




The 65-kDa Polarity Scaffold Hiding in Plain Sight: Why MPP7 Quantification Finally Turns "Epithelial vs. Mesenchymal" From a Morphology Guess Into a Plate-Readable Number
There's a reason every epithelial biology lab can draw the tight junction diagram — ZO-1 on occludin on claudin, E-cadherin anchoring the actin belt — but almost nobody measures the adapter that actually assembles those complexes into a vectorial address code. That adapter is MPP7 (Membrane Palmitoylated Protein 7, also cataloged as MAGUK p55 subfamily member 7, UniProt: Q5T2T1/Q96LB1, Gene ID: 143098/144373), a ~65–80 kDa palmitoyl-modified MAGUK-family scaffold whose N-terminal PDZ domain grabs polarity determinants (LIN-7/VLP, indirectly CRB3-PALS1), whose SH3 domain mediates protein–protein wiring, and whose GUK-like domain (catalytically dead) tethers it into the DLG1 (SAP97/disc-large) complex at sites of epithelial cell–cell contact. When MPP7 is present and correctly localized, the epithelium knows up from down, apical from basal, sealed from leaky. When it drops or delocalizes, the cell may still express E-cadherin — but it no longer knows which direction to send a vesicle, where to build a junction, or when to stop proliferating. The Human MAGUK p55 subfamily member 7 (MPP7) ELISA Kit (KTE61556) from Abbkine is the reagent that finally lets you measure this polarity linchpin as a calibrated, two-site sandwich ELISA readout (ng/mL), so your EMT, kidney injury, or intestinal-barrier paper rests on a number — not a "ZO-1 looks断续 in the IF photo."
MPP7 in One Paragraph: A p55-Stardust MAGUK That Runs on Palmitate, Not Kinase Activity
The MAGUK p55 subfamily (named for Drosophila p55/Stardust) is defined by three modular folds in the order PDZ → SH3 → GUK-like — and MPP7 (aliases: Palmitoylated membrane protein 7, RP11-218D6.5) is the mammalian "workhorse architect" that holds this fold at epithelial membranes:
Domain Function Why It Matters
PDZ (N-term) Binds C-terminal class I motif (-ETDV / -XΦXΦ) on polarity partners (LIN-7/MALS, CRB3 tail region in kidney intestine) Positions the complex at the apical-lateral boundary (the "fence" where tight junctions sit)
SH3 Binds proline-rich regions on adaptors (DLG1-interacting surfaces) Provides the mechanical tether to the larger MAGUK scaffold network
GUK-like (inactive) Lacks key catalytic residues → serves as a protein–protein docking pad (not a guanylate kinase) Keeps DLG1/SAP97 in a productive alignment without spurious nucleotide signaling
C-terminal palmitoylation cysteines Dual Cys palmitoylation → stable membrane association at inner leaflet near junctional actin Explains why MPP7 is a membrane-proximal polarity landmark, not a cytosolic float
The biological bottom line: MPP7 is an address-code reader. It translates "I am at the right spot on the lateral membrane" into "build a tight junction here and send transporters apical." When that code breaks, epithelia don't just leak — they lose positional authority and start behaving like motile mesenchyme.
Why a Sandwich ELISA for MPP7 — And Why "E-cad/ZO-1 IF Only" Leaves the Mechanistic Hole
MPP7 is membrane-associated (palmitoylated), ~65–80 kDa, and moderate abundance — which means:
- It's easy to miss in a whole-lysate gel if your extraction under-represents the membrane/palmitoyl pool (Triton X-100 soluble vs. insoluble split matters).
- EMT "looks" partial on IF — cells can lose MPP7 before E-cadherin fully disappears, and that early polarity erosion is exactly what predicts invasive switch, but you can't plot it off a photo.
- Cohort/banked samples (biopsies, resections, cell-line panels) demand a plate-readout with CVs, not a 6% gel transfer debate.
The KTE61556 kit solves this with the classic architecture:
- Microplate pre-coated with capture anti-MPP7.
- Standards (recombinant human MPP7) + samples — serum, plasma, tissue homogenates, cell culture supernates/lysates — added → MPP7 binds.
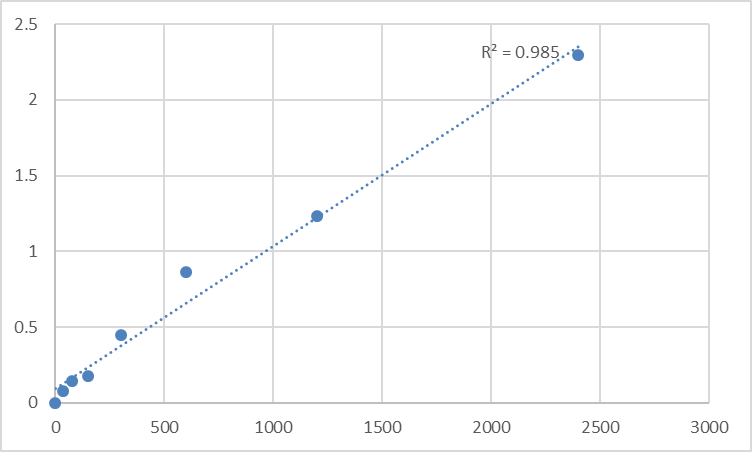
- Wash → biotinylated anti-MPP7 detection (different epitope) → Streptavidin–HRP → TMB → color ∝ bound MPP7.
- Stop → 450 nm → interpolate ng/mL from the standard curve.
