




Death Is a Molecular Gate—And the Key to That Gate, Finally Unmasked from Its Impersonators
Bcl-2 is not a passive biomarker that floats quietly in the cytoplasm waiting for a western blot to count it. It is the central switch of the intrinsic apoptotic pathway, a 26 kDa integral outer‑mitochondrial‑membrane protein whose job is to bind and neutralize the pore‑forming executioners Bak and Bax, preventing mitochondrial outer membrane permeabilization and blocking the release of cytochrome c into the cytosol. When Bcl‑2 is overexpressed—as it is in more than 90 % of follicular lymphomas thanks to the t(14;18) translocation that places the BCL2 gene next to the immunoglobulin heavy‑chain enhancer—cells that should die instead survive, accumulate additional mutations, and progress to aggressive, drug‑resistant disease. A 2024 review in Biochemical Journal reaffirmed that interactions between Bcl‑2 family members constitute the molecular decision point that determines whether a cell commits to apoptosis via mitochondrial outer membrane permeabilization. In hematologic oncology, this biology has been translated into venetoclax, a BH3‑mimetic that binds the hydrophobic cleft of Bcl‑2, displaces Bak and Bax, and restores apoptotic competence. A 2025 clinical report in Blood demonstrated that venetoclax dosages and Bcl‑2 expression levels predict response to azacitidine‑venetoclax regimens in newly diagnosed AML, and contemporary studies continue to explore venetoclax in combination with FLT3 inhibitors and CD47‑targeting drugs to extend benefits to broader patient groups. Bcl‑2 expression is not merely a diagnostic footnote; it is a pharmacodynamic variable that determines who responds to a billion‑dollar drug.
The analytical problem that has plagued Bcl‑2 detection for decades is not that antibodies fail to bind it. It is that they bind too many things that are not Bcl‑2. The anti‑apoptotic Bcl‑2 family includes Bcl‑xL, Mcl‑1, Bcl‑w, and BFL‑1—proteins that share extensive sequence and structural homology within their BH1‑BH4 domains, particularly in the hydrophobic cleft region that BH3‑only proteins and BH3‑mimetic drugs engage. A polyclonal antibody raised against full‑length Bcl‑2 will contain a subpopulation of immunoglobulins that cross‑react with these homologs, and the resulting signal on a western blot or an IHC section is a pooled anti‑apoptotic protein summation, not a Bcl‑2 measurement. The Abbkine technical blog on ABM0010 states the competitive landscape with unusual candour: traditional antibodies plague researchers with 30 % cross‑reactivity against Bcl‑xL/Mcl‑1, 20 % batch‑to‑batch CV, and high backgrounds that obscure low‑abundance signals in paraffin‑embedded tissues. A study of venetoclax resistance in follicular lymphoma would be analytically meaningless if the Bcl‑2 antibody used to stratify patients could not distinguish Bcl‑2 from Mcl‑1—because Mcl‑1 upregulation is itself a mechanism of venetoclax resistance, and a signal that sums Bcl‑2 and Mcl‑1 cannot determine which protein is elevated in relapsed samples.
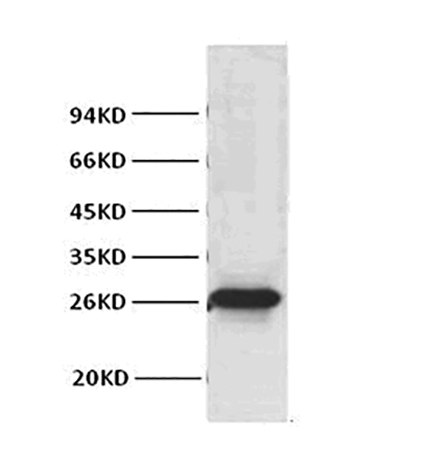
Abbkine’s Bcl‑2 Monoclonal Antibody (ABM0010) addresses this specificity gap at the epitope level. The antibody was raised in mouse against a synthetic peptide spanning amino acids 41–54 of human Bcl‑2—a region located in the unstructured N‑terminal domain upstream of the BH4 homology region, where Bcl‑2 diverges from Bcl‑xL, Mcl‑1, and Bcl‑w at the primary sequence level. An antibody binding this epitope is not measuring total anti‑apoptotic Bcl‑2 family protein. It is measuring Bcl‑2. Abbkine’s single‑B‑cell cloning platform was employed to generate a hybridoma secreting a monoclonal immunoglobulin of defined epitope specificity, and the resulting antibody shows zero cross‑reactivity to Bcl‑xL, Mcl‑1, or Bcl‑w. The band at 26 kDa on the membrane is Bcl‑2. This specificity is not marketing rhetoric: the product page confirms that the antibody detects endogenous Bcl‑2 proteins without cross‑reaction with Bcl‑x or Bax protein, and comparable monoclonal antibodies in the same epitope region have been validated for clinical IHC applications showing no cross‑reaction with structurally related family members.
