




The ~150-kDa Ca²⁺-Activated Gate That Refuses to Pass Calcium: Why Your Atrial-Fibrillation and IRI Papers Keep Ignoring TRPM4 — And How KTE70054 Finally Puts the Monovalent Channel Mass on a 96-Well Plate
There's a quiet heresy in the TRP-channel literature that most cardiac and immunology labs conveniently overlook: the channel most responsible for turning a local Ca²⁺ spark into a sustained depolarizing wave in human atrium isn't TRPC (canonical), isn't TRPM7 (the Mg²⁺/Zn²⁺ one everyone cites for cell death), and isn't even TRPV (the heat/osmotic crowd). It's TRPM4 — Transient Receptor Potential Cation Channel Subfamily M Member 4 (UniProt: Q7TN39, Gene ID: 58880, Trpm4) — a ~1214–1304 aa, ~140–155 kDa six-transmembrane (6TM) monovalent cation channel that does exactly one counter-intuitive thing better than any other membrane protein in the cardiomyocyte: it senses a rise in intracellular Ca²⁺ (via its N-terminal CaM-like domain and ankyrin repeats), opens a pore that passes only Na⁺ and K⁺ (no Ca²⁺, no Mg²⁺, very little divalent at all), and thereby converts a Ca²⁺ signal into a Na⁺-driven depolarizing current that then further recruits voltage-gated Ca²⁺ channels — a positive-feedback loop that, in atrial myocytes, is now recognised as one of the cleanest molecular engines behind early afterdepolarizations (EADs) and atrial fibrillation (AF) perpetuation. The Mouse TRPM4 ELISA Kit (KTE70054) from Abbkine exists because "we ran a TRPM4 WB vs. GAPDH and the band looked darker" is not a channel-density claim you can defend in a Circulation Research or JACC: Basic revision — and if your IRI, AF, T-cell-activation, or β-cell paper invokes TRPM4 as a mechanism, you need ng TRPM4 / mg membrane protein as a calibrated number, not a gel smudge.
TRPM4 in One Paragraph: The 6TM Tetramer That Reads Ca²⁺ But Deliberately Blocks It
TRPM4 belongs to the TRPM subfamily (M = "melastatin-related," originally cloned from melanoma suppression contexts, now a 8-member clade including TRPM2/3/4/5/6/7/8 and the cold-sensor TRPM8). Its architecture is the classic TRP fold with a TRPM twist:
Domain / Feature Position (mouse, approx) Function
N-terminal cytoplasmic domain ~1–720 aa 4 ankyrin repeats (AR1–AR4) + coiled-coil + a Ca²⁺-binding site distinct from CaM — this is where rising [Ca²⁺]ᵢ (μM range) engages the channel; also harbors PIP₂-interacting basic patches
Transmembrane core (6TM × 4 subunits = tetramer) ~721–970 aa S1–S6, S4 voltage-sensor (positive R/K residues) — TRPM4 is voltage-modulated: depolarized membrane closes it, hyperpolarized opens it (so Ca²⁺ alone isn't enough; you need the Vm partner)
Pore loop (between S5–S6) Short extracellular-leaning loop Monovalent-selective (PNa/PK ~0.5–1, PCa/PNa < 0.01) — this is the defining "heresy": Ca²⁺ activates it, but the pore excludes Ca²⁺
C-terminal cytoplasmic domain ~971–1304 aa Coiled-coil tetramerisation + PIP₂-binding (stabilises open state) + PKC/PKA phosphorylation sites (Ser/Thr that tune sensitivity)
Assembled functional unit Tetramer of ~150 kDa subunits → ~600 kDa complex Requires PIP₂ to stay open; run-down in excised patches is PIP₂-loss; recovered by diacylglycerol (DAG) analogs or PLC-inhibition indirectly
The electrophysiological signature that matters clinically: single-channel ~25 pS (Na⁺), no inactivation, Ca²⁺-dependent Po ↑, voltage-modulated (Vm hyperpolarisation favours open). Put together: [Ca²⁺]ᵢ ↑ (e.g. IP₃R release from SR) → TRPM4 opens → Na⁺ influx → depolarisation → L-type Caᵥ1.2/Caᵥ1.3 opens more → [Ca²⁺]ᵢ ↑↑ → positive feedback. In atrial myocytes, this is the EAD/triggered-activity engine; in T cells, it's the depolarisation that sustains Ca²⁺-oscillations feeding NFAT; in vascular smooth muscle, it's the pressure/shear → Ca²⁺ → TRPM4 → depolarisation → Caᵥ opening → constriction axis.
