




The 108-Amino-Acid Gate That Determines Who Catches HBV — And Why Your "Five-Marker" Panel Is Blinded Without preS1-Ag: How KTE62719 Puts the Missing Infectivity Flag on a 450 nm Curve
If your lab works anywhere near hepatitis B serology, you already know the sacred incantation: "HBsAg, HBeAg, anti-HBe, anti-HBc IgM/IgG, anti-HBs — the five-marker panel." It's the clinical backbone. But here's the uncomfortable truth every hepatologist who's chased a HBeAg-negative but HBV-DNA-positive patient eventually learns the hard way: the five-marker panel was never designed to catch the virus that learned to hide. HBV's escape hatch is preC/Core promoter mutation (G1896A stop codon, A1762T/G1764A double mutation) — the exact variants that make the virus HBeAg-negative but still replication-competent and still infectious, because the part of the genome nobody told you to check — the preS1 region of the large surface protein (LHBs / PreS) — is still intact, still making preS1 antigen (PreS1-Ag), and still binding the NTCP (SLC10A1) hepatocyte receptor at amino acids 21–47. The Human Hepatitis B virus pre S1 antigen (HBV preS1-Ag) ELISA Kit (KTE62719) from Abbkine is the reagent that closes this diagnostic blind spot: a two-site sandwich ELISA that quantifies PreS1-Ag in serum/plasma as an interpolated signal (pg/mL or IU/L), so your HBV replication story stops pretending "HBeAg-negative = quiet" and starts proving what's actually still knocking on the hepatocyte door.
preS1-Ag in One Paragraph: The N-Terminal 108–119 Residues That Hold the NTCP Key
The HBV surface open reading frame expresses three co-carboxy-terminal proteins from different start codons — all sharing the same S domain (SHBs, ~226 aa, the "small" HBsAg) but differing at the N-terminus:
• Large surface protein (LHBs / PreS1–PreS2–S, ~389–400 aa): adds the preS2 (aa ~109–174) + preS1 (aa ~1–108/119) N-terminal extensions
• Middle surface protein (MHBs / PreS2–S, ~281 aa): adds preS2 only
• Small surface protein (SHBs / HBsAg, ~226 aa): the classical "Australia antigen" everyone assays
The preS1 domain (aa 1–108/119) is where the action is:
• aa 21–47 = the NTCP (SCL10A1) receptor-binding motif — this is the sole known physiologically relevant hepatocyte-entry determinant for HBV (and HDV) at the plasma membrane
• The preS1 protein is retained in the ER/Golgi during virion assembly, but a fraction is secreted as subviral filament/particle-associated antigen that appears in patient serum — and because it's linked to genome-containing nucleocapsid maturation, its presence tracks with replication-competent, potentially infectious virions
The clinical translation is stark and concise:
Marker What It Tells You What It Misses
HBsAg (+) Exposure/persistence (surface protein still circulating) Cannot distinguish replicating vs. empty subviral particles
HBeAg (+/-) Classic replication proxy (core promoter active) Blind to preC mutants → HBeAg(-) but DNA (+) & preS1 (+)
HBV DNA (+/-) Gold-standard for genome copy number Requires qPCR setup, expensive, not every lab; tells copies not necessarily infectivity gate
preS1-Ag (+/-) Virion-associated, NTCP-binding domain → tracks genome-containing, potentially infectious particles; appears earliest in acute, and catches HBeAg(−) but replicating strains
Why a Sandwich ELISA — And Why "HBsAg Positive" ≠ "Virus Is Actively Trying to Reinfect"
Three reasons PreS1-Ag earns its own immunoassay instead of riding on HBsAg's coattails:
- HBsAg circulates as ~10¹²–10¹³ particles/mL, mostly empty, non-infectious spherical 22-nm subviral particles — so HBsAg mass is a terrible proxy for replication. PreS1-Ag, by contrast, is enriched on the Dane particle (virion) surface and on filamentous subviral forms that co-purify with nucleocapsids, making it a replication-associated surface marker.
- HBeAg-negative variants (G1896A premature stop) lose the classic "e-antigen" readout while preS1 remains intact — meaning adding PreS1-Ag to the panel recovers the detection sensitivity that HBeAg mutation erased.
- PreS1-Ag appears ~1–2 weeks before HBsAg peaks in acute infection, and it clears earlier in successful resolution — so it's also the earliest seroconversion momentum gauge you're not measuring if you stop at five markers.
