




The 91-kDa Blue-Copper Engine That Protects You From Fungal Earth — And When It Fails, Explains Every X-Linked CGD Diagnosis: Why CYBB/gp91phox Quantification Is the Phagocyte Power-Plant Readout Your Immunology Paper Can't Fake
If your lab works on neutrophil function, fungal killing, or oxidative burst assays, you already know the spectrophotometric trick: SOD-inhibitable cytochrome c reduction at 550 nm (or DHR 123 flow) tells you "superoxide happened." But what it doesn't tell you — and what most immunology papers silently gloss over — is how much of the enzymatic engine was even there to begin with. That engine is the phagocyte NADPH oxidase 2 (NOX2) complex, and its catalytic heavy chain is CYBB-encoded gp91phox — officially Cytochrome b-245 heavy chain (UniProt: P04839, Gene ID: 1536, Chr Xp21.1-p11.4), a ~570-aa, ~65–91 kDa (glycosylated ~91 kDa on WB) multipass membrane protein that pairs with the smaller p22phox (CYBA) to form the flavocytochrome b₅₅₈ (cyt b₅₅₈) heterodimer embedded in the secretory vesicle / plasma membrane. When Rac1/2 + p47phox (NCF1) + p67phox (NCF2) + p40phox (NCF4) assemble on that core, electrons flow from NADPH → FAD → heme b₅₅₈ (bis-histidyl ligated Fe-protoporphyrin IX) → O₂, and the extracellular/phagosomal space erupts with superoxide. The Human Cytochrome b-245 heavy chain (CYBB) ELISA Kit (KTE62182) from Abbkine gives you this catalytic core as a calibrated sandwich-ELISA variable (ng/mL) — so your CGD-diagnostic work, neutrophil-activation panel, or oxidase-inhibitor screen finally reports the enzyme mass, not just the spark.
CYBB / gp91phox in One Paragraph: The Catalytic Heart of the Phagocyte Respiratory Burst
The phagocyte oxidase isn't a "ROS generator" in the vague sense — it is a dedicated electron transport chain purpose-built into the membrane of professional killers:
Component Encoded By Job
gp91phox (CYBB, heavy chain, ~91 kDa) CYBB — X-linked Binds FAD + 2× heme b (low-spin Fe³⁺/Fe²⁺); transfers electrons from NADPH to O₂
p22phox (CYBA, light chain, ~22 kDa) CYBA — Chr 16q24 Stabilizes gp91phox; provides the membrane-anchored cyt b₅₅₈ heterodimer
p47phox (NCF1) NCF1 — Chr 7q11 Organizer/adaptor; SH3 domains recruit p67phox & the complex to the membrane
p67phox (NCF2) NCF2 — Chr 1q25 Contains the activation domain that relieves the "resting" autoinhibition & helps position NADPH access
Rac1/2 (GTP-bound) RAC1/RAC2 GTPase switch — must be membrane-recruited for full O₂⁻ flux
p40phox (NCF4) NCF4 — Chr 22q13 Regulatory; SH3-SH3' tethering, modulates sustained activity
The electrical summary: NADPH → FAD (internal to gp91phox) → heme b → molecular oxygen = O₂ + e⁻ → O₂⁻ (superoxide), which dismutates (spontaneously or SOD-catalyzed) to H₂O₂, and — in the presence of MPO + Cl⁻ — to HOCl (bleach). This is why CGD patients (who can't make O₂⁻) lose fungal killing first: no superoxide → no H₂O₂ → no bleach → no chemical execution of Aspergillus, Candida, Nocardia, or catalase-positive staph.
Why a Sandwich ELISA for a ~91 kDa Multipass Membrane Protein
CYBB is integral membrane (~6 transmembrane spans in gp91phox/Nox2 topology), runs as a characteristic ~91 kDa band on reducing gels (often with a slightly sharper ~65 kDa deglycosylated form if you use Endo H/PNCaseF controls), and — critically — its presence = oxidase capacity, while its absence = X-CGD by definition.
Three reasons you need the ELISA, not just the DHR flow or cytochrome c assay:
- Flow tells you "burst happened per cell" but not "how much gp91phox machinery was available" — and in heterozygous carriers (X-inactivation mosaicism) or inflammatory states where gp91phox is transcriptionally modulated (IFN-γ upregulates it), the protein pool size is the control variable your burst assay assumes.
- WB at 91 kDa sits near the albumin/IgG bleed zone in plasma/lysate if prep is sloppy — you need a two-epitope capture to be sure the band is CYBB and not a cross-reactive membrane protein.