Consolidated performance envelope (from distributor/technical summaries aligned with this kit class):
Parameter Specification
Target Human MPP7 / MAGUK p55 subfamily member 7 (UniProt Q5T2T1, Gene 143098)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → SA-HRP → TMB, 450 nm
Dynamic Range 0.156 – 10 ng/mL
Sensitivity / LOD ~0.078 ng/mL
Intra-Assay CV < 6–8%
Inter-Assay CV < 8–10%
Samples Serum, plasma, tissue homogenates, cell culture supernates/lysates, other biological fluids
Assay time ~3–5 hours
(Confirm exact dilution scheme and lot-specific recovery on the Abbkine datasheet for KTE61556.)
Where Quantifying MPP7 Actually Carries the Paper
- Epithelial-Mesenchymal Transition (EMT) & Cancer Invasion — The "Polarity Collapse" Axis
The canonical EMT markers (E-cad↓, N-cad↑, vimentin↑, Snail/Slug↑) tell you "the cell changed shape." MPP7 tells you the address system fell before the shape did: early EMT often shows MPP7 delocalization / cytoplasmic redistribution while total E-cadherin is still detectable by Western — and that distinction is what predicts whether the cell is merely "reorganizing" or has crossed into invasive-mode with loss of apical-basal identity.
Run KTE61556 on TGF-β/ TNF-treated monolayers, Snail/Snail-ER lines, or patient-derived organoids, normalize to mg total protein (BCA), and correlate ΔMPP7 with trans-epithelial resistance (TEER) drop, dextran-flux, and ZO-1/E-cad junctional IF discontinuity. That's the triad reviewers respect: shape + barrier + scaffold quantity.
- Renal Proximal Tubule & Glomerular Barrier Biology
The kidney is arguably the most architecturally demanding epithelium in the body — and MPP7's PDZ network (CRB3-PALS1-LIN-7) is central to proximal tubule apical identity and tight junction fence function. Ischemic AKI, cisplatin nephrotoxicity, and proteinuric states erode polarity; quantifying MPP7 in cortical lysates (normalized to Na⁺/K⁺-ATPase α1 or AQP1 for segment identity) gives you a polarity-integrity readout that creatinine/ BUN can't see.
- Intestinal Barrier & IBD / Mucosal Healing
The intestinal crypt–villus axis lives on a strict apical-basal address code; MPP7 sits at the intermediate zone where absorptive enterocytes declare "apical starts here." In models of DSS colitis, TNBS, or anti-TNF (loss-of-barrier mimics), tracking MPP7 (protein + IF zonation) alongside claudin-2↑/claudin-5↓, FITC-dextran 4kDa flux, and myeloperoxidase lets you separate "inflammation is present" from "the address code is erased."
- Bone Mineral Density & Skeletal Epithelial Niche (The GWAS Connection)
A subtler but fascinating angle: polymorphisms near/within MPP7 are associated with site-specific BMD variation (the product listing itself notes this), linking polarity/scaffold genetics to osteoblast/stromal niche architecture in weight-bearing sites. If your lab works on skeletal intercellular communication or marrow-adjacent epithelioid stroma, MPP7 ELISA offers a protein-level handle on a GWAS-implicated locus.
- 3D Organoid & Polarity Rescue (The "Does It Luminate?" Question)
iPSC-derived gut/kidney/cholangiocyte organoids either lumenate and polarize (MPP7+ apical border forms) or collapse into solid, disorganized masses. Quantifying MPP7 in organoid lysates across passages or rescue constructs gives you a quantitative polarity score to complement apical marker secretion (alkaline phosphatase, dipeptidase-1, CFTR trafficking) and basolateral readouts.
- CRISPR/AAV Validation
Editing MPP7 or CRB3/PALS1? Don't just show "junctions look messier." Report % MPP7 protein remaining ± SEM from the calibrated ELISA (ng/mg), co-show ZO-1/occludin IF zonation index, and tie it to the functional payout — TEER, permeability, or invasion through Matrigel. That's how you prove the scaffold — not just the "stain" — was the causal node.
A Minimal Prep Note (MPP7 Is Palmitoylated — Treat It Like a Membrane Protein)
• For epithelial monolayers / tissue (intestine, kidney, liver bile duct):
Homogenize cold in 50 mM Tris pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100 + protease inhibitors + 1 mM PMSF + 10 mM iodoacetamide (iodoacetamide helps preserve palmitoylation state if you're doing parallel PTM work; for total-protein ELISA it's optional but good hygiene).
Clarify 12,000–16,000 ×g, 15 min, 4°C → supernatant contains the Triton-soluble MPP7 pool (where the PDZ-SH3-GUK scaffold lives).
• BCA the same final lysate → express as ng MPP7 / mg total protein.
• Warm kit reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; and run the full standard curve on every plate — membrane-scaffold recoveries shift with lipid content, and the curve is your insurance.
The Bottom Line
MPP7 is the ~65 kDa, palmitoylated PDZ–SH3–GUK-like scaffold that tells an epithelial cell where it is, which way is up, and where to build the tight junction fence — and when that address code erodes, morphology follows, barrier collapses, and invasion becomes possible even before E-cadherin vanishes from the blot. Measuring it as a calibrated variable instead of a "maybe it's fainter" band changes your epithelial biology story from descriptive to quantitative. The Human MAGUK p55 subfamily member 7 (MPP7) ELISA Kit — KTE61556 from Abbkine gives you that variable: pre-coated capture → biotin detection → HRP–TMB → 450 nm → ng/mL, over a 0.156–10 ng/mL working range with LOD ~0.078 ng/mL, in a ~3–5 hour workflow that scales from an EMT time-course to a tissue-bank cohort without chaining you to a gel rig.
Product Reference: KTE61556 – Human MAGUK p55 subfamily member 7 (MPP7) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-maguk-p55-subfamily-member-7-mpp7-elisa-kit-kte61556/
(For Research Use Only; not for diagnostic procedures in humans.)





