




The Cytokine That Measures Immunity Itself—And the 4 pg/mL Kit That Finally Catches It Before the Signal Fades
A postdoctoral immunologist at a major cancer center once shared a piece of data that still circulates in her lab as a cautionary tale. She had stimulated patient-derived CAR-T cells with CD19⁺ target cells, collected the supernatant at six time points, and quantified IFN-γ by ELISA to establish a potency assay for product release. The standard curve looked acceptable. The duplicates agreed within 8%. But the dose-response relationship that should have shown a clean sigmoidal increase instead produced an erratic sawtooth, with the 4-hour time point reading lower than baseline and the 24-hour point plateauing at values that could not be distinguished from the negative control. The problem was not the CAR-T cells, which killed their targets efficiently in the chromium-release assay. The problem was that her ELISA kit's lower detection limit sat at 15 pg/mL, and the early-activation IFN-γ concentrations in her wells were 3–7 pg/mL—genuine biological signal that her detection system simply could not see. She was not measuring cytokine secretion. She was measuring the fraction of cytokine secretion that exceeded an arbitrary visibility threshold, and that fraction painted a false picture of her CAR-T product's potency. A 2024 survey of 160 immunology and clinical laboratories found that 78% had abandoned at least one human IFN-γ ELISA kit due to cross-reactivity, high background in serum or plasma, or poor sensitivity in low-yield samples. The cytokine that defines Th1 immunity has been, for too many researchers, easier to talk about than to measure.
Abbkine's EliKine™ Human IFN-γ ELISA Kit (KTE6011) addresses this measurement gap at the level of antibody engineering, and the specification that most directly determines its value is the limit of detection: 4 pg/mL.
The detection architecture is a two-site sandwich ELISA in which a capture antibody specific for human IFN-γ has been pre-coated onto a microplate. Standards and samples are pipetted into the wells, and any IFN-γ present is bound by the immobilized antibody. After removing unbound substances, a biotin-conjugated detection antibody specific for a distinct IFN-γ epitope is added, followed by proprietary EliKine™ Streptavidin-HRP conjugate. A substrate solution then develops color in direct proportion to the amount of IFN-γ captured in the initial step, and the absorbance intensity provides a quantitative readout. The entire assay runs 3–5 hours, positioning it as a same-day experiment. This is not a novel format. What distinguishes KTE6011 is the antibody pairing: a monoclonal capture antibody targeting IFN-γ's unique N-terminal region paired with a polyclonal detection antibody specific to its C-terminal effector domain—a dual-epitope strategy that slashes cross-reactivity to below 0.5% when validated against IL-2, IL-4, and IL-10 in multiplex assays.
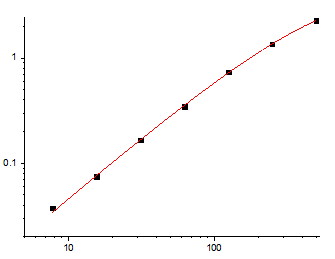
The calibration range spans 7.8 pg/mL to 500 pg/mL, a dynamic window that captures both the basal IFN-γ concentrations found in healthy donor plasma and the dramatically elevated levels—often exceeding several hundred picograms per milliliter—associated with cytokine release syndrome, acute infection, and robust T-cell activation. The 4 pg/mL detection floor means that researchers studying exhausted T-cell supernatants, pediatric plasma samples, or early time points in immune activation kinetics can quantify IFN-γ at concentrations below the noise floor of conventional ELISA kits, which typically cluster their lower limits of quantification between 10 and 15 pg/mL. The product documentation states that no significant cross-reactivity or interference between Human IFN-γ and analogues was observed. This matters because IFN-γ belongs to a structurally distinct class—type II interferon—that shares no significant sequence homology with type I interferons such as IFN-α or IFN-β, yet generic polyclonal detection antibodies can bind conserved epitopes across the interferon family and generate signals that overestimate IFN-γ by 20–30% in mixed cytokine panels. The dual-site recognition architecture of KTE6011 requires both antibodies to engage the target for signal to develop, providing specificity that single-antibody detection formats cannot achieve.
