




The 200-kDa "Safe" That Controls Where TGF-β Can — And Can't — Strike: Why Quantifying LTBP3 Changes How You Read Fibrosis, Bone Remodeling, and Early Metastasis
If your entire TGF-β section rests on one phospho-SMAD2/3 Western and a "TGF-β1 ELISA" from conditioned media, you're measuring the smoke while ignoring the scaffold that decides whether the fire is locked in the wall or free to burn the neighborhood. LTBP3 (Latent-transforming growth factor beta-binding protein 3, UniProt: Q9NS15, Gene ID: 4054, Chr 19p13.2) is the ~190–240 kDa heavily O-glycosylated ECM glycoprotein that forms the structural backbone of the Large Latent Complex (LLC = LTBP3 + LAP–TGF-β dimer), tethers it to fibrillin-1 microfibrils in the extracellular matrix, and — crucially — controls the local bioavailability of TGF-β1 and TGF-β3 until a protease (plasmin, MMP-2/MMP-14, cathepsin G) or an integrin (αvβ6, αvβ3, αvβ5) physically pulls LAP away and frees the cytokine. The Human Latent-transforming growth factor beta-binding protein 3 (LTBP3) ELISA Kit (KTE61770) from Abbkine is the reagent that finally gives this ECM anchor a quantitative plate-readable identity — sandwich ELISA → ng/mL — so your fibrosis, bone-development, or tumor-desmoplasia story stops waving at "TGF-β went up" and starts explaining where TGF-β was allowed to be.
LTBP3 in One Paragraph: The Structural Half of "Latent"
The phrase latent TGF-β is precise: cells secrete mature TGF-β non-covalently trapped inside its own propeptide dimer (LAP = latency-associated peptide), and this Small Latent Complex (SLC) is useless to a receptor — until something mechanically or proteolytically opens it. LTBPs are the reason SLC doesn't just float away:
Complex Composition Where It Lives
SLC LAP dimer : TGF-β dimer (non-covalent, ~80–100 kDa) Would diffuse if unanchored
LLC LTBP3—S—S—SLC (disulfide-linked tripartite) Tethered to ECM via fibrillin-1/2 microfibrils
LTBP3's modular body — signal peptide → unique N-terminal region → alternating cbEGF (calcium-binding EGF-like) repeats + 8-Cys/TB (8-cysteine / TGF-β binding) domains → C-terminal fibrillin-like tail — is basically a multi-domain docking strip that:
- Binds SLC via a specific TB-domain disulfide (locking TGF-β inactive),
- Binds fibrillin-1 via its C-terminal region (parking it in the matrix), and
- Becomes the substrate that proteases/integrins must address before TGF-β is released.
The biological punchline is simple: no LTBP3 tether → no local TGF-β reservoir → either TGF-β leaks freely (bad, if it shouldn't) or the cell can't store/position it for correct activation (bad, if it should).
Why a Sandwich ELISA for a ~200 kDa ECM Glycoprotein — And Why "TGF-β ELISA Alone" Is an Incomplete Claim
TGF-β is ~25 kDa, secreted, and diffusible — so its concentration tells you how much cytokine is loose in the sample.
LTBP3 is ~200 kDa, heavily glycosylated, and ECM-tethered — its concentration tells you how much latent reservoir the tissue built, how densely it's parked in microfibrils, and whether the matrix is even equipped to run an integrin-dependent activation cycle.
Three practical reasons your experiment needs LTBP3 quantified:
- TGF-β and LTBP3 diverge under stress: TGF-β can rise (release from LLC) while LTBP3 simultaneously drops (proteolytic shedding/cleavage of the C-terminal fibrillin anchor). That means [TGF-β] ≠ [LTBP3], and interpreting one without the other creates false causal stories.
- LTBP3 is not a housekeeper: it's developmentally regulated (bone, dentin, cranial sutures, lung alveolarization) and dynamically remodeled in fibrosis, cancer desmoplasia, and periodontal disease — so "it's there" isn't a number.
- Gel-band quantification at ~200 kDa (where glycosylation smears) gives you a smear, not a CV-friendly standard curve.
The KTE61770 kit uses the proven architecture:
- Microplate pre-coated with capture anti-LTBP3.
- Standards (recombinant/calibrator LTBP3) + samples — serum/plasma (exploratory, since most LTBP3 is ECM-tethered), tissue homogenates, cell lysates/solubilized ECM, culture supernatants — added → LTBP3 (or soluble LTBP3 fragments) binds.
