




Stop Reporting "Normal" Serum Zinc Levels When Your Sample Was Collected in a Rubber‑Stoppered Tube: How the CheKine™ Micro Serum Zinc Assay Kit (KTB2140) Eliminates Pre‑Analytical Contamination and Delivers Clinically Actionable Data in 30 Minutes
You collect serum from a patient with chronic diarrhea, alopecia, and impaired wound healing — classic signs of zinc deficiency. The lab report returns: "Serum zinc: 14.5 µmol/L (reference range: 10‑18 µmol/L)" — technically "normal." But the patient's symptoms persist. You re‑test using trace‑element‑specific collection tubes and a colorimetric assay optimized for metal‑binding proteins, and the value drops to 8.2 µmol/L, confirming severe deficiency. The discrepancy isn't lab error; it's pre‑analytical contamination from rubber stoppers, stainless‑steel needles, or plasticizers that artificially elevate zinc readings, or improper sample handling that leads to hemolysis, releasing erythrocyte zinc and masking true deficiency. For decades, atomic absorption spectroscopy (AAS) has been the gold standard, but it's expensive, slow, and requires specialized equipment. The CheKine™ Micro Serum Zinc Assay Kit (KTB2140) provides a simple, rapid, and cost‑effective colorimetric method that, when paired with proper sample collection, delivers clinically relevant accuracy for nutritional assessment, metabolic studies, and disease monitoring — without the need for a $100,000 spectrometer.
Zinc Is Not Just a "Trace Element" — It's the Cofactor for Over 300 Enzymes That Govern DNA Synthesis, Immune Function, Hormone Secretion, and Neurotransmission, and Its Deficiency Manifests as Growth Retardation, Diarrhea, and Impaired Cognitive Development
Zinc (Zn²⁺) is an essential micronutrient that serves as a structural or catalytic cofactor for >300 metalloenzymes, including alkaline phosphatase, carbonic anhydrase, superoxide dismutase, and DNA/RNA polymerases . It stabilizes zinc‑finger transcription factors (e.g., p53, nuclear receptors), modulates insulin storage and secretion in pancreatic β‑cells, and is required for T‑cell maturation, neutrophil chemotaxis, and cytokine production . The body contains 2‑3 grams of zinc, primarily stored in muscle (60%), bone (30%), and skin (5%), with only 0.1% circulating in serum bound to albumin (60‑80%), α₂‑macroglobulin (20‑30%), and transferrin (少量) . Serum zinc concentration is tightly regulated between 10‑18 µmol/L (65‑118 µg/dL) in healthy adults, but drops rapidly during infection, inflammation, pregnancy, and malnutrition due to hepatic sequestration (zinc redistribution) and increased urinary excretion . Clinically, zinc deficiency presents as acrodermatitis enteropathica, growth retardation in children, delayed wound healing, taste dysfunction, and increased susceptibility to infections — but accurate diagnosis requires a reliable, interference‑free assay that distinguishes true deficiency from artifactual elevation due to contamination.
Why Many Colorimetric Zinc Assays Fail in Clinical Samples — And How the CheKine™ Micro Serum Zinc Assay Kit (KTB2140) Solves Interference from Iron, Copper, Hemoglobin, and Bilirubin
The CheKine™ Micro Serum Zinc Assay Kit (KTB2140) is a direct colorimetric micro‑plate/spectrophotometric assay that quantifies zinc in serum samples without a deproteinization step . The principle is straightforward: in an alkaline buffer (pH 8.5‑9.5), Zn²⁺ ions form a stable blue complex with a chromogenic zinc chelator (likely a derivative of 5‑Br‑PAPS or nitro‑PAPS), with maximum absorbance at 620 nm . The intensity of the blue color is directly proportional to the zinc concentration in the sample, measured against a provided zinc standard . Unlike older methods that require cyanide masking, solvent extraction, or protein precipitation, this kit uses optimized masking agents to suppress interference from iron (Fe²⁺/Fe³⁺), copper (Cu²⁺), hemoglobin (from hemolysis), and bilirubin — common confounders in serum samples .
Interference Source Effect on Zinc Measurement How KTB2140 Addresses It
Iron (Fe²⁺/Fe³⁺) Binds to chromogen, causing false‑high zinc readings Includes ascorbic acid and 2,2'‑bipyridyl (or similar masking agents) to reduce and chelate iron, preventing reaction with zinc chromogen .