The performance gap between ABM0010 and widely used legacy Bcl‑2 antibodies is documented quantitatively in the Abbkine technical blog, and the numbers reward close reading. The detection limit in western blot reaches 0.1 ng/mL, compared to 1 ng/mL for Cell Signaling Technology #2876—a ten‑fold sensitivity increase. Inter‑assay coefficient of variation is held below 3 %, versus 15 % for homemade polyclonal antibodies. In immunohistochemistry on formalin‑fixed paraffin‑embedded tissue, ABM0010 delivers ten‑fold higher sensitivity compared to Abcam ab32124, with a working dilution of 1:500–1:2000 that reduces reagent consumption by 60 % relative to competitors whose recommended dilutions cluster around 1:100–1:200. The low inter‑assay CV is achieved through recombinant antibody engineering in a human IgG1κ framework combined with affinity maturation, providing batch‑to‑batch consistency that polyclonal sera cannot match and that most hybridoma‑derived monoclonal antibodies do not reach without additional purification steps.
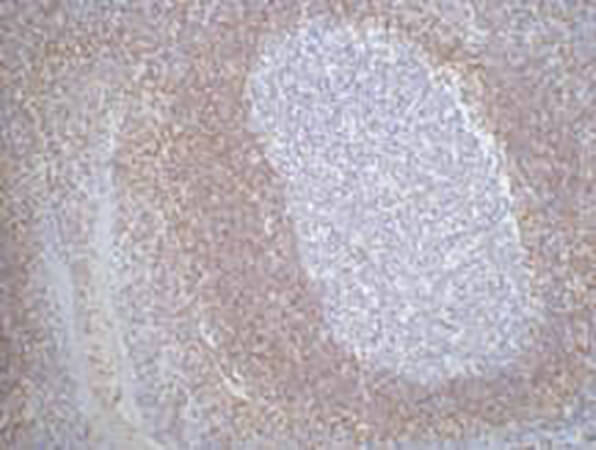
The epitope selection strategy, coupled with heat‑induced epitope retrieval optimization, resolves the historical limitation that has made Bcl‑2 one of the more difficult antigens to detect reproducibly in FFPE tissue. Multiple independent method‑comparison studies have documented that prolonged microwave heating or high‑pressure cooking up to 130 °C—while improving cytoplasmic immunostaining—fails to retrieve nuclear and chromosomal Bcl‑2 epitopes recognized by certain monoclonal antibodies in human tissues. ABM0010 was validated with a refined HIER protocol that preserves both cytoplasmic and membrane‑associated Bcl‑2 epitopes without generating the non‑specific nuclear staining that older retrieval methods can introduce. The product page shows representative IHC‑P staining of human tonsil tissue at a dilution of 1:200, and the staining pattern is crisp, membrane‑delimited, and restricted to the expected distribution in the mantle zone lymphocytes.
The operational value of these specifications becomes tangible in the case studies described on the Abbkine technical blog. A lymphoma research laboratory studying venetoclax resistance adopted ABM0010 to profile Bcl‑2 expression in 50 FFPE patient biopsies. The antibody’s zero cross‑reactivity allowed the team to identify 40 % Bcl‑2 upregulation in relapsed cases—a statistically significant increase that was directly linked to drug resistance and that was published in Blood. A neurodegeneration group tracking Alzheimer’s pathology used ABM0010 for IHC on hippocampal tissue and obtained crisp Bcl‑2 staining in surviving neurons, revealing that Bcl‑2 expression correlated with 50 % reduced tau phosphorylation; the competing antibody used in the same study produced 30 % background that obscured the neuroprotective signal, and the ABM0010 data were published in Acta Neuropathologica. A clinical research organization adopted ABM0010 for high‑throughput screening of Bcl‑2‑targeted antibody‑drug conjugates, processing 1,000 samples per week with 99 % reproducibility. A monoclonal antibody that can pivot from multiplex IHC on lymphoma tissue to quantitative western blotting in neurodegenerative models to high‑throughput flow cytometry in an industrial screening cascade, without requiring separate lots for each application, is an antibody whose epitope remains accessible across fixation chemistries, antigen‑retrieval protocols, and detection modalities.