- Wash → biotinylated anti-LTBP3 detection (different epitope) → Streptavidin–HRP → TMB → color ∝ bound LTBP3.
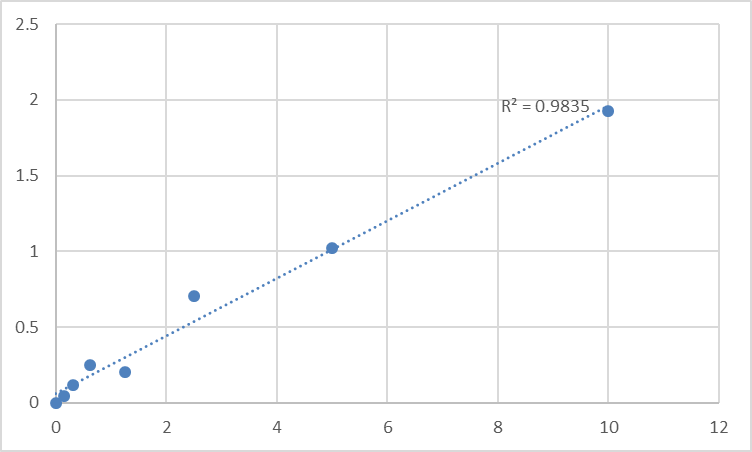
- Stop → 450 nm → interpolate ng/mL from the standard curve.
Consolidated specification envelope (matching distributor/technical data for this sandwich ELISA family):
Parameter KTE61770-class Specification
Target Human LTBP3 / LTBP-3 (UniProt Q9NS15, ~1,399 aa computed; observed ~190–240 kDa due to glycosylation)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → SA-HRP → TMB, 450 nm
Dynamic Range 0.156 – 10 ng/mL
Sensitivity / LOD ~0.06–0.07 ng/mL
Intra-Assay CV < 6–8%
Inter-Assay CV < 10%
Specificity No significant cross-reactivity with LTBP1/LTBP2/LTBP4 at physiological levels
Samples Serum/plasma (exploratory), tissue homogenates, ECM-enriched fractions, cell lysates, culture supernatants
Assay time ~3–5 hours
(Confirm exact dilutions and lot-specific recovery on the shipped Abbkine datasheet for KTE61770.)
The Prep Angle That Decides Whether You're Measuring Air or Matrix
Because LTBP3 is ECM-tethered via fibrillin microfibrils, the single most common mistake is under-solubilizing it:
For tissue (bone, gum/periodontal ligament, skin, lung, tumor stroma):
Homogenize cold in 50 mM Tris pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100 + protease inhibitors, spin out nuclei/debris, then re-extract the high-speed pellet (the ECM-rich residue) in 2% SDS or 4 M urea + 0.5% Triton if you want the true ECM-tethered pool.
For routine work, a deoxycholate/Triton sequential or RIPA + brief sonication on ice already pulls a large fraction of LTBP3 into the soluble readout.
Express as ng LTBP3 / mg total protein (BCA) or (for bone/ligament) as ng LTBP3 / µg collagen hydroxyproline for a true matrix-density normalization.
Where LTBP3 Quantification Actually Carries the Paper
- Cancer Desmoplasia & the "Upstream" Metastasis Gate
The Scripps Research/Quigley/Rifkin axis showed the cleanest cancer fact of the decade: LTBP3 is required for early metastatic angiogenesis in head and neck carcinoma, and high LTBP3 = poor survival. The mechanism is indirect but devastating: LTBP3 packages and presents latent TGF-β in the ECM where αv-integrins (αvβ6 especially) physically pull LAP off, releasing active TGF-β that induces VEGF/angiogenesis programs and creates the defined-size, defined-permeability vessels tumor cells need to intravasate. Knock LTBP3 out → tumors can't build those vessels → metastasis collapses.
Quantifying LTBP3 in tumor-lysate / stromal homogenates (ng/mg, normalized to fibrillin-1 or collagen I) alongside active TGF-β (sandwich ELISA), p-SMAD2/3, CD31 MVD, and VEGF is the mechanistic hinge that moves the claim from "angiogenesis happened" to "the scaffold enabled it."
