




The 13-kDa Heparin-Binding Double Agent: Why Midkine (MK/MDK) Circulating Levels Matter More Than Your Tumor's Ki-67 Index — And How KTE61678 Puts It on a Plate-Readable Curve
If you've been reducing cancer "aggressiveness" to a mitotic index and a VEGF western, you're ignoring the oldest trick in developmental biology: release a single basic, secreted, disulfide-bridged 13-kDa factor into the extracellular space, and suddenly the microenvironment stops asking "should we grow?" and starts building blood vessels to feed the answer. That factor is Midkine (MK, gene symbol MDK, UniProt: P21741) — originally cloned as the retinoic-acid-responsive "midkine" gene product induced during mid-gestation (hence the name), and the founding member — alongside pleiotrophin (PTN/NEGF1) — of the smallest, most cationic growth-factor family in human biology. Unlike the bulky GF family (EGF/HB-EGF/TGF-α at ~6 kDa but heavily modified, or FGFs at ~17–25 kDa), MK punches with a computed mature mass of ~13 kDa (123 aa after signal-peptide cleavage) that migrates as a ~15–18 kDa band on reducing SDS-PAGE because its 10 conserved cysteines form 5 disulfide bridges that lock it into a rigid, highly stable N-terminal-and-C-terminal two-domain architecture. The Human Midkine (MK) ELISA Kit (KTE61678) from Abbkine is the immunoassay that lets you measure this deceptively tiny, fiercely heparin-loving cytokine as a calibrated, two-site sandwich ELISA concentration (pg/mL) — so your tumor-biology, tissue-repair, or inflammatory study stops waving at "angiogenesis happened" and starts quantifying the secreted commander that ordered it.
MK in One Paragraph: A 123-Aa Disulfide-Caged Double Agent
MK is not a promiscuous "weirdly basic peptide" — it's a folded, secreted, two-domain protein with a basic N-domain (heparin-/CS-binding rich) and a C-domain separated by a flexible hinge, and it pulls strings through an unusually broad receptor orchestra:
Receptor/Partner Functional Consequence
PTPRZ1 (RPTPβ/ζ) — the main signaling receptor Tyrosine-phosphatase inhibition → β-catenin stabilization, survival, migration
LRP1 (LDLR-related protein 1) + ITGB2 (β2 integrin) Neutrophil/macrophage recruitment; neuronal survival
ALK (anaplastic lymphoma kinase) Direct ALK → IRS1 → MAPK/PI3K → proliferation (the link that made MK a cancer-cell autonomy suspect)
Syndecans (SDC3/GPC2) + Integrins (α6β1, α4β1) Cell adhesion, neurite outgrowth, osteoblast migration
Chondroitin sulfate E / heparin Sequesters MK to ECM; controls spatial presentation (gradient-forming)
Biologically, MK is developmentally essential (mid-gestation embryo expression peaks then drops to near-zero in most adult tissues), but it reawakens in three situations that matter most to a translational lab:
- Malignancy — MDK is among the most consistently upregulated genes in human cancers: neuroblastoma (where high MK = poor outcome), glioblastoma, Wilms', CRC, HCC, ovarian, bladder, breast, lung, esophageal, gastric, prostate.
- Inflammation / tissue injury — MK is pro-angiogenic, anti-apoptotic, and pro-recruitment; after cardiac damage, renal IRI, or vascular injury, MK-negative feedback loops modulate inflammatory cell influx while promoting endothelial survival (dual nature: protective repair vs. pathological neovascularization).
- Repair & regeneration — liver, bone, cartilage: MK recruits macrophages to trauma sites and promotes chondrocyte differentiation.
Normal human serum MK is very low: usually < 0.5–0.6 ng/mL (500–600 pg/mL) — and that's exactly why a high-sensitivity assay matters.
Why a Sandwich ELISA — And Why MK's Tiny Size Doesn't Force You Into Competitive
A perennial confusion: "MK is only 13 kDa — don't you need a competitive hapten assay?"
