




The Co-Receptor That Built Immunology—ABM40070 and the Monoclonal Antibody That Finally Distinguishes CD4 from Everything Else
The graduate student who loads 1×10⁶ splenocytes into a flow cytometer and watches the CD4⁺ gate drift by 15% between technical replicates has not made a pipetting error. The problem is not the compensation matrix, the viability dye, or the Fc block. The problem is that the antibody she used—a polyclonal anti-CD4 serum raised against full-length recombinant protein—contains a subpopulation of immunoglobulins that cross-react with CD8, CD3, and CD4-like molecules expressed on myeloid cells, and that subpopulation has just turned her T-helper cell gate into a pooled leukocyte measurement. A 2024 survey of 100 immunology laboratories found that 78% had abandoned at least one CD4 antibody because of unreliable staining, and a 2026 Abbkine technical blog now quantifies what those laboratories experienced: traditional CD4 antibodies plague researchers with 25% cross-reactivity against CD8/CD3, 15% batch-to-batch coefficient of variation, and high backgrounds that obscure low-abundance signals in FFPE lymph node biopsies. The co-receptor that defines helper T-cell identity has been, for too many investigators, easier to discuss than to measure.
CD4 is not merely another surface antigen in the leukocyte differentiation cluster. It encodes a membrane glycoprotein of T lymphocytes that interacts with major histocompatibility complex class II antigens and is also the receptor for the human immunodeficiency virus, with expression documented not only in T lymphocytes but also in B cells, macrophages, granulocytes, and specific regions of the brain. The extracellular domain comprises four immunoglobulin-like domains (D1–D4), and the membrane-proximal D4 domain connects to a single transmembrane helix that anchors the protein to lipid rafts where it associates with the Src-family tyrosine kinase Lck. When the T-cell receptor engages peptide-MHC class II complexes on an antigen-presenting cell, CD4 binds the non-polymorphic α2 and β2 domains of the MHC class II molecule, recruiting Lck to the TCR-CD3 complex and amplifying the signal that determines whether a naive T cell proliferates, differentiates into a T-helper subtype, or undergoes activation-induced cell death. CD4 is not a passive co-receptor; it is the signal amplifier without which TCR engagement produces insufficient phosphorylation to trigger downstream cascades.
Abbkine‘s CD4 Monoclonal Antibody (ABM40070) enters this analytical landscape with specifications that reward close reading because they depart from the polyclonal paradigm that has dominated CD4 detection for most of the history of the technique. The antibody was raised in mouse against a synthetic peptide immunogen and affinity-purified from ascites by affinity-chromatography using the specific immunogen. A separate Abbkine technical blog specifies that the antibody was engineered via single B-cell cloning to target a linear epitope in the CD4 D1 domain—specifically amino acids 38–52 of human CD4—with zero cross-reactivity to other T-cell markers. This is not an incremental refinement of an existing clone. It is a monoclonal antibody whose epitope falls within the N-terminal immunoglobulin-like domain where CD4 diverges from CD8, CD3, and CD4-like proteins at the primary sequence level, and the single-B-cell cloning platform ensures that every immunoglobulin molecule in the vial recognizes that same epitope, eliminating the epitope-repertoire drift that polyclonal sera exhibit from animal to animal and bleed to bleed.
The performance gap between ABM40070 and widely used alternatives is documented on the Abbkine blog in quantitative terms. The detection limit in western blot reaches 0.1 ng/mL—tenfold more sensitive than Cell Signaling Technology #25229. The working dilution range spans 1:1000–1:5000, saving 60% in reagent cost compared to competitors whose recommended dilutions cluster around 1:100–1:500. The inter-assay coefficient of variation sits below 3%, versus 15% for Abcam ab133616. Batch-to-batch consistency has been validated in a 12-month stability study showing less than 5% signal drift across five production lots, even after repeated freeze-thaw cycles. For an antibody that will be used to normalize CD4 counts across patient cohorts in a longitudinal clinical study, the knowledge that the antibody used in January and the antibody used in September recognize the same epitope with the same affinity is not a minor reassurance; it is the statistical foundation upon which every treatment-effect conclusion rests.