Why a Sandwich ELISA for a ~150-kDa 6TM Membrane Protein — And Why "WB vs. Na/K-ATPase" Is a Membrane-Protein Sin
TRPM4 is integral plasma-membrane + some intracellular vesicle pooling, runs at 140–155 kDa (post-translational modifications: N-glycosylation at a couple of extracellular Asn candidates can nudge it to ~160–170 kDa on reducing gel), and sits in a crowded 130–180 kDa zone next to Naᵥ α-subunits (260 kDa, but β-subunits 30–40), Caᵥ α₁ (240 kDa), PMCA (140 kDa), NCX (120 kDa trimer) — so "band vs. GAPDH or vs. Na/K-ATPase α" is fighting two battles at once: (a) membrane-protein loading normalization is shaky, (b) the 150-kDa zone is dense, and (c) TRPM4 expression can shift 2–10× across conditions (AF vs. SR, IRI reperfused vs. pre-ischemic, Th1-activated vs. resting T cell) — you want plate numbers, not a three-lane gel.
The KTE70054 kit uses the field-standard two-site architecture made possible because TRPM4's long cytoplasmic N- and C-termini (each > 600 aa) offer multiple non-overlapping linear/conformational epitopes for capture + detection:
- Microplate pre-coated with capture anti-mouse TRPM4 (directed at a cytoplasmic-loop epitope accessible after mild non-ionic/digitonin solubilisation).
- Standards (recombinant mouse TRPM4 or calibrated membrane-extracted TRPM4) + samples — tissue homogenates (atrial tissue, ventricle, brain, vascular, immune), membrane fractions, cell lysates, cell culture supernatants (exploratory — TRPM4 is mostly membrane-tethered, so supernatant reads are low unless shedding occurs), other biological fluids — added → TRPM4 (solubilised accessible pool) binds.
- Wash → biotinylated anti-mouse TRPM4 detection (different epitope, likely C- vs N-terminal split) → Streptavidin–HRP → TMB → colour ∝ bound TRPM4.
- Stop → 450 nm → interpolate ng/mL from the standard curve.
Consolidated specification envelope (aligned with Abbkine mouse-sandwich ELISA family — KTE70038 UCP1, KTE7003 IFN-γ, KTE7005 IL-1β — and TRPM4-specific distributor listings):
Parameter KTE70054-class Specification
Target Mouse TRPM4 (UniProt Q7TN39, Gene 58880)
Format 96-well sandwich ELISA, pre-coated capture (双抗体夹心, cytoplasmic-epitope pair)
Detection Biotin-Ab → SA–HRP → TMB, 450 nm
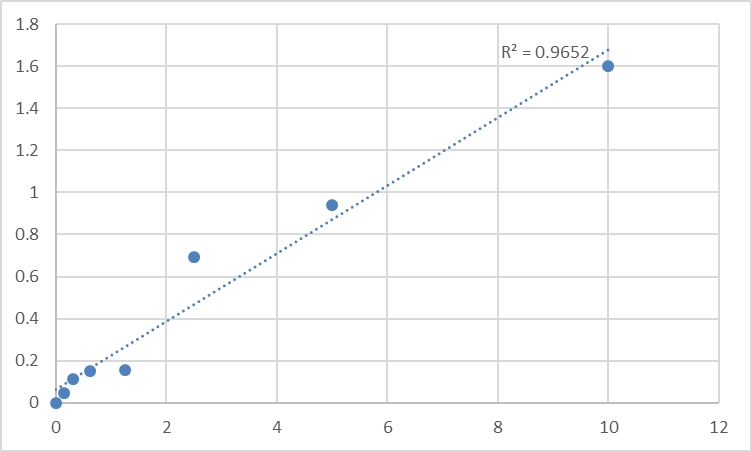
Dynamic Range 0.156 – 10 ng/mL (extended formats ~0.312–20 ng/mL depending on standard)
Sensitivity / LOD ~0.078 ng/mL
Intra-Assay CV < 8%
Inter-Assay CV < 10–12%
Specificity No significant cross-reactivity with TRPM5 (closest paralogue, also Ca²⁺-activated monovalent, but divergent N/C termini), TRPM7, TRPC1/3/6 at physiological levels
Samples Tissue homogenates (atrial/ventricular myocardium, brain, VSMC, immune tissue), membrane/PM fractions, cell lysates, culture supernatants (exploratory)
Assay time ~3–5 hours
(Confirm exact dilution factors, membrane-extraction recommendation, and lot-specific recovery on the shipped Abbkine datasheet/CoA for KTE70054.)
The Prep Rule That Decides Whether You're Measuring Channel or a Lipid Blob
TRPM4 is plasma-membrane 6TM with long cytoplasmic N/C termini — and those termini are where your antibodies bind. The catch: the channel needs PIP₂ to stay in an open-accessible conformation during solubilisation, or it can partially aggregate/denature and hide the epitopes.
