




The Green Hemoprotein That Bleaches Your Arteries: Why Myeloperoxidase (MPO) Isn't Just a Neutrophil Marker — And How KTE61560 Puts the Oxidative Burden on a Plate-Readable Curve
Myeloperoxidase (MPO) is the only human enzyme whose product smells like a swimming pool. Stored in the azurophilic (primary) granules of every neutrophil and released in bulk during degranulation and NETosis, MPO catalyzes the deceptively simple reaction H₂O₂ + Cl⁻ → HOCl + H₂O — converting harmless peroxide into hypochlorous acid, the same bleach you buy in a jug, and the single most reactive oxidant the innate immune system deliberately deploys. That green tint you sometimes see in purulent fluid? That's ferric-oxy MPO (Fe³⁺-OH, λₘₐₓ ~470 nm). But the clinical reality is far more nuanced than "green pus = infection": circulating and plaque-associated MPO has been repeatedly pinned as a prognostic oxidant in acute coronary syndromes, vulnerable plaque rupture, ANCA-associated vasculitis, severe sepsis/ARDS, and even CKD progression, because HOCl doesn't stop at bacteria — it chlorinates cholesterol esters, modifies apoB, oxidizes phospholipids, and pits the vascular wall into a self-propagating oxidative inflammation loop. The Human Myeloperoxidase (MPO) ELISA Kit (KTE61560) from Abbkine is the tool that lets you quantify this dangerous hemoprotein as a calibrated sandwich-ELISA concentration (ng/mL), so your neutrophil-activation story rests on a number — not a MPO-DAB stain you squint at through a microscope.
MPO in One Paragraph: A ~150 kDa Heme Enzyme That Turns Your Own Peroxide Into Bleach
MPO (UniProt: P05164, Gene ID: 4350, Chr 17q23.1) is synthesized as a 90 kDa precursor (pre-pro-MPO) in the ER, routed through the endoplasmic reticulum–Golgi intermediate compartment (ERGIC) where it acquires its protoporphyrin IX (ferriprotoporphyrin IX = heme b) prosthetic group, then proteolytically matures into the active homodimer: two heavy chains (59–64 kDa each) disulfide-linked to two light chains (~13–15 kDa each), giving the mature, granule-stored complex a native ~140–155 kDa on non-reducing gels (light + heavy visible ~60–75 and ~13–15 on reducing).
The catalytic reaction everyone memorizes:
H₂O₂ + Cl⁻ → HOCl + H₂O (MPO + heme Fe³⁺ → Compound I → Compound II cycle)
The downstream chemistry is what makes MPO a biomarker worth measuring: HOCl rapidly chlorinates tyrosine → 3-chlorotyrosine, oxidizes LDL → MPO-oxidized LDL (highly atherogenic, taken up by macrophage scavenger receptors into foam cells), and reacts with NO → nitrosyl/hypochlorite species that disrupt endothelial NO signaling — a direct molecular bridge between neutrophil inflammation and endothelial dysfunction, plaque instability, and thrombogenicity.
Why an MPO ELISA — And Why "WBC Count + CRP" Misses the Enzyme That's Actually Doing the Damage
White blood cell count tells you how many neutrophils arrived. CRP tells you something inflammatory is happening. MPO tells you the neutrophil actually fired:
Question WBC CRP MPO (ELISA)
How many PMNs? ✅ ✗ ⚠︎ (indirect, if you normalize)
Systemic inflammatory load? rough ✅ ✗ (local enzyme, not systemic cytokine)
Did PMNs degranulate / NETose — and how much HOCl burden? ✗ ✗ ✅ (this is the one)
Plaque vulnerability / oxidative modification of matrix? ✗ ⚠︎ ✅ (MPO colocalizes to macrophage-rich shoulder region)
Vasculitis activity (ANCA, especially MPO-ANCA)? ⚠︎ ✅ ✅ (MPO-ANCA + circulating MPO mass both matter)
The critical sampling caveat: MPO is granular, not secreted — it reaches plasma/serum either by degranulation during the draw (poor phlebotomy technique = artefactual spike) or by NET release / ongoing vascular inflammation. That means sample handling is half the assay.
