




The 17-kDa Fire Alarm That Won't Stay in the Macrophage: Why Your "Inflammasome Activated" Claim Collapses Without a 8-pg/mL IL-1β Sandwich Read — And How KTE7005 Puts the Pyroptotic Cytokine on a 450 nm Curve You Can Actually Defend
IL-1β is the only cytokine in the mouse house that forces you to admit an uncomfortable truth: your cells might be making plenty of precursor protein, but until a NLRP3–ASC–caspase-1 inflammasome actually snips the pro-form at Asp¹¹⁶ (human numbering conventions in the mouse equivalent), all that ~31–35 kDa pro-IL-1β is a harmless cytoplasmic cargo pod sitting behind a nuclear export/translation firewall. The mature, secreted effector is a ~153-aa polypeptide, computed ~17.5 kDa (runs ~17 kDa on reducing gels) — and it's the founding member of the entire IL-1 superfamily, the pyrogenic master switch that tells the hypothalamus to hike the setpoint, the endothelium to dial ICAM-1/VCAM-1/E-selectin for leukocyte recruitment, and the liver to crank SAA + CRP (ptldr: serum amyloid A) via NF-κB. The EliKine™ Mouse IL-1β ELISA Kit (KTE7005) from Abbkine is the tool that forces the distinction between "pro-IL-1β accumulated" and "mature IL-1β actually released" — a double-antibody sandwich ELISA delivering a 15.6–1000 pg/mL working range with LOD ~8 pg/mL, so your LPS+ATP, alum, monosodium urate (MSU), or nigericin timecourse rests on interpolated pg/mL, not a "we saw a 17-kDa band and assume it's secreted" inference.
IL-1β in One Paragraph: 31-kDa Pro-Form → Caspase-1 Snip → 17-kDa Secreted Weapon
The biosynthetic logic is what makes IL-1β unique among the big-name cytokines — and it's also why lazy quantification ruins more papers than reviewers like to admit:
Step Driver Molecule Location
Transcription/translation NF-κB (TLR4→MyD88→IRAK→IKK→NF-κB) pro-IL-1β (precursor, ~266 aa, ~31–35 kDa, no signal peptide!) Cytosol (stored un-exported; lacks classical N-terminal signal sequence — exported via gasdermin D pores after pyroptosis, not ER-Golgi secretory pathway)
Inflammasome assembly NLRP3 (LPS priming → second hit: ATP/alum/MSU/nigericin → K⁺ efflux/lysosomal rupture/ROS) → ASC speck → recruits caspase-1 (p45 → p20+p10) Caspase-1 cleaves pro-IL-1β at Asp¹¹⁶ Cytosol → mature IL-1β (p17, ~17 kDa) freed
Release Pyroptotic rupture (GSDMD-N pores) Mature IL-1β floods supernatant Paracrine: binds IL-1R1 + IL-1RAcP → MyD88 → IRAK → NF-κB + MAPK on target cells
The clinical number everyone recognises: IL-1β is the target of anakinra (IL-1Ra, Kineret®), canakinumab (anti-IL-1β mAb), and rilonacept (IL-1 Trap) — approved for CAPS/NOMID (cryopyrin-associated periodic syndromes), RA, gout flares, and now cardiovascular risk reduction (CANTOS trial: anti-IL-1β → ↓ recurrent MI via hsCRP axis). But the mouse work that justified those drugs always came down to one readout: how much mature IL-1β actually escaped the macrophage.
Why the Sandwich ELISA — And Why "pro-IL-1β Western" Is the Wrong Quant for Secretion
Three reasons the gel-alone approach fails specifically for IL-1β:
- pro-IL-1β (
31 kDa) and mature IL-1β (17 kDa) can both be in your lysate, but only the 17 kDa form should be in your supernatant — and if you're running a densitometer on a whole-lysate lane and calling it "IL-1β secretion," you're measuring a pellet artifact, not a release event. - A sandwich ELISA using paired anti-mouse IL-1β mAbs directed at the mature p17 epitope(s) bypasses the pro-form background problem: it reads mature, released IL-1β in the extracellular compartment, not the precursor pool stacking up in the cytosol.
- Your experiment is a timecourse (BMDM: 0 h → LPS 3 h → ATP 30/60/120 min; or in vivo: 2 h / 6 h / 24 h post-MSU peritonitis) — that needs plate-scale pg/mL numbers, not a triplicate gel.
The KTE7005 architecture is the classic two-site build confirmed across Abbkine's own CN-site and distributor listings:
- Microplate pre-coated with a mouse IL-1β-specific capture antibody (mouse-sourced antibody pair, optimised for murine p17 epitopes).