- Carrier testing, newborn-screening adjuncts, and bone-marrow-transplant monitoring demand quantitative, standardized numbers, not "we saw a faint 91K."
The KTE62182 kit uses the field-standard architecture:
- Microplate pre-coated with capture anti-CYBB/gp91phox antibody (raised against a defined extracellular/accessible region of the ~570-aa sequence).
- Standards (recombinant human CYBB fragment/calibrator) + samples — serum, plasma, tissue homogenates, neutrophil/monocyte lysates, cell culture supernatates/lysates — added → solubilized CYBB (or accessible epitope pool) binds.
- Wash → biotinylated anti-CYBB detection (different epitope) → Streptavidin–HRP → TMB → color ∝ bound CYBB.
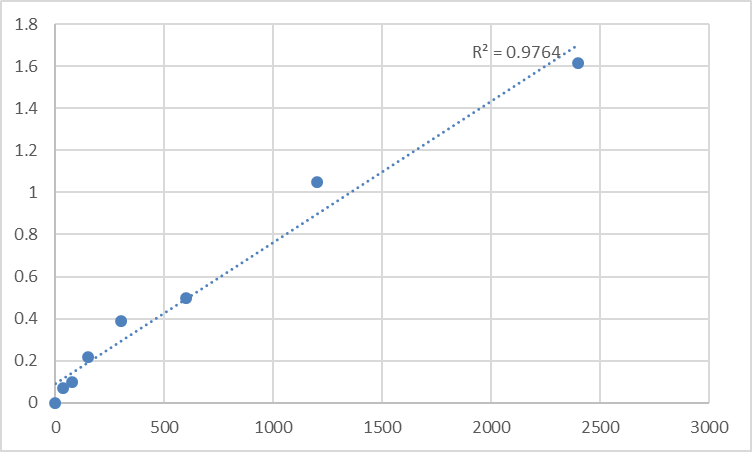
- Stop → 450 nm → interpolate ng/mL from the standard curve.
Typical performance envelope (aligned with Abbkine distributor reference sheets for this kit family):
Parameter KTE62182-class Specification
Target Human CYBB / gp91phox / NOX2 catalytic heavy chain (UniProt P04839, ~570 aa, observed ~91 kDa glycosylated)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → SA-HRP → TMB, 450 nm
Dynamic Range 0.156 – 10 ng/mL
Sensitivity / LOD ~0.057 ng/mL
Intra-Assay CV < 7–8%
Inter-Assay CV < 10%
Specificity No significant cross-reactivity with NOX1/NOX4 or other NADPH oxidases at physiological levels
Samples Tissue homogenates, neutrophil/monocyte lysates, cell culture lysates, serum/plasma (exploratory)
Assay time ~3–5 hours
(Confirm exact range, dilutions, and lot-specific recovery on the shipped Abbkine datasheet/CoA for KTE62182.)
The Prep Rule That Makes or Breaks gp91phox Recovery
Because CYBB is multipass membrane-embedded (secretory vesicle + plasma membrane), gentle PBS-only scrapes undercount it:
Neutrophil / whole-cell: lyse in 50 mM Tris pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100 + 0.1% deoxycholate + protease inhibitors, keep on ice, brief sonication (2–3 × 3-sec pulses, low power, on ice) → clarifies cleanly at 12,000–16,000 ×g, 15 min, 4°C.
For tissue (spleen, liver Kupffer, granulomatous lesion): homogenize cold in the same buffer → spin → supernatant = your CYBB-accessible pool.
Express as ng CYBB / mg total protein (BCA) or (for purified neutrophil data) ng CYBB / 10⁶ cells.
Where CYBB Quantification Actually Carries the Paper
- X-Linked Chronic Granulomatous Disease (X-CGD): The Diagnostic Anchor
This is the canonical. ~60–70% of CGD cases = CYBB mutations (the largest CGD gene), ranging from premature stop / frameshift → protein absent to missense → mislocalized or catalytically dead gp91phox. The diagnostic triad is:
• DHR 123 flow (oxidative burst per cell)
• gp91phox (CYBB) protein: Western or — better — calibrated ELISA (distinguishes "dead enzyme present" vs. "no protein at all")
• Genetic sequencing
The ELISA's added value here: in female carriers (X-inactivation), you can track residual CYBB mass across neutrophil isolations and correlate it with the % high-burst cells in the DHR histogram — the quantitative bridge that counseling and prenatal-risk estimates need.