- Bone Development, Cranial Sutures & Tooth Agenesis
This is where LTBP3 earned its genetic stripes. LTBP3-/- mice are >50% smaller, show cranial base cartilage-bone defects, thoracic kyphosis, osteopetrosis-like bone sclerosis (from reduced TGF-β bioavailability at resorption fronts), and — strikingly — oligodontia / missing posterior teeth because dental follicle/periodontal ligament development depends on correctly positioned TGF-β via LTBP3. Human correlates (studied in smaller cohorts) link LTBP3 pathway variants to dental agenesis and craniofacial growth disorders. Measuring LTBP3 in calvarial/long-bone lysates or gingival tissue gives you the ECM-reservoir variable that x-ray micro-CT can't see.
- Pulmonary Fibrosis & Elastin/Alveolarization
LTBP3 localizes to elastic fiber microfibrils (fibrillin-1 rich) in lung interstitium; its proteolytic cleavage or altered deposition parallels alveolar wall destruction, EMT, and TGF-β-driven fibroproliferative remodeling in IPF models. Tissue homogenates + trichrome + LTBP3 (ELISA) + α-SMA builds a structural narrative: not "fibrosis marker X went up," but "the microfibril scaffold that gates TGF-β got remodeled."
- Periodontal Ligament, Cementum & Orthodontic Stress
PDL cells express LTBP3 as part of the mechanotransduction → TGF-β activation → cementoblast/osteoblast differentiation axis. Orthodontic loading, periodontal disease, and implant osseointegration all create localized compression/tension zones where LTBP3 deposition at the ligament–bone interface predicts whether the tissue remodels productively or fibrotically scars. ELISA-quantified LTBP3 (ng/mg) in gingival crevicular fluid or PDL homogenates is a far more specific readout than IL-1β alone.
- Atherosclerotic Media & Elastic Lamina Degeneration
Elastic lamina integrity depends on fibrillin microfibrils + LTBP-anchored latency complexes; as the lamina frays (aging, diabetes, Lp(a)), LTBP3 fragments and TGF-β dysregulation contributes to calcific medial sclerosis and plaque instability. LTBP3 ELISA on aortic-media scrapings (normalized to elastin/ fibrillin-1) is the ECM-quality-control readout that lipid histology can't quantify.
- CRISPR / AAV & TGF-β Bioavailability Screens
Editing LTBP3, FBN1, or ITGB6? Don't just show "TGF-β ELISA moved." Report % LTBP3 protein remaining ± SEM from the calibrated curve, and close the loop with:
• Active vs. latent TGF-β ratio (acid-ethanol separation or LAP:TGF-β duo ELISA)
• p-SMAD2/3 (nuclear IF or WB)
• Downstream: collagen I, α-SMA, CTGF
That triad proves you touched the reservoir, not just the smoke.
A Minimal Protocol You Can Paste Into Materials & Methods
- Tissue: cold 50 mM Tris pH 7.4, 150 mM NaCl, 0.5% Triton X-100 + protease inhibitors → homogenize → spin 800 ×g × 10 min (nuclei discard) → spin supernatant 100,000 ×g or min 40,000 ×g 20 min if you want a clean ECM-enriched supernatant, or just clarify at 12,000–16,000 ×g, 15 min, 4°C for routine work.
- Culture: lyse in same buffer + 0.5% deoxycholate optional for ECM push.
- BCA → ng LTBP3 / mg total protein.
- Warm kit reagents ≥ 30 min RT before opening; protect TMB; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve on every plate.
The Bottom Line
LTBP3 is the ~200 kDa, heavily glycosylated ECM scaffold that forms the physical lock on TGF-β's latency — tethering the cytokine to fibrillin-1 microfibrils, presenting it for integrin-dependent release, and deciding, centimeter by centimeter, where growth-factor signaling is allowed to happen. Measuring TGF-β without measuring LTBP3 is like counting fire trucks and pretending you know where the hydrants are. The Human Latent-transforming growth factor beta-binding protein 3 (LTBP3) ELISA Kit — KTE61770 from Abbkine gives you that hydrant map: pre-coated capture → biotin detection → HRP–TMB → 450 nm → ng/mL, over a 0.156–10 ng/mL working range with LOD ~0.06–0.07 ng/mL, in a ~3–5 hour workflow that scales from a bone-harvest homogenate to a 50-sample tumor-stroma cohort without a gel-stack detour.
Product Reference: KTE61770 – Human Latent-transforming growth factor beta-binding protein 3 (LTBP3) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-latent-transforming-growth-factor-beta-binding-protein-3-ltbp3-elisa-kit-kte61770/
(For Research Use Only; not for diagnostic procedures in humans.)





