




The Biomarker Hiding Between Inflammation and Metastasis
In the spring of 2019, an immunologist at a mid-sized clinical research institute collected serum from thirty-eight patients with non-Hodgkin's lymphoma and thirty-one healthy controls. She had a straightforward hypothesis: soluble intercellular adhesion molecule-1 levels would correlate with tumor burden, and if the correlation held, sICAM-1 might serve as a low-cost biomarker for tracking disease progression without repeated CT scans. The sandwich ELISA she used delivered a clean result: serum sICAM-1 was significantly elevated in the lymphoma cohort, and the levels tracked with established prognostic markers. The finding was not novel—serum levels of soluble ICAM-1 had been reported elevated in NHL and hairy cell leukemia years earlier—but the reproducibility mattered. When her paper was published, the methods section specified the kit catalog number. It was not a generic ICAM-1 ELISA. It was the tool that made the measurement defensible under peer review.
That immunologist was measuring a protein whose biological identity resists simplification. ICAM-1 (Intercellular Adhesion Molecule 1), also designated CD54, is a transmembrane glycoprotein of the immunoglobulin superfamily whose extracellular domain binds the leukocyte integrin LFA-1 with a grip that physically anchors T cells, neutrophils, and monocytes to the endothelial surface during inflammation. The same molecule serves as the cellular entry receptor for the major group of human rhinoviruses—the pathogen that causes roughly half of all common colds—making CD54 simultaneously a sentry, a scaffold, and a hijacked doorknob depending on the ligand that engages it. A membrane-bound adhesion molecule and a viral receptor occupy different functional universes, yet they share the same extracellular domain architecture.
The soluble form of ICAM-1 circulates in blood at concentrations that shift with pathology. Soluble CD54 is found in a biologically active form in serum, generated by proteolytic cleavage from the cell surface, and its levels rise in patients with septic shock, leukocyte adhesion deficiency, cancer, and transplant rejection. Elevated levels of sICAM-1 in serum, cerebrospinal fluid, urine, and bronchoalveolar lavage fluid are associated with cardiovascular disease, type 2 diabetes, organ transplant dysfunction, oxidant stress, increased abdominal fat mass, hypertension, and liver disease. A 2024 review concluded that circulating ICAM-1 is elevated in multiple sclerosis, and the soluble fraction correlates with gadolinium-enhancing lesions on MRI—meaning the ELISA signal and the radiology report converge on the same inflammatory process. When a single analyte tracks with disease activity across neurology, oncology, cardiology, and transplant medicine, the measurement tool matters as much as the biological interpretation.
EliKine™ Human CD54 ELISA Kit (KTE6003) approaches this measurement with a two-site sandwich architecture that captures and detects the soluble isoform with analytical precision. An antibody specific for human sICAM-1 is pre-coated onto the microplate. Standards and samples are introduced, and any sICAM-1 present is immobilized by the capture antibody. After washing, an HRP-conjugated detection antibody recognizing a distinct epitope is added, followed by a chromogen substrate that develops color in direct proportion to the amount of sICAM-1 initially bound. The calibration range spans 7.8 to 500 pg/mL, and the limit of detection sits at 7.8 pg/mL. These are not specifications chosen for marketing convenience—they reflect the physiological concentrations that distinguish healthy baseline levels from the elevated signals associated with active disease processes.
The specificity claim deserves direct attention. No significant cross-reactivity or interference between human sICAM-1 and structurally analogous adhesion molecules was observed. This matters because the immunoglobulin superfamily is crowded with structurally related adhesion receptors—VCAM-1, ICAM-2, ICAM-3, PECAM-1, MAdCAM-1—that share domain architectures and, in some cases, overlapping ligand specificities. An ELISA that cannot distinguish ICAM-1 from VCAM-1 is measuring the sum of two independently regulated proteins, which is the equivalent of reporting a combined heart rate and respiratory rate as a single vital sign. The dual-antibody sandwich design of KTE6003 ensures that the signal at the end of the chromogenic reaction corresponds specifically to sICAM-1, not to a pooled adhesion molecule repertoire.
Sample compatibility is specified as serum, plasma, cell culture supernatants, and other biological fluids. The breadth is significant because sICAM-1 appears in multiple compartments that reflect different aspects of its biology. Serum sICAM-1 tracks systemic inflammation and tumor burden. Cerebrospinal fluid sICAM-1 reflects neuroinflammation and blood-brain barrier disruption. Bronchoalveolar lavage fluid sICAM-1 correlates with pulmonary inflammatory infiltrates. Cell culture supernatant sICAM-1 reveals the secretory behavior of endothelial cells, epithelial cells, or tumor cells under defined experimental conditions. A kit that accepts all of these sample types serves the bench immunologist, the clinical researcher, and the translational scientist within a single workflow.