No — and here's why the MK kits use sandwich, not competition:
Yes, MK is small, but it has ~123 aa with multiple distinct surface epitopes (the N-domain, hinge, and C-domain are structurally/immunologically separable), and — crucially — it carries 5 rigid disulfide bridges that prevent it from behaving like a floppy unstructured peptide. That structural rigidity means two well-selected anti-MK monoclonal/polyclonal antibodies can bind non-overlapping epitopes simultaneously, making a two-site sandwich ELISA not just possible but preferable for sensitivity and specificity over competitive.
The KTE61678 architecture is textbook:
- Microplate pre-coated with capture anti-MK (MDK) antibody.
- Standards (recombinant human MK/MDK) + samples — serum, plasma, tissue homogenates, cell culture supernatants/lysates, other biological fluids — added → MK binds.
- Wash → biotinylated anti-MK detection (different epitope) → Streptavidin–HRP.
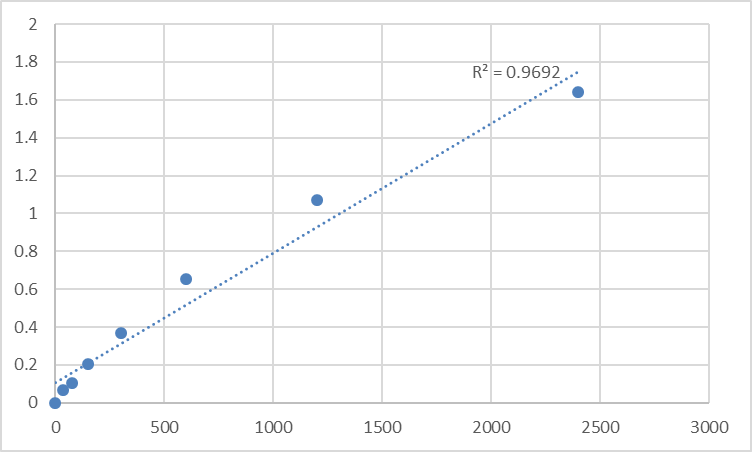
- TMB → stop → 450 nm → interpolate MK concentration from the standard curve.
Consolidated specs from distributor/technical sources aligned with this kit family:
Parameter KTE61678-class Specification
Target Human Midkine / MK / MDK (UniProt P21741, Gene 4194 / MDK, mature ~13 kDa / ~15–18 kDa on gel)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → SA-HRP → TMB, 450 nm
Range 31.25 – 2,000 pg/mL
Sensitivity / LOD ~7.8–9.4 pg/mL
Intra-Assay CV < 8%
Inter-Assay CV < 10–12%
Specificity No significant cross-reactivity with PTN/analogues at physiological levels
Samples Serum, plasma (EDTA preferred), tissue homogenates, culture supernatants/lysates
Assay time ~3–5 hours
(Confirm exact dilutions and lot-specific recovery on the Abbkine datasheet for KTE61678.)
Sample-Handling Note: MK Is Basic, Stable — But Don't Treat the Draw Casually
MK is secreted and relatively stable in EDTA plasma when cold-processed, but because it binds heparin and negatively charged GAG surfaces, it can:
• Adsorb to glass/plastic at very low concentrations (low-binding tubes help for neat serum dilution series)
• Complex with heparin contamination (e.g., from poorly washed glassware or heparinized catheter lines) — EDTA is preferred; avoid heparinized plasma if you can
• Process cold, spin within 30–60 min, aliquot, -80°C, avoid >1 freeze–thaw
Where MK Quantification Actually Drives the Paper
- Cancer: The "Silent" Tumor-Load Marker You're Not Measuring
Serum MK is < 0.5 ng/mL in healthy adults and rises 2–10× in many malignancies — and it does so before imaging catches size. In neuroblastoma (the poster-child), MK mRNA/protein is one of the strongest independent prognostic secreted markers, sometimes outperforming NSE or LDH in treatment-response stratification. Running KTE61678 on coded pre/post-treatment plasma/serum banks (pg/mL, interpolated, normalized only if you have a true MK-free internal control band) lets you test whether your therapy actually suppressed the tumor's secretory aggressiveness — not just shrank a mass.