- Standards (recombinant mouse IL-1β protein standard) + samples — cell culture supernatants, serum, plasma (EDTA/heparin), peritoneal lavages, other biological fluids — added → IL-1β captured.
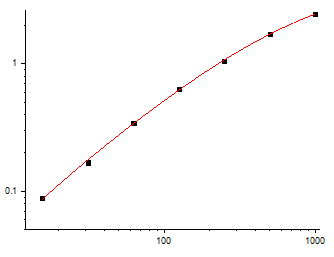
- Wash → biotinylated anti-mouse IL-1β detection antibody (different epitope) → EliKine™ Streptavidin–HRP → TMB → stop → 450 nm → interpolate pg/mL from the 4-PL standard curve.
Parameter KTE7005 — EliKine™ Specification
Target Mouse IL-1β (UniProt P10749, Gene ID 16176)
Format Sandwich ELISA, pre-coated capture (双抗体夹心法)
Detection Biotin-Ab → EliKine™ SA–HRP → TMB, 450 nm
Dynamic Range 15.6 – 1000 pg/mL
Sensitivity / LOD ~8 pg/mL
Intra-Assay CV < 8%
Inter-Assay CV < 10–12%
Recovery (serum) 93–107%
Specificity No significant cross-reactivity with mouse IL-1α or other analogous cytokines at physiological levels
Samples Cell culture supernatants, serum, plasma (EDTA/heparin), peritoneal lavage, tissue homogenate supernatants, other biological fluids
Assay time ~2–3 hours (pre-coated plate + ready-to-use buffers)
Storage (unopened) 2–8°C
(Always lock Methods to the shipped Abbkine CoA/datasheet for your specific lot.)
The Prep Rule That Keeps Your 8 pg/mL Real
IL-1β is stable enough at 4°C for a day, but the biology around it is thermally sensitive:
• Cell culture supernatants (the #1 matrix): harvest at the programmed timepoint, spin ≥ 10,000 ×g, 5–10 min, 4°C to drop cells/debris (you do not want a lysed-well contaminating your "secreted" read), take clear supernatant, store -80°C, avoid >1 freeze–thaw. Keep serum-free or ≤ 1–2% FBS (FBS is IL-1β-null for most qualified batches, but high-FBS adds bulk protein that can mildly raise baseline OD — run a medium-only blank always).
• Serum/plasma: EDTA preferred, cold chain, spin promptly, aliquot, -80°C, single thaw.
• Peritoneal lavage (MSU/alum peritonitis model): lavage with 5 mL ice-cold PBS + 0.1% BSA/EDTA → spin → supernatant → read immediately or -80°C. The lavage IL-1β (pg/mL × lavage volume) is the gold-standard for in vivo inflammasome pharmacology.
Where IL-1β Quantification Actually Carries the Paper
- The NLRP3 Inflammasome: The Gold-Standard Two-Hit & Why the 17-kDa Band Is Never Enough
This is the canonical. BMDMs (or thioglycollate-elicited peritoneal macrophages):
• Hit 1 (priming): LPS 100 ng/mL, 3 h → NF-κB → pro-IL-1β builds up (lysate is full of ~31 kDa band)
• Hit 2 (activation): ATP 5 mM / nigericin 10 μM / MSU crystals / alum, 30–60 min → NLRP3 fires, caspase-1 cleaves, p17 released
• Read supernatant IL-1β by KTE7005 (pg/mL) → this is the only compartment that proves secretion
• Parallel lysate pro-IL-1β (Western, p31 vs. GAPDH) → proves priming
• Parallel caspase-1 p20 (Western, ~10 kDa active fragment) or FLICA/YVAD-AFC → proves inflammasome assembly
• Optional: LDH (membrane integrity) to prove release is pyroptosis-driven, not generic lysis
That triad — pro-form in pellet, p17 in supernatant, caspase-1 active — is the 30-second checklist that prevents a reviewer from writing "How do we know it's not just leaky membranes?"
- Gout & Crystal Inflammation (MSU/Uric Acid Crystal Model)
The reason colchicine and corticosteroids work for acute gout isn't "they kill neutrophils" — it's that MSU crystals → phagolysosomal rupture → NLRP3 activation → IL-1β flood → endothelial adhesion cascade → attack. The in vivo readout is peritoneal lavage or ankle-joint homogenate supernatant IL-1β (KTE7005, pg/site or pg/mg tissue) alongside neutrophil counts (myeloperoxidase MPO), swelling volume, and paw-calipers — and the pharmacological proof is: anakinra/anti-IL-1β blocks the attack without touching urate crystals themselves.