Assay Principle: KTE61560 — Sandwich ELISA (Pre-Coated)
The kit uses the field-standard architecture:
- A microplate is pre-coated with a capture antibody specific for human MPO.
- Standards (recombinant/calibrator MPO) and samples — serum, plasma, tissue homogenates, cell lysates, cell culture supernatants/lysates, other biological fluids — added → MPO binds.
- Wash → biotinylated anti-MPO detection antibody (different epitope) → Streptavidin–HRP.
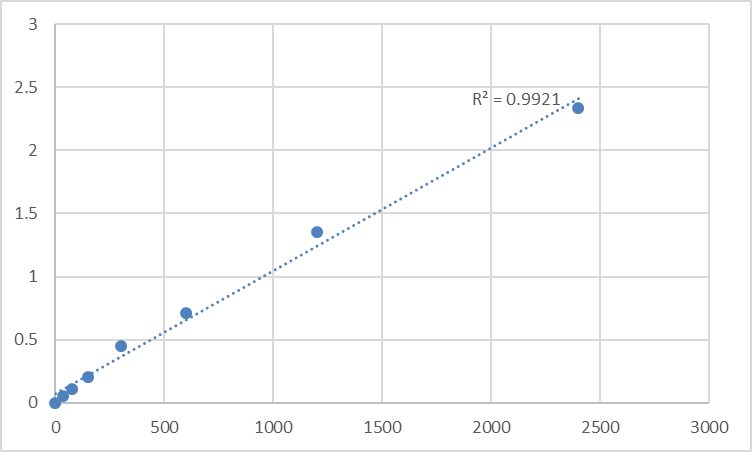
- TMB → stop → read 450 nm → interpolate unknowns from the MPO standard curve.
Typical performance envelope for this kit family (confirm exact range/recovery on your shipped CoA/datasheet):
Parameter Typical KTE61560-class Specification
Target Human MPO / Myeloperoxidase (UniProt P05164, ~140–155 kDa dimer)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → SA-HRP → TMB, 450 nm
Dynamic Range 0.156 – 10 ng/mL (7-point standard)
Sensitivity / LOD ~0.05–0.10 ng/mL
Intra-Assay CV < 8%
Inter-Assay CV < 10–12%
Specificity No significant cross-reactivity with other peroxidase family members (EPO, LPO) in physiological ranges
Samples Serum, plasma (EDTA preferred), tissue homogenates, cell lysates, culture supernatants
Assay time ~3–5 hours
Sample Handling: The 30-Minute Window That Decides Whether Your MPO Is Real or a Phlebotomy Artifact
Because MPO lives in azurophilic granules, the #1 rule is do NOT let neutrophils sit in the tube with the clot or in warm blood:
- Use EDTA tubes (chelates Ca²⁺, slows degranulation; citrate acceptable; avoid serum for "basal MPO" unless you specifically want the degranulation that occurs during clotting — just disclose it).
- Keep on wet ice immediately, invert gently, spin ≥ 1,500–2,000 ×g, 4°C, 10–15 min within 30–60 min of draw.
- Aliquot supernatant (plasma/platelet-poor if you can), snap to -80°C, and never freeze–thaw > once (MPO is stable when handled cold but adsorption + residual protease nibbling at room temp are real).
- If you must use serum: acknowledge that serum MPO ≥ plasma MPO in many donors because clotting triggers PMN degranulation — use it only if the study question is "total neutrophil activation burden including clotting cascade cross-talk."
Where MPO Quantification Actually Drives the Paper
- Acute Coronary Syndromes & Plaque Vulnerability (The "HOCl in the Cap" Hypothesis)
Unstable angina / NSTEMI plaques aren't just "more lipid" — they're MPO-rich shoulder regions where activated neutrophils have dumped HOCl-generating enzyme onto collagen and apoB lipoproteins. Multiple case-control and prospective cohorts have correlated plasma MPO (often a median around 30–70 ng/mL in healthy, spiking into 100–500+ ng/mL in ACS) with event risk independent of hs-CRP. Running KTE61560 on coded EDTA plasma banks lets you test whether MPO adds to the TIMI/GRACE + troponin + CRP risk model — and if your intervention (statins, colchicine, anti-IL-1β) actually brought the oxidative burden down.