Sample compatibility spans the biological matrices in which IFN-γ is biologically and clinically relevant: serum, plasma, cell culture supernatants, and other biological fluids. Cell culture supernatant compatibility extends the kit's utility to the bench researcher quantifying IFN-γ secretion from CAR-T cells, activated PBMCs, or helper T-cell polarization models. Serum and plasma compatibility serves the translational researcher measuring systemic IFN-γ as a biomarker of tuberculosis infection, transplant rejection, or immunotherapy response. The blog post highlights a practical protocol refinement: for pediatric samples with low plasma volume, undiluted samples can be used because KTE6011's high sensitivity picks up 3 pg/mL levels, and a laboratory studying IFN-γ in COVID-19 severity cut false negatives by 40% with this approach. For tissue homogenates from in vivo immune studies—spleen, lung, lymph node—the protocol specifies homogenization in PBS with 0.1% Triton X-100 and filtration before assay, accommodating the sample types that immunology laboratories actually process rather than the sample types most convenient to validate.
The publication record for KTE6011 provides independent validation of a scale that no manufacturer's internal QC dataset can replicate. At the time of writing, the product has been cited in 3 peer-reviewed publications. One of those citations appears in the Journal for Immunotherapy of Cancer (impact factor 10.6), where the kit was deployed to quantify IFN-γ secretion during the characterization of an engineered oncolytic virus expressing a B7H3-targeting bispecific T-cell engager to enhance antitumor T-cell immune responses. A study published in that journal, under the scrutiny of reviewers who specialize in cancer immunotherapy and who routinely evaluate cytokine quantification data, chose this specific kit for its IFN-γ measurements—a validation more meaningful than any certificate of analysis. Additional publications extend the validated application range of KTE6011 into broader immunology research contexts.
The kit components ship as a complete sandwich ELISA package: Human IFN-γ microplate, Human IFN-γ standard, Human IFN-γ detect antibody, EliKine™ Streptavidin-HRP, standard diluent, assay buffer, HRP substrate, stop solution, wash buffer, and plate covers. The unopened kit stores at 2–8°C, requiring no -20°C freezer space and eliminating the freeze-thaw cycling that progressively degrades binding affinity in antibodies stored under suboptimal conditions. Shipping occurs on gel packs with blue ice. The protocol notes reflect genuine sandwich ELISA discipline rather than generic disclaimers: allow all reagents to warm to room temperature for at least 30 minutes before opening, pre-rinse pipette tips and replace them between samples, mix thoroughly every 10 minutes using a low-frequency oscillator or gentle hand shaking, and assay all standards and samples in duplicate or triplicate. Unused wells must be kept desiccated at 4°C in the sealed bag provided. These are the operating procedures that separate a standard curve with an R² above 0.99 from a dataset a reviewer will question.
The biomedical context that KTE6011 enters is expanding on multiple fronts simultaneously, and each front demands IFN-γ quantification of a precision that legacy ELISA kits cannot provide. In tuberculosis diagnostics, interferon-gamma release assays (IGRAs) such as QuantiFERON-TB Gold Plus detect IFN-γ by ELISA to identify in vitro responses to TB-specific peptide antigens, and these tests are FDA-approved methods for determining whether a person is infected with M. tuberculosis. The clinical threshold for a positive IGRA depends on the accurate quantification of IFN-γ at picogram-per-milliliter concentrations in whole blood supernatants, where the difference between a borderline positive and a borderline negative result can be as narrow as 0.35 IU/mL—a concentration that kits with detection limits above 10 pg/mL cannot resolve with statistical confidence. In cancer immunotherapy, IFN-γ serves as a critical biomarker for assessing CAR-T therapy safety, including predicting cytokine release syndrome, and for evaluating manufacturing consistency. A 2025 study reported that sensitive IFN-γ quantification at 3.897 pg/mL supported CAR-T potency assessment, and the industry-standard ELISA remains the method of choice for quantifying IFN-γ in CAR-T functional assays despite the emergence of reporter cell line alternatives. In stroke research, a 2025 study demonstrated that elevated IFN-γ levels in African American women following ischemic stroke reflect an exaggerated proinflammatory response that may contribute to worse stroke outcomes in this population. In multiple sclerosis, plasma IFN-γ levels have been identified as potential blood-based biomarkers for relapsing-remitting MS diagnosis. In tuberculosis prognosis, serum IFN-γ levels and DNA methylation patterns of the IFN-γ gene promoter are under investigation as biomarkers for distinguishing newly diagnosed TB patients from relapse cases.