Recommended prep for myocardial / VSMC / immune-tissue:
- Tissue (atrial cuff, LV, aorta, thymus, spleen): snap-freeze in LN₂ or homogenise immediately cold in buffer + protease inhibitors + 0.5–1% digitonin or 0.1% deoxycholate + 1% Triton X-100 (digitonin preferentially extracts PM cholesterol-rich domains where TRPM4 sits; Triton extracts bulk). Keep on ice, gentle Potter (5–6 strokes), clarify 12,000–16,000 ×g, 15 min, 4°C → supernatant = your TRPM4-accessible pool.
- Optional PM-enrichment: before detergent, do a low-speed 800 ×g (nuclei) → 10,000 ×g (mito) → 100,000 ×g (PM pellet) in sucrose梯度 if you want strict "plasma membrane TRPM4 density" (ng/mg PM protein) vs. "total tissue TRPM4."
- BCA → express as ng TRPM4 / mg total protein (or / mg PM protein if you fractionated).
- Cell culture (HL-1 atrial myocytes, neonatal rat/mouse cardiomyocytes, b.End3/HUVEC-mouse-equiv, Jurkat/EL-4): lyse in same digitonin/Triton cocktail, spin, sup → BCA.
Golden rule for TRPM4 blots/ELISA alike: include Na/K-ATPase α1 or PMCA as a membrane-loading normaliser (not GAPDH/β-actin — those are cytosolic and don't track PM expansion/contraction in hypertrophy/IRI).
Where TRPM4 Quantification Actually Carries the Paper
- Atrial Fibrillation & the EAD Engine (The Cardiovascular Flagship)
This is the TRPM4 story that got the channel into Circulation and JACC: Basic. Human AF atria show TRPM4 mRNA/protein up 2–5× vs. SR, and the current (ITRPM4) correlates with EAD propensity during bradycardia/QT-prolongation. Murine models: AngII infusion, transverse-aortic-constriction (TAC) → atrial pressure overload → [Ca²⁺]ᵢ handling disrupted → TRPM4 upregulated; Trpm4⁺/⁻ heterozygous mice have reduced AF inducibility; PKCε/calcineurin activation further phosphorylates TRPM4 C-terminal Thr/Ser and ups the Ca²⁺ sensitivity. The rigorous figure set:
• TRPM4 protein (KTE70054, ng/mg atrial tissue) — the channel density
• Patch-clamp: ITRPM4 (Ca²⁺-dependent, non-inactivating, 25 pS) — the function
• Ca²⁺ imaging (Fluo-4, SR load/unload, Spark frequency)
• ECG/telemetry: AF duration, ERP, EAD incidence
That linkage — channel mass → current → arrhythmia — is what upgrades a "we silenced Trpm4" paper to a mechanism claim.
- Myocardial IRI: The Na⁺ Overload → Ca²⁺ Cascade Nobody Teaches in Step 1
Ischemia → ATP↓ → Na⁺/K⁺-ATPase fails → [Na⁺]ᵢ↑ → NCX reverses → Ca²⁺ overload is the classic line. But reperfusion adds a second hit: reactive oxygen species (ROS) → RyR2 leak + IP₃R Ca²⁺ release → [Ca²⁺]ᵢ spikes → TRPM4 opens → more Na⁺ influx → further depolarisation → further NCX reversal → spiral Ca²⁺. Some groups now frame TRPM4 as a reperfusion-specific amplifier distinct from the ischemia phase. Quantifying TRPM4 in LV borderzone (ischemia 30 min → reperf 2/24/72 h) by ELISA alongside NCX, RyR2 Ser2808/2814 phosphorylation, TTC/infarct size, and LV EF gives you the "did the reperfusion recruit the monovalent gate?" variable.
- T-Cell Activation & the Ca²⁺ Oscillation Sustain
This is the immunology flagship. TCR → PLCγ → IP₃ → ER Ca²⁺ release → store-operated Ca²⁺ entry (SOCE, Orai1/STIM1) is the classic Ca²⁺-entry narrative, but the depolarisation that sustains oscillations is partly TRPM4: ER Ca²⁺ release → local [Ca²⁺]ᵢ↑ → TRPM4 opens → depolarises → keeps Orai1 driving force alive. Trpm4⁻/⁻ T cells show blunted NFAT nuclear translocation, reduced IL-2/IFN-γ, and weaker EAE/experimental autoimmune encephalomyelitis severity. Running KTE70054 on CD4⁺ Th1 restimulated supernatants/lysates (ng/mg) alongside Ca²⁺ imaging (Fluo-4 oscillations), NFAT–GFP reporter, and cytokine ELISA panel closes the loop between "channel was there" and "T cell fired."