- ANCA-Associated Vasculitis (AAV: GPA/MPA)
This is the canonical MPO-ANCA disease: autoantibodies to MPO (not just "against neutrophils") drive a pro-inflammatory, pro-NETotic loop where FcγR engagement + PR3/MPO antigen presentation amplifies small-vessel necrotizing vasculitis (pauci-immune RPGN, pulmonary capillaritis). Here, MPO ELISA plays two roles:
• Measuring circulating MPO mass (degranulation burden)
• Serving as the capture antigen for anti-MPO antibody ELISAs (if you're developing or running that assay in-house, the same kit's antibody pair is a building block)
- Sepsis, ARDS & Neutrophil Exhaustion
Severe sepsis = massive PMN turnover + NETosis flood + HOCl-mediated surfactant/albumin chlorination in the lung alveolus. BAL fluid and plasma MPO (ng/mL) are straightforward oxidative-burden markers to pair with PCT, IL-6, lactate, and 3-Cl-Tyr / HOCl-modified protein footprints — and because MPO is fast to run on a 96-well, it scales across time courses (0, 6, 24, 72 h) in a way LC-MS chlorotyrosine panels can't always afford.
- IBD: Mucosal Oxidative Injury
In active ulcerative colitis and Crohn's, mucosal MPO activity (often measured historically as TPO-like activity assay) correlates with PMI (polymorphonuclear infiltration index) and endoscopic severity. A sandwich ELISA on mucosal homogenates or (when available) luminal aspirates/washings gives you the protein mass that complements calprotectin and lactoferrin as a neutrophil-burden readout.
- Chronic Kidney Disease & Dialysis Leukopenia
HD-induced bioincompatible membrane contact → complement + neutrophil activation → MPO release → oxidative modification of albumin and lipoproteins → accelerated comorbidity. Monitoring pre- vs. post-dialyzer plasma MPO (paired with complement split products C3a/C5a) is a rational QA/QA-mechanism read.
- Cancer Microenvironment: MPO as a Double-Edentged Sword
Tumor-associated neutrophils can exist in N1 (anti-tumor, less MPO degranulation) vs. N2 (pro-tumor, pro-metastatic, high MPO/HOCl stress) polarization states. In some models, MPO-derived HOCl modifies the TME redox landscape enough to influence T-cell suppression vs. direct tumoricidal potential — measuring MPO protein in tumor-lysate / TAN-abundant zones (normalized to MPO-ANCA status, Ly6G/Ly6C, ARG1, iNOS) adds an oxidative-damage axis to the immune-landscape panel.
A Minimal Prep/QC Note (Because MPO Handling Is the Science)
• EDTA plasma preferred → process cold/fast → aliquot → -80°C → single thaw
• For tissue (atherosclerotic plaque, gut mucosa, kidney): homogenize cold in 50–100 mM Tris, pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100 + protease inhibitors + catalase scavenger optional (to protect the heme during prep if you're super-careful, though most commercial lysates just use inhibitors) → clarify → use supernatant → BCA → ng MPO / mg protein
• Warm kit reagents to RT ≥ 30 min before opening; protect TMB from light; stop uniformly; read 450 nm promptly; run full standard curve on every plate
The Bottom Line
MPO is the ~150 kDa green heme enzyme that turns your neutrophil's own peroxide into hypochlorous acid — the strongest oxidant the innate immune system intentionally makes, and the molecule most responsible for tipping that defense into plaque rupture, endothelial NO steal, chlorinated LDL foam-cell loading, and ANCA-driven small-vessel necrosis when the control systems fail. Measuring it demands more than a granule stain or a "WBC is up so MPO must be up" assumption. The Human Myeloperoxidase (MPO) ELISA Kit — KTE61560 from Abbkine gives you the right format to do it rigorously: pre-coated capture → biotin detection → HRP–TMB → 450 nm → ng/mL, over a 0.156–10 ng/mL working range, in a ~3–5 hour workflow that can be the difference between "neutrophils were there" and "they unloaded bleach while they were there."
Product Reference: KTE61560 – Human Myeloperoxidase (MPO) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-myeloperoxidase-mpo-elisa-kit-kte61560/
(For Research Use Only; not for diagnostic procedures in humans.)





