




The Protein Your Liver Makes When Something, Anywhere, Is Wrong
A first-year medical resident learns C-reactive protein the way a ship captain learns the barometer. The absolute value matters less than the change over time, and a reading that doubles in six hours means something fundamentally different from a reading that drifts upward over three weeks. But the barometer analogy fails in one critical respect: a barometer reads atmospheric pressure, a single physical quantity. CRP is not a passive pressure gauge bolted to the hull of the immune system. It is an active participant in the inflammatory cascade, binding phosphocholine residues on damaged cell membranes and bacterial surfaces, engaging C1q to activate the classical complement pathway, and opsonizing debris for phagocytic clearance. Measuring CRP is not like reading a gauge. It is like measuring the output of a factory that is simultaneously reporting a fire and helping to extinguish it.
The pentraxin family to which CRP belongs is ancient and highly conserved across vertebrate evolution, and CRP itself is a pentameric disc composed of five identical non-glycosylated 206-amino-acid subunits arranged in cyclic symmetry around a central pore. Its hepatic synthesis is driven primarily by interleukin-6, with IL-1β and tumor necrosis factor-α serving as synergistic enhancers, and its plasma concentration can rise from baseline levels below 1 µg/mL to over 500 µg/mL within 48 hours of a potent inflammatory stimulus—a dynamic range of nearly three orders of magnitude that no other routinely measured clinical analyte approaches. That extraordinary dynamic range is both the reason CRP is clinically indispensable and the reason measuring it accurately across the full spectrum of biologically relevant concentrations has been an analytical challenge for decades.
High-sensitivity CRP assays were developed specifically to address the lower end of that spectrum—the 0.1 to 10 mg/L range where chronic, low-grade inflammation registers before it produces symptoms, before it accelerates atherosclerotic plaque formation, and before it elevates the risk of myocardial infarction, stroke, and cardiovascular death. Multiple prospective cohort studies have demonstrated that hs-CRP outperforms LDL cholesterol as a predictor of future cardiovascular events, and that individuals in the highest tertile of hs-CRP face a risk of myocardial infarction approximately three to seven times that of individuals in the lowest tertile. In cancer epidemiology, elevated CRP is associated with increased risk of prostate cancer, breast cancer, and colorectal cancer, and the relationship between chronic inflammation and carcinogenesis is now sufficiently established that CRP and interleukin-6 are considered dual sentinels of the inflammation-cancer axis. In infectious disease, CRP kinetics distinguish bacterial from viral etiologies with enough reliability to guide antibiotic stewardship decisions. In rheumatology, CRP levels track disease activity in rheumatoid arthritis and seronegative spondyloarthropathies. In transplant medicine, a rising CRP may herald graft rejection before creatinine climbs or echocardiographic abnormalities appear.
Yet for all its clinical ubiquity, CRP measurement in the research setting has been beset by a fragmentation problem. Clinical chemistry analyzers deliver CRP values from serum in roughly twelve minutes, but the per-sample cost assumes hospital-scale throughput and the instrumentation occupies an entire bench. Standard ELISA kits with nanogram-level sensitivity cannot resolve the sub-nanogram concentrations that define the low-risk cardiovascular stratum. And generic sandwich ELISA kits that claim reactivity with human CRP frequently exhibit cross-reactivity with serum amyloid P component (SAP, also designated pentraxin 2) or pentraxin 3, structural homologs within the pentraxin family whose independent biological functions—amyloid fibril stabilization for SAP, innate immune amplification for PTX3—render their co-detection analytically indefensible. When a researcher quantifies CRP in tumor-conditioned medium and that medium also contains SAP released from hepatocytes or PTX3 secreted by tumor-associated macrophages, the measured signal must be exclusively CRP-derived, or the resulting publication builds its conclusions on a summed pentraxin concentration rather than a CRP measurement.
EliKine™ Human CRP ELISA Kit (KTE6003) closes these gaps without overengineering the solution.
