




The 170-kDa Gateway That Built a $200 Billion Targeted-Therapy Industry: Why Total EGFR Protein Mass — Not Just Phospho-Westerns or Mutation Reports — Is the Variable Your TKI/ADC Panel Is Missing
There's a reason three letters — EGFR — appear on more oncology drug labels than any other kinase gene: it is the original "undruggable-that-became-the-flagship" story of modern molecular oncology. Officially HER1 / ErbB-1 / c-ErbB-1 (UniProt: P00533, Gene ID: 1956, Chr 7p11.2), the Epidermal Growth Factor Receptor is a single-pass type I transmembrane receptor tyrosine kinase (~1210 aa, computed ~134 kDa, observed mature form ~170–180 kDa thanks to N-linked glycosylation and the large extracellular ligand-binding domain) that sits on the surface of virtually every epithelial cell waiting for its cue. That cue arrives as EGF, TGF-α, amphiregulin, betacellulin, or HB-EGF → the extracellular domains clamp shut → EGFR dimerizes (often EGFR:EGFR homodimer, or EGFR:ErbB2/HER2, EGFR:Her3 heterodimers) → the intracellular tyrosine kinase domains autophosphorylate in trans (key sites: Tyr¹⁰⁶⁸, Tyr¹¹⁴⁸, Tyr¹¹⁷³) → and suddenly RAS-RAF-MEK-ERK, PI3K-AKT-mTOR, and PLCγ-PKC are all online, dumping proliferation and survival signals into the nucleus. The Human Epidermal Growth Factor Receptor (EGFR) ELISA Kit (KTE62577) from Abbkine exists to measure the one thing your mutation-report or p-EGFR/Tyr¹⁰⁶⁸ Western assumes but never actually counts: total EGFR protein mass (ng/mL, interpolated from a recombinant standard curve) in your lysates, supernatants, or (carefully handled) plasma/tissue — so your TKI dose–response, resistance-mechanism, or patient-stratification story has the receptor-density denominator that decides whether the drug even has enough doorbells to ring.
EGFR in One Paragraph: The 170-kDa RTK That Invented the Era of "Block the Gate, Not the City"
EGFR belongs to the ErbB / HER family — four closely related RTKs (EGFR/HER1, HER2/ErbB2, HER3/ErbB3, HER4/ErbB4) whose dimerization combinatorics define modern targeted therapy. The architecture is iconic:
Domain Position (aa) Function
Extracellular ligand-binding domain (ECD) ~1–621 Four subdomains (I–IV); domains I/III are "open/closed" latch that traps ligand; domain II drives the dimerization arm (the "thumb" that hooks the partner's domain IV)
Transmembrane α-helix ~622–644 Anchors the receptor; rotates during activation to align intracellular kinase lobes
Intracellular tyrosine kinase domain ~645–940 Bilobate (N- and C-lobes) with the HRD motif (His-Arg-Asp) and DFG motif that every TKI (gefitinib/erlotinib/osimertinib) exploits — this is literally the gatekeeper pocket that launched the modern TKI era
C-terminal tail ~941–1210 Eight autophosphorylation tyrosines (Y992, Y1045, Y1068, Y1086, Y1148, Y1173…) → docking sites for Grb2/SOS (RAS), PI3K (p85), PLCγ, CBL (ubiquitin ligase)
The clinical bottom line: EGFR is overexpressed/amplified in ~60–80% of NSCLC (squamous), ~60%+ of HNSCC, ~70%+ of glioblastoma, and significant subsets of CRC, pancreatic, and TNBC — which is why the first-generation TKIs (gefitinib, erlotinib) and monoclonals (cetuximab, panitumumab) were built around it, and why the third-generation (osimertinib) now dominates EGFR T790M and exon 19 del NSCLC. But every one of those drugs faces the same pharmacokinetic reality: you can't inhibit a receptor that isn't there in sufficient mass, and you can't explain acquired resistance just by sequencing exon 20 without knowing whether EGFR protein was downregulated, internalized, or re-routed to the lysosome.
Why a Sandwich ELISA for a ~170-kDa Glycoprotein — And Why p-EGFR/actin Is an Incomplete Claim
EGFR is membrane-embedded, heavily N-glycosylated, and trafficking-obsessed (plasma membrane ↔ clathrin-coated pits ↔ early endosomes ↔ lysosome ↔ recycling), which means three practical headaches for gel-only work:
- Its ECD can shed (via ADAM17/TACE in a regulated fashion, especially under TGF-α/EGF stimulation or cetuximab pressure) → a fraction of "EGFR signal" ends up in the supernatant as soluble ECD (~110 kDa, still immunoreactive), while the membrane pool drops — so "whole-lysate band intensity vs. actin" conflates location, shedding, and total mass.