- Metabolic Inflammation (HFD, Palmitate, Saturated FA → NLRP3 in Adipose/MΦ)
This is where IL-1β became a metabolic villain: saturated fatty acids (palmitate) and crown-like structures in omental adipose drive low-grade NLRP3 priming + TXNIP-mediated activation → chronic low-level IL-1β secretion (~50–300 pg/mL supernatants, ~pg/mL in fasted serum) → JNK/IRS-1 serine phosphorylation → insulin resistance. KTE7005 lets you run epididymal fat explants or SVF-conditioned media (pg/mL, BCA-normalised) across diet arms (chow vs. HFD vs. HFD+MCC950/NLRP3i) and show the cytokine axis is live — not just "TNF was up too."
- Neuroinflammation & Microglial Pyroptosis (LPS → Aβ → MSU-like cascades)
Microglia primed by systemic LPS (1 mg/kg ip) or Aβ oligomers → second hit (ATP/CSF1R dynamics) → IL-1β release that drives S1P/COX-2/PGE₂/endothelial VCAM-1 and sickness-behavior (anhedonia-like, social withdrawal). Hippocampal CA1 microdissection → tissue homogenate → KTE7005 (pg/mg protein) is the structural anchor next to Iba1 CD68, NLRP3 IF, and sucrose-gradient ASC-speck quantification.
- Anti-Inflammasome Drug Screens (MCC950, CY-09, OLT1177, CRID3)
If you're testing a NLRP3-specific inhibitor, don't stop at "it reduced caspase-1 p20." Report % IL-1β secretion remaining ± SEM from the calibrated curve (pg/mL supernatant → normalised to total protein or pro-IL-1β lysate), and close the loop with ASC speck-oligomerisation (cross-linking + Western) or FLICA so the inhibitor's target is airtight. That's the evidence package that separates mechanism from phenomenology.
- In Vivo Peritonitis / Sepsis-LPS Models (The Systemic Fire Alarm)
Systemic LPS (10–20 mg/kg ip in mice) → peak serum IL-1β ~1–3 h (short window, then IL-1Ra and decoy IL-1R2 clamp it down). Tail bleed → EDTA plasma → KTE7005 gives you the peak pg/mL that correlates with hypothermia, TNF-α, and IL-6. If you're testing NLRC4 (flagellin) vs. NLRP3 triggers, the IL-1β kinetic is the first variable that tells them apart temporally.
A Minimal Protocol You Can Paste Into Materials & Methods
- Culture supernatants: harvest at exact timepoint, spin ≥ 10,000 ×g, 5–10 min, 4°C, collect clear sup, -80°C, avoid >1 freeze–thaw. Include a medium-only (no-cell) well as background control.
- Serum/plasma: EDTA, wet ice, spin ≥ 2,000 ×g, 10 min, 4°C, aliquot, snap -80°C, single thaw.
- Dilute into kit assay buffer per manual (most stimulated supernatants land neat or 1:2–1:5 inside the 15.6–1000 pg/mL window).
- Warm reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate.
The Bottom Line
IL-1β is the ~153-aa, ~17-kDa pro-inflammatory cytokine that has to be primed (NF-κB → pro-IL-1β precursor) then activated (NLRP3–ASC–caspase-1 → Asp¹¹⁶ cleavage → mature p17 exported via gasdermin D pores) before it ever becomes a secreted signal — which means "pro-IL-1β was present on a gel" is never proof of function, and only a two-epitope sandwich ELISA reading mature p17 in the extracellular compartment can give you the secreted mass you claim your inflammasome is firing. The EliKine™ Mouse IL-1β ELISA Kit — KTE7005 from Abbkine gives you that readout: pre-coated anti-mouse IL-1β capture → biotin detection → EliKine™ SA–HRP → TMB → 450 nm → pg/mL, over a 15.6–1000 pg/mL calibrated range with LOD ~8 pg/mL (Intra CV < 8%, Inter CV < 12%, recovery 93–107%), in a ~2–3 hour workflow that scales from a 48-well BMDM inflammasome panel to a peritonitis lavage cohort without chaining you to a densitometer.
Product Reference: KTE7005 – EliKine™ Mouse IL-1β ELISA Kit
Learn more and order: https://www.abbkine.com/product/elikine-mouse-il-1%ce%b2-elisa-kit-kte7005/
(For Research Use Only; not for diagnostic procedures in humans.)





