a complete sandwich ELISA package: Human UQCR microplate, Human UQCR standard, Human UQCR detect antibody, Streptavidin-HRP, standard diluent, assay buffer, HRP substrate, stop solution, wash buffer, and plate covers. The calibration range and limit of detection are specified as "please inquire," which is standard for a recently launched kit targeting a mitochondrial protein whose endogenous concentrations vary across tissue types and whose reference ranges in serum and plasma have not been established by large-scale clinical studies. The unopened kit stores at 2–8 °C, subjecting the pre-coated capture antibody to none of the freeze-thaw cycling that progressively degrades binding affinity in kits stored under suboptimal conditions. Shipping occurs on gel packs with blue ice.
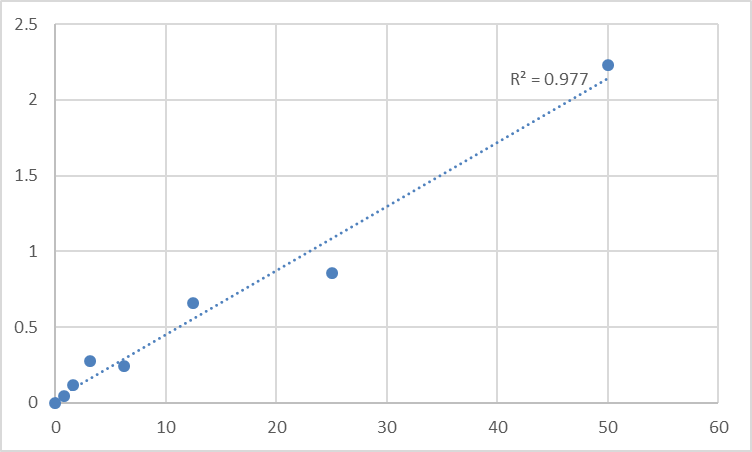
The protocol notes reflect genuine sandwich ELISA discipline rather than generic disclaimers. All reagents must warm to room temperature for at least 30 minutes before opening to prevent condensation on cold reagent vials from altering concentration. Pipette tips must be pre-rinsed and replaced between samples, standards, and reagents to prevent carryover contamination. Thorough mixing every 10 minutes using a low-frequency oscillator or gentle hand shaking is specified as critical for consistent color development, particularly given the small molecular weight of the target analyte and the potential for rapid binding kinetics. All standards and samples should be assayed in duplicate or triplicate. Do not mix components from different kit lots or use reagents beyond the kit expiration date. Unused wells must be kept desiccated at 4 °C in the sealed bag provided. These are the operating procedures that separate a standard curve with an R² above 0.99 from a dataset a reviewer will question.
The protein detected by KTE60084 occupies a unique position in the mitochondrial proteome that deserves explicit articulation because it explains why the kit exists at all. UQCR is not merely one subunit of Complex III; it is the subunit that physically tethers the Rieske iron-sulfur protein—the catalytic core that accepts electrons from ubiquinol and passes them to cytochrome c₁—to the cytochrome b scaffold within the inner mitochondrial membrane. The Rieske protein contains a 2Fe-2S cluster that undergoes a redox-dependent conformational change during the Q cycle, and UQCR stabilizes the protein in its membrane-embedded orientation, preventing the dissociation that would interrupt electron flow and generate superoxide. The functional relationship between UQCR and the Rieske protein is sufficiently intimate that UQCR has been described as an iron-sulfur protein binding factor, and its role in CIII assembly and RIP1 stability is documented in the UniProt annotation. When Nat10 suppresses Uqcr11 expression in cardiomyocytes, the resulting mitochondrial dysfunction is not attributable to a global Complex III deficiency; it is attributable to a specific defect in Rieske protein stabilization that weakens respiration at the ubiquinol oxidation step. Quantifying UQCR protein concentration is therefore not merely a measure of Complex III abundance—it is a measure of the capacity of the complex to maintain the iron-sulfur protein in its functional, membrane-bound conformation.
The clinical and translational implications of UQCR quantification extend across a range of diseases in which Complex III dysfunction has been mechanistically implicated. In hypertrophic cardiomyopathy, the UQCR11 homozygous mutation leads to mitochondrial dysfunction that manifests as reduced basal and maximal oxygen consumption. In heart failure, Nat10-mediated Uqcr11 suppression contributes to the metabolic shift from fatty acid oxidation to glycolysis that characterizes the failing myocardium. In gastric cancer, UQCRQ expression levels correlate with prognosis, suggesting that Complex III subunit stoichiometry influences tumor metabolic fitness and patient outcomes. In endometrial cancer, UQCR expression serves as a favorable prognostic marker. The UQCR11 gene has been associated with Bardet-Biedl Syndrome 18 and mitochondrial disease, and its related pathways include respiratory electron transport and Complex III assembly. In every one of these contexts, the ability to quantify UQCR protein concentration directly—not UQCR mRNA, not Complex III enzymatic activity, not citrate synthase-normalized mitochondrial content, but UQCR protein itself—is what separates a study that describes a Complex III phenotype from a study that quantifies the specific subunit alteration driving it.
The product page currently shows zero publications citing KTE60084. This is not a liability. It reflects the launch timing of a kit targeting a protein whose quantification has, until now, been confined to western blot densitometry and mass spectrometry-based proteomics. The kit enters a research landscape where the biological significance of UQCR is expanding—driven by high-profile publications in Nature Communications and the identification of UQCR11 mutations as causes of cardiomyopathy—and where the availability of a quantitative, specific, and accessible ELISA will enable the kinds of studies that generate citations. The technical specifications that will drive adoption are already documented: two-site sandwich ELISA architecture with capture and detection antibodies recognizing distinct UQCR epitopes, no significant cross-reactivity or interference with Complex III analogues, compatibility with serum, plasma, cell culture supernatants, and other biological fluids, a 3–5 hour assay duration, and storage at 2–8 °C.
For the mitochondrial biologist quantifying Complex III subunit stoichiometry in patient-derived fibroblasts, the cardiology researcher measuring UQCR as a biomarker of mitochondrial dysfunction in heart failure, the oncologist comparing UQCR expression between tumor subtypes as a prognostic indicator, the pharmacologist evaluating the effect of a Nat10 inhibitor on Uqcr11 expression in cardiomyocytes, or the basic scientist performing any experiment in which Complex III integrity is a variable rather than a confound, direct UQCR quantification is the measurement that converts a complex abundance phenotype into a subunit-specific molecular mechanism. KTE60084 provides that measurement in a sandwich ELISA format that distinguishes UQCR from the other ten subunits of Complex III, detects it in the biological matrices that actually contain the protein, and ships as a complete kit ready for same-day deployment. The smallest protein in the largest enzyme complex can now be quantified without ambiguity.
Explore specifications, access the protocol, and place your order here: https://www.abbkine.com/product/human-cytochrome-b-c1-complex-subunit-10-uqcr-elisa-kit-kte60084/





