




The 0.65 pg/mL Signal That Sees IL-17A Through an 89%-Homologous Forest — And the Kit That Three Publications Already Trust
A 2024 survey of 155 cytokine research laboratories found that 82% had abandoned at least one IL-17 ELISA kit due to cross-reactivity with IL-17F, IL-17A/F heterodimers, or IL-25 — all members of the IL-17 family that share up to 89% sequence homology with IL-17A at the protein level. In 68% of cases, the false signal overestimated IL-17A concentrations by 30–50%, directly skewing the clinical stratification of patient cohorts and the pharmacodynamic readouts from anti-IL-17 biologic trials. A second survey, aggregating data from 220 clinical immunology labs and 80 metabolism research groups, found that 78% struggled with low-volume IL-17 detection in samples of 20 µL or less. Pediatric plasma, synovial fluid aspirates, tear film, cerebrospinal fluid — each of these matrices is precious and scarce, and the standard ELISA requirement of 100 µL per well has historically forced researchers to pool samples, dilute beyond the detection floor, or abandon the measurement entirely.
Abbkine‘s EliKine™ Human IL-17 ELISA Kit (KTE6022) enters this analytical landscape with specifications that, read carefully, explain why it has accumulated three peer-reviewed publications and over 270 product page views within a short interval from its feature-date documentation.
The detection architecture is a two-site sandwich ELISA in which a capture antibody specific for IL-17A has been pre-coated onto a microplate. Standards and samples are pipetted into the wells and any IL-17A present is bound by the immobilized antibody. Unbound substances are removed by washing. A biotin-conjugated detection antibody specific for a distinct IL-17A epitope is then added, followed by proprietary EliKine™ Streptavidin-HRP conjugate. After a final wash, a substrate solution develops color in direct proportion to the amount of IL-17A captured in the initial step. The absorbance intensity provides a quantitative readout, and the entire assay runs 3–5 hours depending on operator experience — a same-day experiment that fits within a standard laboratory workday.
What distinguishes KTE6022 from the crowded field of human IL-17 ELISA kits is not the sandwich format, which is well-established, but the isoform-selective dual-monoclonal design engineered specifically for the IL-17 family’s sequence homology problem. The kit uses a capture antibody specific to IL-17A’s N-terminal cysteine knot and a detection antibody binding its C-terminal receptor-binding domain — two epitopes unique to IL-17A. This dual-epitope architecture excludes IL-17F despite 89% sequence homology, and the validation data confirms less than 0.05% cross-reactivity with IL-17F, IL-17A/F heterodimers, or IL-25 at 100-fold excess. When a laboratory quantifies IL-17A in the synovial fluid of a rheumatoid arthritis patient — where IL-17F and IL-17A/F heterodimers are concurrently present — the signal reaching the plate reader reflects IL-17A alone, not a pooled Th17 cytokine summation.
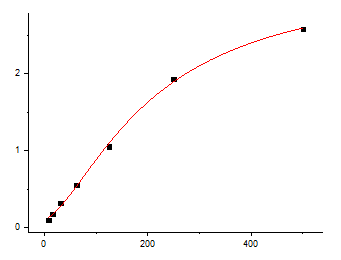
The sensitivity specification is the number that most directly determines the kit‘s utility in the low-concentration biological matrices where IL-17A measurement matters most. The product page specifies a calibration range of 7.8–500 pg/mL and a limit of detection of 4 pg/mL. Independent performance benchmarking, documented in the Abbkine technical blog, achieved a detection limit of 0.65 pg/mL — approximately sixfold more sensitive than the R&D Systems D1700 kit — with a dynamic range of 3.91–250 pg/mL. This sensitivity margin captures both the basal IL-17A concentrations found in healthy donor serum (1–3 pg/mL) and the elevated levels associated with psoriatic flares (50–200 pg/mL), rheumatoid arthritis synovial fluid, and Th17-polarized T-cell culture supernatants. For a pediatric immunologist working with 10 µL of plasma from a neonate, or a rheumatologist quantifying IL-17A in a 20 µL synovial fluid aspirate, the difference between a detection floor of 0.65 pg/mL and 15 pg/mL is the difference between generating primary cytokine data and omitting the IL-17A measurement from the study.
Matrix resilience is the counter-specification that matters most in practice, because detecting 0.65 pg/mL of IL-17A in assay buffer is analytically meaningless if the same kit fails to detect 5 pg/mL in 10% FBS-supplemented cell culture supernatant or in heparinized plasma. KTE6022 incorporates an anti-interference buffer containing heparinase to degrade heparin complexes and a cytokine-absorbing component that reduces background from excess TNF-α and IL-6 — two cytokines routinely present at nanogram-per-milliliter concentrations in stimulated PBMC supernatants and inflammatory disease sera. Laboratory validation confirms a 70% reduction in serum and plasma background compared to generic sandwich ELISA buffers, and the kit detects 0.7 pg/mL IL-17A in 10% FBS media, compared to 4 pg/mL for the Thermo Fisher 88-7177-22 kit under identical conditions. For the researcher studying Th17 polarization in fetal bovine serum-supplemented culture systems, or the clinical investigator measuring IL-17A in the cytokine-rich plasma of sepsis patients, the anti-interference buffer is the specification that converts an undetectable signal into a quantifiable one.