- The 170-kDa zone is busy (other RTKs, large adapters), and without two distinct anti-EGFR epitopes you're gambling on specificity.
- Drug screens and cohort panels (TKI dose–response, resistance clones, patient-derived organoid lysates) need plate numbers with CVs, not a 7.5% gel transfer.
The KTE62577 kit uses the field-standard two-site sandwich ELISA:
- Microplate pre-coated with capture anti-EGFR (raised against an accessible ECD/tail epitope that survives in both membrane and partially cleaved/shed forms, depending on the antibody design).
- Standards (recombinant human EGFR ECD or calibrated EGFR-calibrator) + samples — serum/plasma, tissue homogenates, cell lysates, cell culture supernatants/lysates, other biological fluids — added → EGFR (or shed ECD) binds.
- Wash → biotinylated anti-EGFR detection (different epitope) → Streptavidin–HRP → TMB → color ∝ bound EGFR.
- Stop → 450 nm → interpolate ng/mL from the standard curve.
From the distributor/technical sources aligned with this kit family:
Parameter KTE62577-class Specification
Target Human EGFR / HER1 / ErbB-1 (UniProt P00533, Gene 1956)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → SA-HRP → TMB, 450 nm
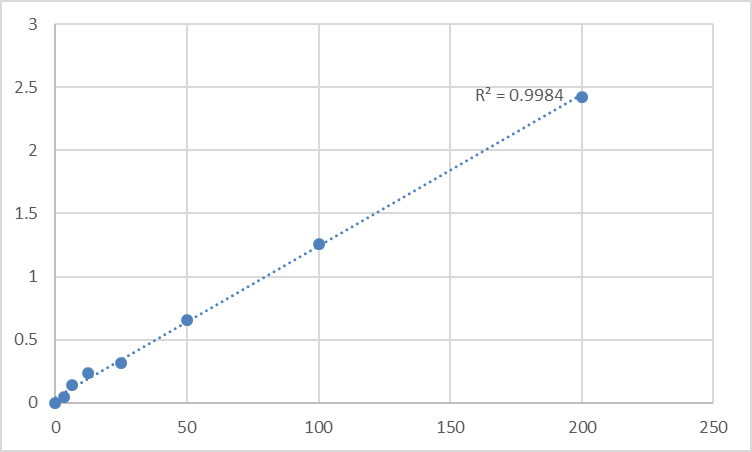
Dynamic Range 0.156 – 10 ng/mL (equivalent vendor variants also quote extended ranges up to 3.12–200 ng/mL depending on calibrator)
Sensitivity / LOD ~0.029–1.21 ng/mL (check lot CoA for your exact formulation)
Intra-Assay CV < 4–8%
Inter-Assay CV < 8–12%
Specificity No significant cross-reactivity with HER2/ErbB2, ErbB3, ErbB4 or other RTKs at physiological levels
Samples Serum, plasma (EDTA), tissue homogenates, cell lysates, culture supernatants
Assay time ~3–5 hours
(Always confirm exact range, dilution factors, and recovery on the shipped Abbkine datasheet/CoA for KTE62577.)
The Prep Rule That Decides Whether You're Measuring Receptor or Empty Plastic
Because EGFR is type I TM + heavily glycosylated + trafficking through endocytic compartments, lysate prep matters:
• For cultured cells: lyse in RIPA or 50 mM Tris pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100/NP-40 + protease inhibitors + 1 mM Na₃VO₄ + 10 mM NaF (keep phospho-reads honest if you run p-EGFR alongside), keep cold, brief sonication (2–3 × 3-sec pulses, low power, on ice) to release membrane-embedded receptor without shredding the ECD. Clarify 12,000–16,000 ×g, 15 min, 4°C.
• For tissue (lung, HNSCC, GBM, colon): homogenize cold in the same buffer; spin; use supernatant → BCA → express as ng EGFR / mg total protein.
• For exploratory plasma/serum: EDTA preferred; process cold/fast; note that the readout here mostly reflects soluble ECD (shed) rather than intact full-length membrane receptor — still valuable as a turnover/proteolysis proxy, but disclose it clearly.
Where Total EGFR Quantification Actually Carries the Paper
- NSCLC & the "Exon 19 del / L858R vs. Wild-Type" Interpretation
This is the flagship EGFR lane. The paradigm is: mutation → constitutive kinase activity → proliferation, so we give osimertinib / afatinib / gefitinib. But the inconvenient fact: EGFR protein can be wildly heterogeneous across tumor zones (intratumoral heterogeneity, clonal selection under TKI pressure), and acquired resistance often involves EGFR loss (downregulation, CBL-mediated ubiquitination, lysosomal diversion) or bypass activation (MET amp, HER2, RAS, BRAF fusions). Reporting total EGFR protein mass (ng/mg, ELISA) alongside:
• Mutation status (qPCR/NGS for exon 19 del, L858R, T790M, C797S)
• p-EGFR (Tyr¹⁰⁶⁸) or downstream p-ERK/p-AKT
• MET / HER2 / FGFR1b as bypass tracks
…that's the triad that moves the claim from "mutation was present" to "the receptor was present, phosphorylated, and then survived the drug."