The KTE62719 kit uses exactly the two-site format the distributor documentation confirms:
- Microplate pre-coated with a capture antibody specific for HBV preS1-Ag (directed at the preS1 N-terminal epitope cluster, not cross-reactive with free HBsAg/MHBs).
- Standards + samples — serum, plasma (EDTA/citrate), other biological fluids — added → PreS1-Ag binds.
- Wash → biotinylated anti-preS1 detection (different epitope) → Streptavidin–HRP → TMB → color ∝ bound PreS1-Ag.
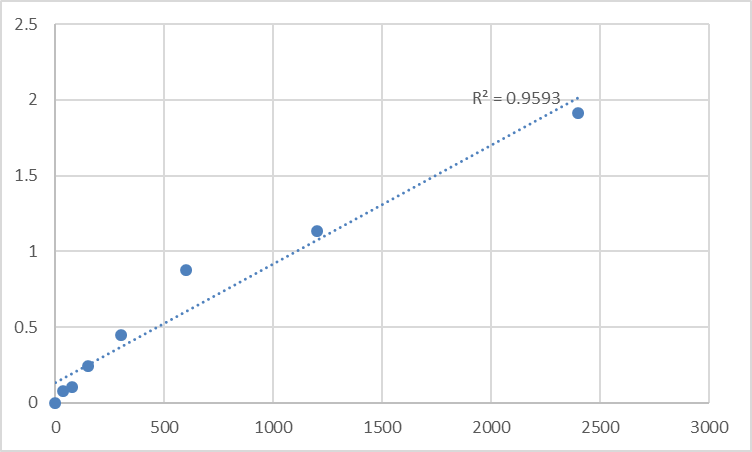
- Stop → 450 nm → interpolate concentration from the standard curve.
Consolidated specs from the distributor/technical sources aligned with KTE62719:
Parameter KTE62719-class Specification
Target Human HBV preS1 antigen (preS1 domain of LHBs; aa ~1–108/119)
Format 96-well sandwich ELISA (quantitative, two-site), pre-coated capture
Detection Biotin-Ab → SA-HRP → TMB, 450 nm
Standard / Range Calibrated reference (expressed in pg/mL or IU/L; typical working standards ~10–120 pg/mL range, with alternate listings quoting 5–80 IU/L)
Sensitivity / LOD ~1–2 pg/mL (depending on standard definition)
Intra-Assay CV < 8–9%
Inter-Assay CV < 10–11%
Cross-reactivity No significant cross-reactivity with HBsAg, HBeAg, anti-HBc, or other HBV serology markers
Samples Serum, plasma (EDTA/citrate), cell culture supernatants, other biological fluids
Assay time ~3–5 hours
(Confirm exact standard identity, concentration units [pg/mL vs. IU/L], dilution scheme, and lot-specific recovery on the shipped Abbkine datasheet/CoA for KTE62719.)
The Sample Rule That Matters: Treat Every Tube as Potentially Infectious, and Don't Kill the Antigen
preS1-Ag is protein epitope, not nucleic acid — so your concern isn't DNase/RNase, it's:
• Proper handling as a BSL-2 specimen (HBV-positive serum = bloodborne pathogen)
• Avoid NaN₃ (azide poisons HRP)
• EDTA or citrate preferred, spin promptly, aliquot, -20°C / -80°C, avoid unnecessary freeze–thaw
• Never mix with bleach before the assay (hypochlorite can oxidize the preS1 N-terminal epitope)
Where preS1-Ag Quantification Actually Changes the Conclusion
- The HBeAg(–) / HBV-DNA(+) Diagnostic Blind Spot
This is the definitive use case. Study after study (363 HBsAg+ samples analyzed with ELISA FQ-PCR) shows:
• HBeAg(+) group: PreS1-Ag positive ~79–92% — consistent with replication
• HBeAg(–) group (e.g., HBeAb(+)/HBcAb(+) pattern): PreS1-Ag still positive ~35–50%, proving replication continues despite the e-antigen vanishing
• preS1-Ag correlates with HBV-DNA copy number (χ² = 198.58, P < 0.01, r ≈ 0.59) — not perfect overlap, but far superior to HBeAg alone for detecting active infection
Running KTE62719 on coded HBsAg+ sera (HBeAg+ vs. HBeAg– strata) and plotting PreS1-Ag vs. log₁₀ HBV-DNA copies/mL is the figure that forces the reviewer to admit: five markers aren't enough.