- Liver Regeneration & Hepatocarcinogenesis
MK is retinoic-acid responsive and re-expressed during hepatic lobectomy/regeneration; conversely, HCC upregulates it massively as part of a pro-proliferative, anti-apoptotic, angiogenic program. Liver-tissue homogenates + adjacent-benign + HCC core → MK ELISA (ng/mg protein) gives you the secretory-drive axis that complements AFP, GPC3, and Ki-67 without requiring you to guess from IHC intensity alone.
- Cardiovascular Repair vs. Neointima: The MK Paradox
After arterial injury (balloon angioplasty, stenting), MK is induced in the neointima/media where it promotes SMC migration, macrophage recruitment, and angiogenic repair — beneficial short-term, pathological if uncontrolled. Measuring MK in plaque/cuff-tissue lysates or (exploratorily) in plasma after PCI/biopsy models captures the repair-vs-restenosis balance. The Frontiers review frames MK as a "novel player" where the net effect is context-dependent — exactly the situation where a quantitative assay beats a qualitative stain.
- Inflammation, Sepsis & Renal Ischemia-Reperfusion
MK promotes neutrophil and macrophage recruitment via LRP1/β2-integrin crosstalk, but also limits runaway inflammation by driving anti-apoptotic signaling in endothelial/stromal cells. In renal IRI and AKI models, MK in tissue lysates (normalized to BCA/Na⁺K⁺-ATPase) or exploratory urine/plasma gives you the secretory repair factor level alongside NGAL, KIM-1, and histologic score.
- Stem Cell & Differentiation Models (Neurogenesis, Osteogenesis, Chondrogenesis)
MK was literally discovered as a neurite outgrowth-promoting factor in retinoic-acid–treated embryonal carcinoma. In iPSC-derived neuronal, osteoblast, or chondrogenic cultures, MK appears in day-7–21 conditioned media — a plate-readout here replaces "we saw neurites" with "we measured the secreted morphogen that patterned them."
- shRNA/siRNA/CRISPR Validation
Knocking MDK? Report % MK protein remaining ± SEM from the calibrated curve (pg/mL or ng/mg), and co-show the functional payout — tube formation, scratch closure, Annexin V, cleaved caspase-3, or xenograft growth — so the cytokine isn't just "down" but provably linked to the phenotype.
A Minimal Protocol You Can Paste Into Materials & Methods
- Collect in EDTA tubes, invert gently, keep on wet ice, spin ≥ 1,500 ×g, 4°C, 10–15 min within 30–60 min.
- Aliquot plasma (or serum if you must), snap -80°C, label clearly, avoid freeze–thaw.
- For tissue (tumor/liver/kidney): homogenize cold in 50 mM Tris pH 7.4, 150 mM NaCl, 0.5–1% Triton X-100 + protease inhibitors, clarify 12,000–16,000 ×g, 15 min, 4°C → supernatant → BCA → ng MK / mg total protein.
- Warm kit reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate.
The Bottom Line
Midkine (MK/MDK) is the ~13 kDa, 5-disulfide, highly basic heparin-binding growth factor that human embryos scream for during mid-gestation, then silence in almost every adult tissue — until cancer, vascular injury, or regenerative demand wakes it back up to orchestrate angiogenesis, cell survival, and inflammatory recruitment from the secretory compartment. It's small, but it's structurally rigid enough for a two-site sandwich ELISA, and its circulating levels (normally < 0.5–0.6 ng/mL) are exactly the range where a pg/mL-sensitive, matched-antibody-pair format matters. The Human Midkine (MK) ELISA Kit — KTE61678 from Abbkine gives you that format: pre-coated capture → biotin detection → HRP–TMB → 450 nm → pg/mL, over a 31.25–2,000 pg/mL working curve with LOD ~7.8 pg/mL, in a ~3–5 hour workflow that scales from a 50-sample cohort to a conditioned-media time-course without chaining you to densitometry guesses.
Product Reference: KTE61678 – Human Midkine (MK) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-midkine-mk-elisa-kit-kte61678/
(For Research Use Only; not for diagnostic procedures in humans.)