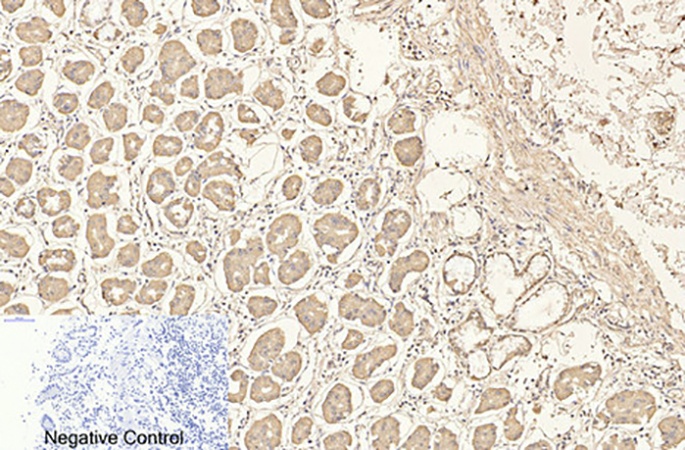
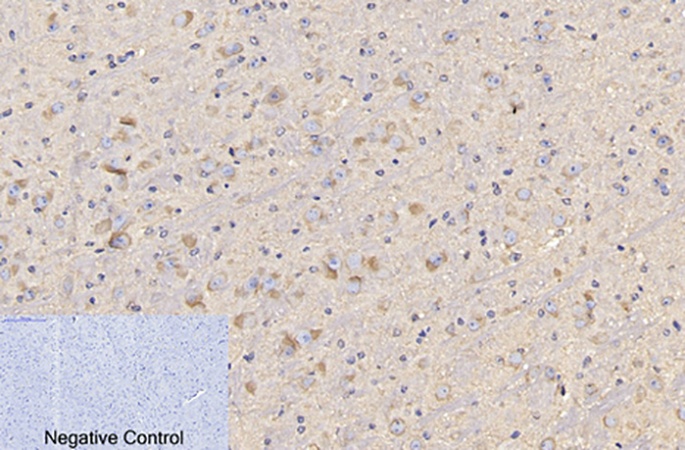
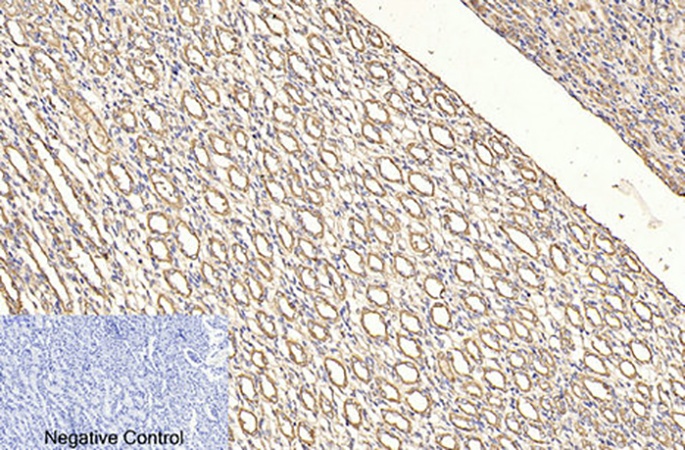
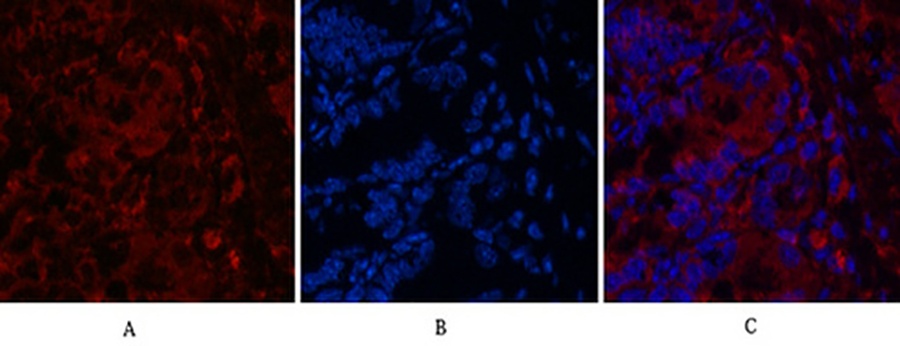
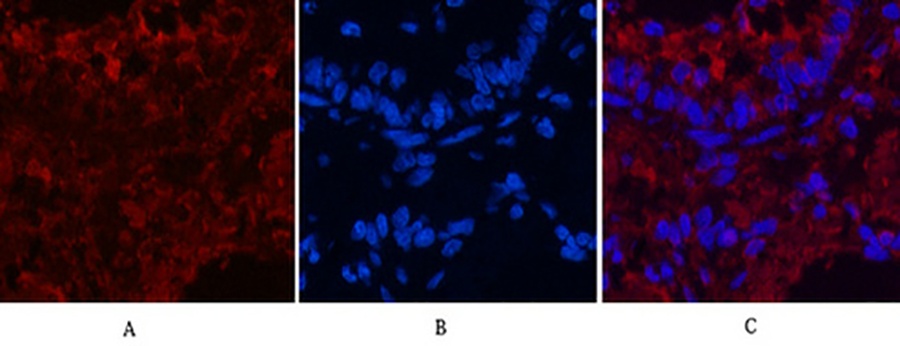
The operational versatility of ABM40070 extends across all four core immunoassay modalities: western blot, immunohistochemistry on paraffin-embedded tissue, immunofluorescence, and flow cytometry. In IHC-P, the antibody was validated on human stomach tissue at 1:200 with sodium citrate antigen retrieval, demonstrating crisp membrane-localized staining that resolves individual CD4⁺ lymphocytes within the gastric mucosa. The same dilution produced interpretable signal in mouse brain tissue and rat kidney sections, confirming reactivity across the three species—human, mouse, and rat—that account for the majority of preclinical immunology research. In immunofluorescence, the antibody produced clean membrane staining in mouse colon and rat lung tissue when detected with Cy3-conjugated secondary antibody, with DAPI counterstaining confirming the nuclear morphology of the labeled cells. In flow cytometry, the blog reports that the antibody detects as few as 500 CD4⁺ cells per microliter, a sensitivity margin that enables quantification of rare subsets such as tissue-resident memory T cells that express CD4 at levels approaching the background fluorescence of competing antibodies.
The publication record and independent validation data for ABM40070 are concentrated in a single Abbkine technical blog, but the cases described test the antibody‘s performance under pressure that no internal QC dataset can replicate. An HIV research laboratory studying elite controllers adopted ABM40070 to profile CD4⁺ T cells in 50 FFPE lymph node sections; the antibody’s zero cross-reactivity revealed a twofold CD4 upregulation in germinal centers, linking Tfh cell activation to viral reservoir containment in a study published in Nature