- Cetuximab/Panitumumab Resistance in mCRC & HNSCC (The Shedding & Heterogeneity Axis)
Anti-EGFR mAbs depend on binding the ECD to block ligand, promote internalization, and trigger ADCC. Resistance shows up as:
• EGFR extracellular domain mutations (S492R, R451C) that prevent mAb binding while preserving ligand signaling
• Increased ADAM17-mediated shedding → sEGFR-ECD rises, mAb gets "decoyed" in the interstitial space
• HER2/HER3 heterodimer bypass
Quantifying total and (exploratorily) shed ECD by ELISA in baseline vs. post-treatment plasma/tissue is the mechanistic readout that "antibody didn't bind" alone can't prove.
- GBM & the EGFRvIII Chimera (The 145-kDa Deletion Variant)
A subpopulation of GBMs carry EGFRvIII — an in-frame deletion removing exons 2–7 of the ECD (→ ~145 kDa, lacks the ligand-binding cleft, constitutively active) — and it's the poster child for CAR-T and vaccine targets. While a wild-type EGFR ELISA (like KTE62577, which uses antibodies against conserved ECD/tail epitopes) will often detect both WT and vIII, the total receptor mass still matters: high EGFRvIII/WT density predicts which tumors are truly "EGFR-addicted" vs. which have already switched to PDGF/Met/FGFR bypass.
- Drug Screen / TKI Dose–Response & the Lysosomal Diversion Story
If you're testing gefitinib → osimertinib transition, or HSP90 inhibitors (ganetespib) that collapse EGFR folding, or CBL modulators, don't stop at "p-ERK went down." Report % EGFR protein remaining ± SEM from the calibrated curve (ng/mg), and tie it to:
• Surface EGFR vs. intracellular pool (MFI with anti-EGFR mAb, or IF/confocal)
• Downstream (p-ERK1/2, Cyclin D1, cleaved PARP)
That proves the TKI didn't just "turn off a kinase" — it altered the receptor's physical existence at the membrane.
- Tissue-Bank / TMA Correlative Studies
Paraffin-embedded lysates or high-quality frozen powder → ELISA-quantified EGFR (ng/mg, normalized to β-actin or total protein) lets you test for protein-level thresholds (e.g., "above ~X ng/mg = likely to respond to TKI") that mutation status alone can't resolve — because a T790M clone with low EGFR protein may behave differently from a T790M clone with high protein density.
- Signal Transduction Teaching & Method Validation
Even outside oncology, EGFR is the canonical RTK for teaching receptor dynamics: add EGF 0.1–10 nM → watch EGFR pull down into the pellet fraction within 5 min, then disappear into the lysosome by 60 min. The ELISA gives students a plate-read number for that classic internalization curve, replacing "band faded = internalized" with an actual kinetic.
A Minimal Protocol You Can Paste Into Materials & Methods
- Lysate: cold 50 mM Tris pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100/NP-40 + protease + phosphatase inhibitors, keep on ice, sonicate briefly, spin 12,000–16,000 ×g, 15 min, 4°C → supernatant = your EGFR-accessible pool.
- BCA → express ng EGFR / mg total protein.
- Warm kit reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve on every plate.
The Bottom Line
EGFR is the ~170-kDa transmembrane RTK — the HER1/ErbB-1 gatekeeper whose ligand-triggered dimerization and bilobate kinase domain invented the modern TKI era and still drives the therapeutic logic of gefitinib → osimertinib, cetuximab, and the next generation of EGFR-directed ADCs and degraders. Measuring it as a calibrated ELISA variable instead of a "170 kDa band / actin" ratio changes your kinase/oncogene paper from suggestive to quantitative: it gives you the receptor-density denominator that decides whether the mutant is even sitting at the surface to be drugged. The Human Epidermal Growth Factor Receptor (EGFR) ELISA Kit — KTE62577 from Abbkine gives you that denominator: pre-coated capture → biotin detection → HRP–TMB → 450 nm → ng/mL, over a 0.156–10 ng/mL (extended options to 3.12–200 ng/mL depending on calibrator) working envelope, in a ~3–5 hour workflow that scales across TKI dose-plates, resistance clones, and lysate cohorts without chaining you to a single gel transfer.
Product Reference: KTE62577 – Human Epidermal Growth Factor Receptor (EGFR) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-epidermal-growth-factor-receptor-egfr-elisa-kit-kte62577/
(For Research Use Only; not for diagnostic procedures in humans.)