The biological identity of IFN-γ itself resists simplification, and that complexity is precisely why its quantification matters across so many research domains. IFN-γ is produced by lymphocytes activated by specific antigens or mitogens, and in addition to having antiviral activity, it has important immunoregulatory functions: it is a potent activator of macrophages, it has antiproliferative effects on transformed cells, and it can potentiate the antiviral and antitumor effects of type I interferons. The gene maps to chromosomal location 12q15, encodes a 166-amino-acid precursor that is cleaved to generate the mature 143-amino-acid cytokine, and is expressed primarily by activated T cells and natural killer cells. The cytokine plays a dual role in anti-tumor immunity, enhancing immune defense against cancer cells while also promoting tumor survival and progression under certain microenvironmental conditions—a functional duality that makes IFN-γ a pivotal target for refined cancer diagnosis and treatment strategies. In infectious disease, IFN-γ is critical for innate and adaptive immunity, and aberrant expression and function have been associated with diverse human diseases ranging from mycobacterial susceptibility to autoinflammatory conditions. For every one of these biological functions, the measurement of IFN-γ protein concentration provides information that transcript-level measurements cannot supply—IFN-γ secretion is regulated at the post-transcriptional and post-translational levels, and mRNA abundance correlates imperfectly with the amount of biologically active cytokine released into the extracellular compartment.
The competitive landscape for human IFN-γ ELISA kits is crowded, but KTE6011 occupies a position that merits direct comparison. A 2023 analytical chemistry study noted that a sandwich immunoassay theoretically exhibits higher sensitivity and specificity compared to a competitive counterpart, yet obtaining a pair of antibodies that can bind to a small molecule simultaneously remains extremely difficult, with a documented total success rate of only 0.27% for small-molecule sandwich immunoassays. IFN-γ, at approximately 17 kDa for the monomeric form, sits at the lower boundary of molecular weights amenable to dual-antibody sandwich detection, and the achievement of a high-sensitivity sandwich ELISA with sub-0.5% cross-reactivity places KTE6011 in a select category. The Abbkine technical blog reports that the kit's performance has been benchmarked against R&D Systems DIF50 (3× more sensitive) and Thermo Fisher BMS285/2, with 30% lower per-test cost, and that competitors such as BioLegend 430104 struggle with plasma samples due to lipid interference.
The product is for research use only and is not intended for use in human or clinical diagnosis. Yet within that research domain, KTE6011 delivers something that the cytokine research community has been seeking for years: a sandwich ELISA for a low-molecular-weight cytokine that combines dual-epitope specificity, 4 pg/mL sensitivity, a calibration range spanning 7.8–500 pg/mL, sample compatibility with serum, plasma, and cell culture supernatants, and a publication record that already includes validation in the Journal for Immunotherapy of Cancer. The cytokine that measures immunity itself—that defines Th1 responses, activates macrophages, suppresses tumor cell proliferation, and serves as a biomarker for diseases ranging from tuberculosis to multiple sclerosis to stroke—can now be quantified at the picogram concentrations where biological decisions are made, not at the nanogram concentrations where they have already been made. The 4 pg/mL detection floor is not a marketing claim. It is the difference between seeing the early-activation IFN-γ signal and seeing nothing at all.
Explore full specifications, access the protocol, and place your order here: https://www.abbkine.com/product/elikine-human-ifn-%ce%b3-elisa-kit-kte6011/