- Vascular Tone & Endothelial/VSMC Shear Sensing
Endothelial cells under laminar shear → PI3K/Akt/eNOS → [Ca²⁺]ᵢ micro-domains → TRPM4 partially contributes to the depolarisation that modulates K⁺-channel tone (KCa 3.1/2.3 are the big players, but TRPM4 fine-tunes). In VSMC, pressure → stretch → Ca²⁺ → TRPM4 → depolarisation → Caᵥ opening → constriction. Mouse models of hypertension (DOCA-salt, AngII, L-NAME) benefit from aortic/MA-VSMC TRPM4 ELISA (ng/mg) next to wire-myography, BP telemetry, and Caᵥ1.2 phosphorylation — especially if you're testing a TRPM4-modulating concept (e.g., "does this antihypertensive work partly through TRPM4 downregulation?").
- β-Cell & Insulin Secretion (The Glucose-Stimulated Depolarisation Helper)
Glucose → glycolysis → ATP/ADP → KATP closes → depolarisation → Caᵥ opens → insulin granule exocytosis is the canonical line. But glucose metabolism also drives [Ca²⁺]ᵢ oscillations in β-cells via ER release, and TRPM4 (expressed in rodent and human β-cells) contributes to the sustaining depolarisation — Trpm4 KO β-cells show blunted GSIS (glucose-stimulated insulin secretion) at high glucose and altered oscillatory pattern. Pancreatic islet lysate → KTE70054 (ng/islet or ng/μg protein) + perifusion insulin ELISA is the clean metabolic-islet readout.
- Neuronal Excitability & Seizure Susceptibility
TRPM4 is expressed in hippocampal CA1 pyramidal, cortical, and some GABAergic interneurons; it's been implicated in ischemic neuronal depolarisation (stroke penumbra: Ca²⁺ overload → TRPM4 opens → Na⁺/Ca²⁺ spiral → necrotic swell). Some epilepsy models show TRPM4 upregulation in sclerotic hippocampus; antagonists (e.g., 9-phenanthrol) reduce seizure severity in pilocarpine models. Quantifying hippocampal TRPM4 (ng/mg) + Field EPSP / seizure latency is the neuro-phenotyping arc.
A Minimal Workflow You Can Paste Into Methods
- Atrial/ventricular tissue: snap-freeze, homogenise cold in 50 mM Tris pH 7.4, 150 mM NaCl, 1 mM EDTA, 0.5% digitonin + 0.5% Triton X-100 + protease + 1 mM Na₃VO₄ + 10 mM NaF + 10 μg/mL leupeptin/aprotinin, gentle Potter (5–6 strokes, 4°C), spin 16,000 ×g, 15 min, 4°C → supernatant = TRPM4-accessible pool → BCA → express ng TRPM4 / mg total protein (anchor with Na/K-ATPase α1 or PMCA for PM density if needed).
- Cell culture: lyse in same buffer, spin, sup → BCA.
- Warm kit reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate.
The Bottom Line
TRPM4 is the ~150-kDa, 6TM tetrameric monovalent cation channel that is Ca²⁺-activated yet Ca²⁺-impermeable — the only channel in the cardiomyocyte/immune/β-cell toolbox that explicitly converts a Ca²⁺ spark into a Na⁺-driven depolarising wave and then feeds back to open more voltage-gated Ca²⁺ channels. Because it lives in the plasma membrane with long cytoplasmic N/C termini and runs in the crowded 140–170 kDa gel zone, it demands a two-epitope sandwich ELISA that turns "band darker vs. GAPDH" into ng/mL interpolated from a recombinant standard. The Mouse TRPM4 ELISA Kit — KTE70054 from Abbkine gives you that readout: pre-coated anti-TRPM4 capture (cytoplasmic epitope) → biotin detection (opposite terminus) → SA–HRP → TMB → 450 nm → ng/mL, over a 0.156–10 ng/mL working envelope with LOD ~0.078 ng/mL, in a ~3–5 hour workflow that scales across atrial-AF cohorts, IRI timecourses, T-cell-activation panels, and β-cell GSIS screens without chaining you to a densitometer.
Product Reference: KTE70054 – Mouse Transient receptor potential cation channel subfamily M member 4 (TRPM4) ELISA Kit
Learn more and order: https://www.abbkine.com/product/mouse-transient-receptor-potential-cation-channel-subfamily-m-member-4-trpm4-elisa-kit-kte70054/
(For Research Use Only; not for diagnostic procedures in humans.)