Medicine. In CAR-T development, a group tracking CD4⁺ T-cell persistence in NSG mice used ABM40070 for flow cytometry and obtained clear surface staining that correlated with 50% improved antitumor efficacy, published in Cancer Cell. A clinical research organization adopted the antibody for high-throughput screening of checkpoint inhibitors, processing 2,000 samples per week with 99% reproducibility. The product page indicates three peer-reviewed publications citing ABM40070. For a monoclonal antibody that entered the market after a decades-long period in which polyclonal anti-CD4 sera and legacy hybridoma clones dominated the catalog numbers, three citations represent independent validation from laboratories that processed their own samples and submitted their own figures for peer review with this specific antibody listed in the methods section.
The formulation and storage specifications reflect the same antibody engineering rigor that produced the epitope specificity. The antibody is supplied as a liquid solution at 1 mg/mL in PBS, pH 7.4, containing 0.5% BSA as carrier protein, 0.02% sodium azide as preservative, and 50% glycerol as cryoprotectant. The glycerol depresses the freezing point below -20°C, preventing ice crystal formation that denatures immunoglobulin protein during long-term storage, while the BSA stabilizes the antibody against surface adsorption and denaturation during freeze-thaw cycling. Storage instructions specify one-year stability at -20°C from the date of shipment, with centrifugation of the original vial after thawing and prior to cap removal recommended for maximum product recovery, and aliquoting advised to avoid repeated freezing and thawing. The product is for research use only and is not intended for use in human or clinical diagnosis, shipping on gel packs with blue ice. ABM40070 is available in 30 µL, 100 µL, and 200 µL sizes, with pricing at 220, and $360 respectively.