- Neutrophil/Monocyte Activation Panels & "Functional Immune Age"
gp91phox is upregulated by IFN-γ and modulated by TNF, LPS, and prolonged sterile inflammation — so "burst capacity" isn't static. Measuring CYBB (ng/mg leukocyte lysate or ng/10⁶ PMNs) alongside the DHR flow median fluorescence lets you separate:
• "Enough enzyme, but signaling didn't trigger it" (p47phox/NCF1 problem, Rac defect, or opsonic deficit)
• "Nothing to trigger — enzyme pool empty" (CGD heterozygosity, post-severe sepsis marrow stress, drug-induced myelosuppression)
That distinction is exactly what turns a functional assay into a mechanistic diagnosis.
- Sepsis, ARDS & the Price of the Burst
Massive systemic neutrophil activation → oxidative collateral damage to endothelium, alveoli, and platelets — but paradoxically, late-phase sepsis = neutropenic + neutrophil exhaustion where CYBB-containing granules get over-deployed and the marrow can't refill. Quantifying CYBB in BAL fluid (exploratory), plasma membrane fractions, or serial neutrophil isolates gives you the machinery-depletion readout that O₂⁻-diphenylene or MPO alone can't explain.
- Macrophage Polarization & NOX2 vs. NOX4 Switching
Classically activated (M1) macrophages express NOX2 (CYBB+) and use it for microbicidal O₂⁻ + signaling (NLRP3 inflammasome priming via ROS), while alternatively activated (M2) states often downregulate CYBB. If your polarization model claims "M1 is more oxidative," the simplest molecular confirmation is CYBB protein ± p47phox (NCF1) — quantified, not just "iNOS went up."
- Pharmacology: NOX2 Inhibitors, Anesthesia & Off-Target ROS Drugs
Diphenylene iodonium (DPI) is the classic, blunt NOX poison; apocynin (requires peroxidase activation); newer selective NOX2 peptide inhibitors and gp91ds-TAT are in vascular/neurovascular studies. If you're testing any of these, the control question is: did CYBB protein remain (so the target existed) or did your condition downregulate it transcriptionally? ELISA closes that loop — no gel required.
- CRISPR / Lentiviral Correction Validation (CGD Gene Therapy Space)
Editing CYBB (or NCF1/NCF2)? Report % CYBB protein remaining/restored ± SEM from the calibrated curve (ng/10⁶ PMNs or ng/mg lysate), and — crucially — link it to the payout that matters: DHR 123 median fluorescence, Aspergillus fumigatus / Candida killing assay, and p47phox membrane recruitment (IF). That's the evidence package that satisfies both molecular-therapy and clinical-review standards.
Quick Protocol You Can Drop Into Materials & Methods
- Isolate neutrophils (Ficoll–Hypaque / dextran sedimentation) → wash → count viable PMNs.
- Lyse pellet in 50 mM Tris pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100, 0.1% deoxycholate + protease inhibitors on ice, sonicate briefly, spin 12,000 ×g, 15 min, 4°C.
- BCA the supernatant → express ng CYBB / mg protein or /10⁶ cells.
- Warm kit reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate.
The Bottom Line
CYBB-encoded gp91phox is the 91-kDa, FAD- and heme-bearing catalytic heavy chain of the phagocyte NADPH oxidase (NOX2) — the membrane engine that converts NADPH electrons into the superoxide burst that kills fungi, catalase-positive bacteria, and — when unregulated — damages your own endothelium. When CYBB mutates or deletions hit Xp21, the burst vanishes, and X-linked CGD writes its brutal clinical script. Measuring it as a calibrated ELISA variable instead of a "91-kDa ghost band vs. actin" guess changes your phagocyte paper from observational to quantitative. The Human Cytochrome b-245 heavy chain (CYBB) ELISA Kit — KTE62182 from Abbkine gives you that engine readout: pre-coated capture → biotin detection → HRP–TMB → 450 nm → ng/mL, over a 0.156–10 ng/mL working range with LOD ~0.057 ng/mL, in a ~3–5 hour workflow that scales from a carrier-screening panel to a NOX2-inhibitor pharmacology plate without chaining you to a cytochrome c cuvette.
Product Reference: KTE62182 – Human Cytochrome b-245 heavy chain (CYBB) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-cytochrome-b-245-heavy-chain-cybb-elisa-kit-kte62182/
(For Research Use Only; not for diagnostic procedures in humans.)