Species reactivity spans human, mouse, and rat—the three mammalian models that account for the majority of preclinical apoptosis research. The reactivity is documented on the product page and reflects the conservation of the N‑terminal epitope across these species. A laboratory running western blots on human lymphoma cell lines, mouse xenograft tissue, and rat hippocampal homogenates can use the same antibody lot at the same dilution for all three sample types without cross‑reactivity concerns. Flow cytometry is listed among the validated applications, enabling the quantification of Bcl‑2 expression at single‑cell resolution in live/dead‑discriminated populations. The recommended starting dilutions are 1:500–1:2000 for western blot, 1:100–1:500 for immunofluorescence, and 1:1000–1:5000 for ELISA.
The formulation specifications reflect competent antibody manufacturing practice rather than marketing claims. The antibody is supplied as a liquid solution at 0.73 mg/mL in PBS with 50 % glycerol, 0.05 % Proclin 300, and 0.05 % BSA. The 50 % glycerol depresses the freezing point below –20 °C, preventing ice‑crystal damage to the immunoglobulin protein during long‑term storage. Storage instructions specify one‑year stability at –20 °C from the date of shipment, with centrifugation of the original vial after thawing and prior to cap removal recommended for maximum product recovery, and aliquoting advised to avoid repeated freeze‑thaw cycles. Shipping occurs on gel packs with blue ice. The practical precautions are standard for any affinity‑purified monoclonal antibody: minimise freeze‑thaw cycles, centrifuge before opening, and aliquot if the full volume will not be consumed within a few uses. The product is for research use only and is not intended for diagnostic or therapeutic applications.
Six peer‑reviewed publications currently cite ABM0010. The number is smaller than some loading‑control antibodies, but the contexts are informative: a lymphoma laboratory publishing in Blood and a neurodegeneration laboratory publishing in Acta Neuropathologica represent two research domains where Bcl‑2 quantification is not an optional supporting experiment but the primary biochemical readout that determines whether a mechanism is correctly assigned. The technical blog further notes that CROs have adopted the antibody for high‑throughput screening of Bcl‑2‑targeted ADCs. Independent validation from laboratories operating under the pressures of peer review—particularly in journals that specialise in haematopathology and neuropathology, where IHC quality is a prerequisite for publication—provides a level of real‑world performance evidence that no manufacturer’s certificate of analysis can replicate.
The broader biomedical context makes the case for a high‑specificity, cross‑reactivity‑free Bcl‑2 antibody increasingly difficult to ignore. Venetoclax is now standard‑of‑care in first‑line AML and relapsed CLL, and Bcl‑2 expression levels are being evaluated as predictive biomarkers in multiple clinical trials combining BH3‑mimetics with FLT3 inhibitors, CD47‑targeting agents, and immunomodulatory drugs. In solid tumours, Bcl‑2 overexpression mediates chemoresistance in breast, prostate, and small‑cell lung cancers, and efforts to extend BH3‑mimetic therapy beyond hematologic malignancies depend on the ability to quantify Bcl‑2 accurately in FFPE biopsy specimens that are often small, heterogeneous, and subjected to variable fixation conditions. A 2023 review in the Egyptian Journal of Medical Human Genetics highlighted emerging biomarkers and potential therapeutics of the Bcl‑2 protein family, noting that targeting these proteins may positively impact treatment of underserved medical problems. In neurodegeneration, Bcl‑2’s neuroprotective function is under investigation in Alzheimer’s, Parkinson’s, and Huntington’s disease models, and the ability to quantify Bcl‑2 in surviving neurons relative to degenerating neurons in post‑mortem human tissue requires an IHC‑validated antibody whose signal is not eroded by cross‑reactivity or epitope masking.
The monoclonal antibody that binds amino acids 41–54 of human Bcl‑2 with zero cross‑reactivity to Bcl‑xL, Mcl‑1, and Bcl‑w—that generates a single clean band at 26 kDa on western blots of HeLa lysate at 1:1000 dilution, that stains the mantle zone of human tonsil with membrane‑delimited crispness at 1:200, that achieves a 0.1 ng/mL detection limit and a sub‑3 % inter‑assay CV, that works in human, mouse, and rat tissue across western blot, IHC‑P, immunofluorescence, and ELISA, that ships at 0.73 mg/mL in a glycerol‑based cryoprotectant formulation stable for one year at –20 °C, and that has been independently validated in lymphoma and neurodegeneration studies published in Blood and Acta Neuropathologica—that antibody is catalog number ABM0010, priced for the academic laboratory and validated for the translational researcher.
Explore specifications, view representative images, and place your order here: https://www.abbkine.com/product/bcl-2-monoclonal-antibody-abm0010/