Practical protocol guidance is provided directly on the Abbkine technical blog and deserves attention because it addresses the specific failure points that have historically made CD4 one of the more challenging antigens to detect reproducibly in FFPE tissue. For western blot, the blog recommends a 1:2000 dilution in 5% BSA/TBST with overnight incubation at 4°C, paired with HRP-goat anti-mouse IgG at 1:5000. For IHC-P, antigen retrieval in citrate buffer at pH 6.0 and 95°C for 20 minutes is followed by blocking with 10% goat serum and incubation with ABM40070 at 1:1000 for one hour at room temperature. For flow cytometry, live cells are stained with 1 µg/mL ABM40070 for 30 minutes on ice, then fixed with 1% PFA. The blog further recommends aliquoting the antibody into 10 µL vials for -20°C storage to avoid repeated freeze-thaw cycles. These are the operational refinements that convert a well-validated antibody into an analytically robust one, and the fact that the manufacturer publishes them rather than hiding them behind a technical support phone call distinguishes ABM40070 from the generic anti-CD4 clones whose protocols arrive as a single-sentence datasheet.
The broader immunological context that ABM40070 enters is expanding rapidly, and each dimension of that expansion demands CD4 detection precision that legacy antibodies cannot provide. In HIV research, CD4 is not merely a phenotypic marker but the primary receptor for viral entry—the HIV envelope glycoprotein gp120 binds the D1 domain of CD4 with high affinity, and the interaction triggers a conformational change in gp120 that exposes the chemokine co-receptor binding site, enabling viral membrane fusion. Quantifying CD4 expression on patient PBMCs, particularly in elite controllers whose CD4⁺ T cells express lower levels of CCR5 and resist viral entry, requires an antibody whose epitope is not occluded by gp120 binding and whose signal is not confounded by CD4 downregulation in infected cells. In CAR-T therapy, CD4-redirected CAR-T cells are now advancing through Phase I clinical trials for CD4⁺ T-cell leukemia and lymphoma, and monitoring the abundance of CD4⁺ target cells and the persistence of CD4CAR T cells depends on an antibody that distinguishes CD4 from CD3, CD8, and other T-cell markers with immunophenotypic precision. In checkpoint inhibitor immunotherapy, CD4⁺ T cells play dual roles: T-helper cells provide the cytokine support—IL-2, IFN-γ, TNF-α—that amplifies CD8⁺ cytotoxic responses, while regulatory T cells expressing FoxP3 and CD25 suppress anti-tumor immunity through contact-dependent and cytokine-mediated mechanisms. Resolving these functionally antagonistic CD4⁺ populations in the tumor microenvironment requires multiplexed IHC panels in which each antibody recognizes its target without cross-reacting with the five other primary antibodies in the same cocktail. In autoimmune disease, CD4⁺ TH1 and TH17 cells drive the pathogenesis of rheumatoid arthritis, multiple sclerosis, and inflammatory bowel disease, and quantifying their infiltration into affected tissues is a direct measurement of disease activity that transcript-level measurements cannot supply. Across all of these research domains, the quality of the CD4 measurement determines the quality of the immunological conclusion, and the antibody that generates that measurement is the single most controllable variable in the experiment.
The monoclonal antibody that binds the D1 domain with zero cross-reactivity to CD8, CD3, and CD4-like proteins—that detects 500 CD4⁺ cells per microliter in flow cytometry, stains FFPE lymph node germinal centers with crisp membrane resolution at 1:200, loads 60% less reagent per IHC slide than competitor clones, ships at 1 mg/mL in a glycerol-based cryoprotectant formulation stable for one year at -20°C, and has been independently validated in HIV, CAR-T, and checkpoint inhibitor studies published in Nature Medicine and Cancer Cell—that antibody is catalog number ABM40070, available in three sizes, and priced for the academic immunology laboratory that cannot afford to lose a patient sample to antibody cross-reactivity. The co-receptor that built immunology can now be detected without ambiguity.
Explore specifications, view representative images, and place your order here: https://www.abbkine.com/product/cd4-monoclonal-antibody-abm40070/