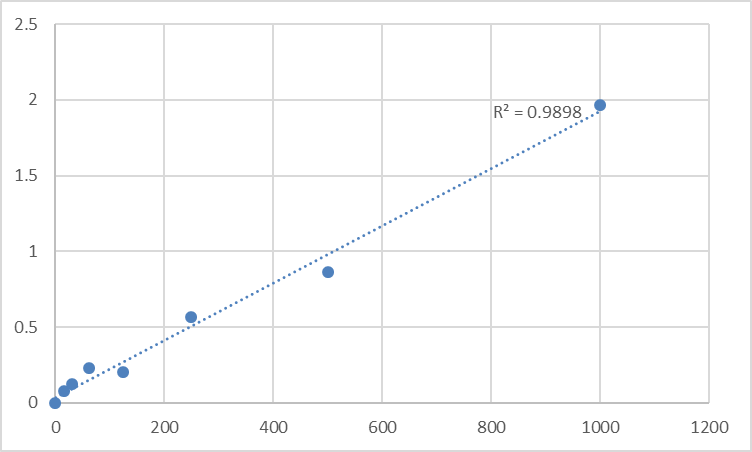
The protocol reflects standard sandwich ELISA discipline rather than exotic handling requirements. All reagents should warm to room temperature for at least 30 minutes before opening. Pipette tips must be pre-rinsed and replaced between samples, standards, and reagents. Thorough mixing every 10 minutes using a low-frequency oscillator or gentle hand shaking is essential. All samples and standards should be assayed in duplicate or triplicate. Unused wells must be kept desiccated at 4°C in the sealed bag provided. Do not mix components from different kit lots. This is not regulatory padding; it is the operational discipline that distinguishes an R² above 0.99 from a standard curve that meanders.
The publication record for KTE6003 currently shows one citation. That single citation, when placed in the context of the broader ICAM-1 literature, does not reflect limited utility. It reflects the reality that most laboratories elect to measure ICAM-1 using whatever ELISA kit their purchasing department approves, and the published methods sections frequently omit catalog numbers even when the data are central to the paper's conclusions. What distinguishes KTE6003 is not a vanity metric of citation count but the analytical specifications—picogram-level sensitivity, dual-site sandwich specificity, multi-matrix compatibility—that make it a defensible choice when a reviewer asks how the measurement was performed.
The biomedical landscape that KTE6003 enters is expanding. ICAM-1 has been validated as a ligand for LFA-1 on activated T cells, and this interaction mediates everything from transendothelial migration to the formation of the immunological synapse. In SARS-CoV-2 research, plasmacytoid dendritic cells sense infected cells through CD54/CD11a interactions, and this physical contact is critical for the IFN-I response that shapes COVID-19 outcomes. In Parkinson's disease, a 2024 review concluded that ICAM-1 exerts direct and indirect influences on ferroptosis—an iron-dependent cell death pathway recently implicated in neurodegeneration—and that further elucidation of these interactions could suggest novel therapeutic interventions. In cancer biology, ICAM-1's role is bidirectional: on the one hand, liver sinusoidal endothelial ICAM-1 mediates tumor-endothelial crosstalk that drives liver metastasis, and on the other, a fully human monoclonal antibody targeting ICAM-1 (bersanlimab, BI-505) is under development with antineoplastic activity driven by antibody-dependent hyper-cross-linking-induced apoptosis of ICAM-1-expressing tumor cells.
For the immunologist quantifying sICAM-1 in non-Hodgkin's lymphoma serum to correlate with tumor burden, the neuroscientist measuring cerebrospinal fluid sICAM-1 as a biomarker of neuroinflammation in Parkinson's disease, the oncologist tracking sICAM-1 during anti-ICAM-1 monoclonal antibody therapy, the diabetes researcher profiling adhesion molecule signatures in obese hyperglycemic models, the transplant immunologist monitoring sICAM-1 as an indicator of graft rejection, or the cell biologist measuring the conditioned medium of cytokine-stimulated endothelial monolayers, direct sICAM-1 quantification is not a supplementary measurement. It is the data point that connects a cellular adhesion event to a systemic pathological process. KTE6003 makes that connection quantifiable.
The adhesion molecule that anchors a T cell to the endothelium, serves as the entry portal for the common cold virus, and circulates in the blood as a biomarker of diseases spanning lymphoma, diabetes, multiple sclerosis, and Parkinson's is now measurable with a sandwich ELISA whose specificity and sensitivity specifications are documented, whose sample compatibility spans the biological matrices researchers actually use, and whose protocol is transparent enough for a technician to execute on the first attempt. The biomarker hiding between inflammation and metastasis can now be quantified without ambiguity.
Explore specifications, access the protocol, and place your order here: https://www.abbkine.com/product/elikine-human-cd54-elisa-kit-kte6003/