The kit employs a two-site sandwich ELISA in which a capture antibody specific for human CRP is pre-coated onto the microplate, standards and samples are introduced, and any CRP present is immobilized. After washing, a biotin-conjugated detection antibody recognizing a distinct CRP epitope is added, followed by streptavidin-conjugated horseradish peroxidase. A chromogenic substrate then develops color in direct proportion to the amount of CRP captured in the initial step. The entire assay—from the first reagent warming to the final plate reader export—requires three to five hours, depending on operator experience, which positions it as a same-day experiment rather than a multi-day protocol.
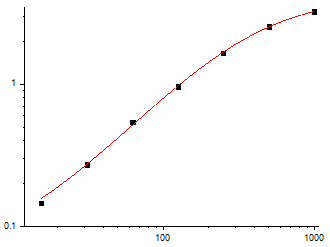
The analytical specifications are calibrated to the biological reality of CRP rather than to marketing convenience. The calibration range spans 15.6 pg/mL to 1,000 pg/mL, and the limit of detection reaches 8 pg/mL. At 8 pg/mL, the kit detects CRP at concentrations three orders of magnitude below the 1 µg/mL baseline of healthy human plasma—a sensitivity margin that enables researchers to quantify CRP in dilute biological matrices such as cerebrospinal fluid, bronchoalveolar lavage fluid, cell culture supernatants from unstimulated primary hepatocytes, and tissue homogenates where the interstitial CRP concentration is a small fraction of the plasma level. The kit achieves this sensitivity without sacrificing the upper end of its calibration range, meaning samples that span the full pathophysiological spectrum—from quiescent tissue to septic plasma—can be quantified without running separate low-sensitivity and high-sensitivity kit variants.
Specificity is the dimension where sandwich ELISA architecture most directly determines data quality. KTE6003 specifies that no significant cross-reactivity or interference between human CRP and structural analogues was observed. This is not a generic disclaimer. The pentraxin family includes CRP (pentraxin 1), serum amyloid P component (pentraxin 2), and pentraxin 3, all of which share the pentraxin domain fold and exhibit varying degrees of sequence homology. Monoclonal antibody cross-reactivity studies have demonstrated that anti-human CRP antibodies can exhibit weak but measurable binding to SAP and limulin, the horseshoe crab pentraxin. A sandwich ELISA that uses two antibodies targeting distinct CRP epitopes achieves specificity through dual recognition—both antibodies must engage the target for signal to develop, and a pentraxin that shares one epitope but not the other will not generate a signal. The resulting CRP measurement is a CRP measurement, not a summed pentraxin concentration.
Sample compatibility spans the biological matrices researchers actually use: serum, plasma, cell culture supernatants, and other biological fluids. Serum and plasma are the canonical sample types for systemic CRP quantification, and the kit's sensitivity range captures both the low baseline concentrations of healthy individuals and the dramatically elevated levels associated with acute infection, tissue injury, and chronic inflammatory states. Cell culture supernatant compatibility extends the kit's utility to the bench researcher studying CRP secretion from hepatocyte models, the tumor biologist quantifying CRP release from cancer cell lines, and the immunologist measuring CRP production in monocyte-hepatocyte co-culture systems. Cerebrospinal fluid CRP has emerged as a biomarker of neuroinflammation with particular relevance to multiple sclerosis, Alzheimer's disease, and post-infectious neurological syndromes. Bronchoalveolar lavage fluid CRP reflects pulmonary inflammatory activity. The kit's stated compatibility with "other biological fluids" accommodates these specialized sample types without requiring separate validation for each matrix.