- Acute HBV: Earliest Viremic Phase & Prognostic Clearance
PreS1-Ag appears in the pre-icteric/incubation window alongside (or just after) the very earliest HBV-DNA — often before HBeAg peaks and well before liver enzymes crash. Its kinetics during convalescence are the cleanest early-resolution flag:
• PreS1-Ag ↓ ↓ → loss = good (immune clearance winning)
• PreS1-Ag persistently (+) > 12 weeks → heightened risk of chronicity (HBsAg > 6 months)
Paired with IgM anti-HBc and ALT/AST trajectories, it turns "acute HBV" from a static diagnosis into a time-resolved immune clearance curve.
- Treatment Monitoring: Is the Virion Surface Actually Dropping?
Nucleos(t)ide analogues (entecavir, tenofovir) crush HBV-DNA within weeks — but HBsAg clearance lags years, and HBsAg can remain (+) long after replication halts (thanks to that ocean of empty subviral particles). PreS1-Ag, by contrast, tracks the Dane-particle surface, so if it stays (+) despite deep HBV-DNA suppression, you're looking at either:
• Residual low-level replication (pregenomic RNA still making virions)
• Or a preS1-Ag(+) genotypic escape the DNA test alone can't phenotype
Serial PreS1-Ag (baseline → week 12 → week 24 → week 48) alongside HBV-DNA, HBeAg, and HBsAg quant (IU/mL) gives the most granular readout of "is the infectious-particle surface coming down?"
- Perinatal / Vertical Transmission Risk Stratification
The preS1–NTCP interaction (aa 21–47) is the infection gate for the neonatal hepatocyte — so maternal PreS1-Ag(+) status (especially HBeAg(+) / high DNA) is not just "viral load" but a direct readout of the domain the baby's liver will see. Adding PreS1-Ag to the maternal screening beyond HBsAg titration is the translational logic that connects molecular virology to the obstetric delivery-room.
- Molecular Virology: preS1 Mutant Mapping
Certain immune-escape or vaccine-escape substitutions map near preS1 residues (though the NTCP-binding groove itself is under strong purifying selection because it's functionally constrained). Sequencing + PreS1-Ag ELISA on the same serum gives you the phenotypic correlate: "mutant arose, but is the surface antigen still assembling into PreS1-displaying particles?"
- Cell Culture / Hep-ADM Models
If you're running HepG2-NTCP, HepaRG, or PXB-mouse HBV infection models, supernatant PreS1-Ag (ELISA) is a fast surrogate for Dane-particle secretion rate that doesn't require a qPCR run per timepoint — especially handy for entry-inhibitor (myrcludex-B / bulevirtide) screens, where blocking the preS1–NTCP interaction should collapse extracellular PreS1-Ag on virions.
A Minimal Protocol You Can Paste Into Methods
- Collect serum or EDTA/citrate plasma, process within 2–4 h, spin 2,000–3,000 rpm (~1,500 ×g), 10 min, 4°C, aliquot, -80°C, label Biosafety Level 2, avoid >1 freeze–thaw.
- Do not use NaN₃ in any buffer (inhibits HRP).
- Dilute into kit buffer per manual (most protocols run neat or mild 1:2–1:5 dilution for serum).
- Warm reagents ≥ 30 min RT before opening; protect TMB from light; stop uniformly; read 450 nm promptly; fit 4-PL; run full standard curve per plate.
The Bottom Line
HBV's large surface protein carries a 108–119 aa N-terminal preS1 extension whose aa 21–47 segment binds NTCP — the sole known entry receptor into hepatocytes — and that same domain is secreted as preS1 antigen (PreS1-Ag) on Dane-particle surfaces, making it the one serology marker that tracks replication-competent, potentially infectious virions rather than empty 22-nm HBsAg clouds. When HBeAg(–) preC mutants blind the classic five-marker panel, PreS1-Ag is the flag that says "the virus is still here, still attaching, and still replicating." The Human Hepatitis B virus pre S1 antigen (HBV preS1-Ag) ELISA Kit — KTE62719 from Abbkine gives you that flag as a number: pre-coated anti-preS1 capture → biotin detection → HRP–TMB → 450 nm, in a quantitative sandwich format that slots into any HBV-serology or antiviral-monitoring workflow without a qPCR instrument.
Product Reference: KTE62719 – Human Hepatitis B virus pre S1 antigen (HBV preS1-Ag) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-hepatitis-b-virus-pre-s1-antigen-hbv-pres1-ag-elisa-kit-kte62719/
(For Research Use Only; not for diagnostic procedures in humans.)