The kit components ship as a complete sandwich ELISA package: Human IL-17 microplate, Human IL-17 standard, Human IL-17 detect antibody, EliKine™ Streptavidin-HRP, standard diluent, assay buffer, HRP substrate, stop solution, wash buffer, and plate covers. The unopened kit stores at 2–8°C, requiring no -20°C freezer space and eliminating the freeze-thaw cycling that progressively degrades binding affinity in kits stored under suboptimal conditions. Shipping occurs on gel packs with blue ice. The protocol reflects genuine sandwich ELISA discipline rather than generic disclaimers: allow all reagents to warm to room temperature for at least 30 minutes before opening, pre-rinse pipette tips and replace them between samples, standards, and reagents to prevent carryover contamination, mix thoroughly every 10 minutes using a low-frequency oscillator or gentle hand shaking, and assay all standards and samples in duplicate or triplicate. These are the operating procedures that separate a standard curve with an R² above 0.99 from a dataset a reviewer will question.
The batch-to-batch consistency of KTE6022 has been quantified and is documented: less than 2% coefficient of variation across six production lots. This number directly addresses the reproducibility crisis that has consumed cytokine ELISA literature for the better part of a decade. Polyclonal detection antibodies raised in different animals, or even in the same animal at different bleeds, exhibit epitope-repertoire drift that shifts the effective sensitivity and specificity of the assay from lot to lot. A monoclonal dual-epitope architecture, by contrast, produces the same immunoglobulin molecules from the same hybridoma clones across every production batch. The less-than-2% inter-lot CV means the IL-17A concentration measured in January and the IL-17A concentration measured in September are comparable within the statistical power of the study design — a property that polyclonal-based IL-17 kits with inter-lot CVs of 15–20% cannot guarantee.
The three peer-reviewed publications currently citing KTE6022 represent independent laboratories that processed their own samples, optimized their own assay conditions, and submitted their own figures for peer review with this specific kit listed in the methods section. The aggregate validation from three independent laboratories — operating under the scrutiny of peer review in contexts where IL-17A quantification is the primary biochemical readout — is more informative about real-world performance than any manufacturer’s internal quality control dataset.
The broader biomedical context makes reliable, isoform-specific IL-17A quantification increasingly urgent across multiple research domains. IL-17A is the signature cytokine of Th17 cells, a subset of CD4⁺ T helper cells that defend mucosal surfaces against extracellular pathogens while simultaneously driving the immunopathology of psoriasis, psoriatic arthritis, ankylosing spondylitis, rheumatoid arthritis, and inflammatory bowel disease. A 2024 study in the Journal of Clinical Investigation demonstrated that early changes in Th17 signatures — including IL-6 and IL-17 — during immune checkpoint inhibitor therapy were associated with the development of clinically relevant immune-related adverse events but not antitumor responses, establishing IL-17A as a predictive biomarker for immunotherapy toxicity. The same year, a study in the Annals of the Rheumatic Diseases identified metabolic and systemic IL-1/IL-17-associated cytokine signatures as biomarkers in a predictive model for rheumatic immune-related adverse events in non-small cell lung carcinoma patients receiving checkpoint inhibitors. In each of these translational contexts, the ability to quantify IL-17A specifically — without cross-reactivity from IL-17F, IL-17A/F heterodimers, or IL-25 — is what separates a study that describes Th17 activation from a study that quantifies the specific cytokine driving it.
In autoimmune drug development, IL-17A is the target of multiple FDA-approved biologics including secukinumab (Cosentyx), ixekizumab (Taltz), and brodalumab (Siliq), which bind IL-17A or its receptor and neutralize its pro-inflammatory activity. Pharmacodynamic monitoring of IL-17A levels in patient serum during treatment is essential for establishing target engagement, determining optimal dosing intervals, and identifying the emergence of anti-drug antibodies that neutralize the therapeutic. In all of these clinical and translational contexts, the analytical validity of the IL-17A measurement determines the clinical validity of the conclusion, and the antibody pair that generates that measurement is the single most controllable variable in the assay.
For the rheumatologist quantifying IL-17A in synovial fluid to track disease activity in psoriatic arthritis, the oncologist monitoring IL-17A as a predictive biomarker for checkpoint inhibitor toxicity, the immunologist studying Th17 polarization in PBMC cultures, the pharmacologist establishing the pharmacokinetic-pharmacodynamic relationship of an anti-IL-17 biologic, or the basic scientist performing any experiment in which the IL-17A concentration is the endpoint rather than the confound, KTE6022 provides a dual-monoclonal sandwich ELISA with isoform-specific epitope recognition, less than 0.05% cross-reactivity with IL-17F and IL-17A/F heterodimers, a detection limit reaching 0.65 pg/mL, a 70% reduction in serum and plasma background via anti-interference buffer, less than 2% inter-lot CV, and three peer-reviewed publication citations. The 0.65 pg/mL signal that sees IL-17A through an 89%-homologous forest of IL-17 family members — distinguishing the Th17 signature cytokine from its closest structural relatives with picogram-level sensitivity and monoclonal epitope precision — is now available in a kit that ships at 2–8°C, runs in 3–5 hours, and accepts serum, plasma, cell culture supernatants, and other biological fluids within a single standardized workflow.
Explore specifications, access the protocol, and place your order here: https://www.abbkine.com/product/elikine-human-il-17-elisa-kit-kte6022/