The component list reflects a complete sandwich ELISA system: pre-coated Human CRP microplate, Human CRP standard, Human CRP detection antibody, avidin-HRP conjugate, standard diluent, assay buffer, HRP substrate, stop solution, wash buffer, and plate covers. The kit ships on gel packs with blue ice and stores unopened at 2–8°C, which means no -20°C freezer space consumed and no freeze-thaw cycling of antibodies that progressively degrades binding affinity. After opening, individual components should be stored according to the protocol specifications, and unused microplate wells must be kept desiccated at 4°C in the sealed bag provided.
The protocol notes reflect operational discipline accumulated through the testing of many sandwich ELISAs rather than generic laboratory disclaimers. All reagents must warm to room temperature for at least 30 minutes before opening. Pipette tips must be pre-rinsed with reagent and replaced between samples, standards, and reagents to prevent carryover contamination. Thorough mixing every 10 minutes using a low-frequency oscillator or gentle hand shaking is specified as critical for result quality. All standards and samples should be assayed in duplicate or triplicate. Components from different kit lots must not be mixed, and reagents must not be used beyond the kit expiration date. These are not warnings about exotic handling requirements. They are the operating procedures that separate a standard curve with an R² above 0.99 from a dataset that a reviewer will question.
The publication record for KTE6003 currently stands at one citation. For a recently launched ELISA kit in a market segment historically dominated by legacy products and generic alternatives, a single early citation—particularly when the methods section specifies the catalog number—is not a weakness. It is an independent laboratory's confirmation that the kit measures what it claims to measure and that the resulting values survive peer review. The kit enters a research landscape where CRP measurement spans neurology, cardiology, oncology, infectious disease, rheumatology, transplant medicine, and metabolic disease, and where the analytical requirements—picogram-level sensitivity, pentraxin-family specificity, multi-matrix compatibility—are functionally identical across all of these domains.
The broader research context continues to expand the relevance of CRP quantification. In Alzheimer's disease, elevated cerebrospinal fluid CRP has been associated with accelerated cognitive decline, and the protein's role in complement activation places it at the center of the emerging neuroinflammation hypothesis of neurodegeneration. In SARS-CoV-2 research, CRP levels at hospital admission were among the strongest predictors of progression to severe COVID-19 and mortality in multiple independent cohorts, and CRP-guided treatment algorithms have been incorporated into clinical management protocols. In oncology, the inflammation-cancer axis connecting CRP, IL-6, and tumor progression has motivated multiple CRP-lowering therapeutic strategies now in preclinical and early clinical development. In cardiology, the CANTOS trial demonstrated that targeting inflammation with canakinumab reduced cardiovascular events independently of lipid lowering, and the patients who benefited most were those with the highest baseline hs-CRP levels—establishing CRP not merely as a biomarker but as a therapeutically relevant inflammatory mediator.
For the cardiologist quantifying CRP in a prospective cohort study, the oncologist measuring CRP in tumor-conditioned medium, the neuroscientist profiling cerebrospinal fluid from Alzheimer's disease patients, the immunologist tracking CRP secretion from stimulated hepatocyte models, the infectious disease researcher monitoring CRP kinetics during experimental infection, or the basic scientist performing any experiment in which inflammation is a variable rather than a confound, direct CRP quantification is the measurement that converts a clinical observation into a mechanistic dataset. KTE6003 provides that measurement in a sandwich ELISA format whose sensitivity, specificity, and sample compatibility specifications are documented, whose protocol is transparent enough for a technician to execute on the first attempt, and whose single citation represents an independent validation that the kit produces data worthy of peer review.
The protein your liver manufactures when something, anywhere, is wrong—the ancient pentraxin that activates complement, opsonizes debris, and rises a thousand-fold in concentration within 48 hours of an inflammatory trigger—is now quantifiable with a kit whose lower detection limit reaches into the single-digit picogram range and whose specificity ensures that the signal at the end of the chromogenic reaction belongs to CRP and CRP alone. The barometer of the immune system can now be read with the precision that biological research demands.
Explore specifications, access the protocol, and place your order here: https://www.abbkine.com/product/elikine-human-crp-elisa-kit-kte6004/