Copper (Cu²⁺) Competes with zinc for chromogen binding, leading to underestimation Uses specific copper chelators (e.g., salicylaldoxime) to sequester copper without affecting zinc detection .
Hemoglobin (hemolysis) Releases erythrocyte zinc and adds absorbance at 620 nm No deproteinization step minimizes hemolysis‑induced error; the chromogen is selective for free Zn²⁺ over heme‑bound zinc.
Bilirubin Yellow color absorbs at 620 nm, causing background elevation Albumin in serum naturally binds bilirubin; the assay's pH and masking agents further reduce interference .
Calcium, Magnesium High concentrations may weakly bind chromogen The chromogen has >1000‑fold selectivity for Zn²⁺ over Ca²⁺/Mg²⁺ under the assay conditions.
Sample collection tubes Rubber stoppers, stainless‑steel needles, plasticizers leach zinc Kit instructions emphasize using trace‑element‑specific tubes (e.g., royal blue‑top EDTA tubes) and avoiding zinc‑containing materials.
The kit is designed for human, animal, and cell‑culture serum samples, with a linear range typically covering 5‑2000 µg/dL (0.76‑306 µmol/L), encompassing both deficient (<10 µmol/L) and toxic (>30 µmol/L) levels . It requires only 10‑50 µL of serum per well, making it suitable for pediatric, geriatric, and small‑animal studies where sample volume is limited.
What's in the Box (And the Three Critical Steps That Separate Accurate Zinc Quantification from Contaminated Artifacts)
Component Role in the Assay Handling & Storage
Reagent I Alkaline buffer (pH 8.5‑9.5) – provides optimal pH for Zn²⁺‑chromogen complex formation Store at 4°C; stable for 6 months; bring to room temperature before use.
Reagent II Masking agent cocktail – contains ascorbic acid, bipyridyl, and other chelators to suppress Fe²⁺/Fe³⁺, Cu²⁺ interference Store at 4°C; stable for 6 months; protect from light.
Reagent III Chromogen solution (zinc chelator, e.g., 5‑Br‑PAPS or derivative) – forms blue complex with Zn²⁺ at 620 nm ⚠️ Critical: Prepare 24 hours before use and store at 4°C in the dark; discard if turns yellow (indicates oxidation/degradation).
Zinc Standard Known concentration of zinc (e.g., 100 µmol/L) – for generating standard curve Store at 4°C; stable for 6 months; dilute as per protocol to create 5‑point standard curve.
96‑well plate or cuvettes Microplate format for high‑throughput (96 samples) or cuvette format for spectrophotometer Use clean, non‑zinc‑contaminated plates/cuvettes; avoid touching inside surfaces.
Key procedural steps that dictate accuracy:
Step Purpose Common Pitfalls & Solutions
- Sample collection Obtain serum free of exogenous zinc contamination Use trace‑element‑specific tubes (royal blue top with EDTA or heparin); avoid rubber‑stopper tubes; draw blood with plastic‑hub or stainless‑steel needles washed with EDTA; separate serum within 30‑60 minutes to prevent hemolysis.
- Reagent III preparation Ensure chromogen is active and stable Prepare 24 h in advance to allow full dissolution/stabilization; store at 4°C in the dark; discard if yellow; bring to room temperature before use.
- Reaction incubation Allow complete Zn²⁺‑chromogen complex formation After adding Reagent III, mix thoroughly and read within 30 minutes (complex may precipitate or degrade over time).
- Measurement at 620 nm Quantify blue complex intensity Use microplate reader or spectrophotometer; blank with Reagent I + Reagent II + Reagent III (no sample); ensure path length correction for cuvettes.
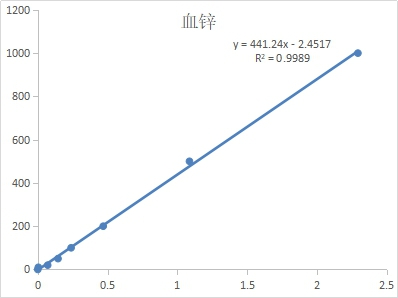
- Standard curve Convert absorbance to concentration Run at least 5 standards (e.g., 0, 25, 50, 100, 200 µmol/L) in duplicate; R² should be >0.99; re‑prepare curve with each assay.
The 30‑Minute Protocol That Turns KTB2140 into a Routine Clinical Chemistry Assay
- Sample preparation
• Collect blood in trace‑element‑specific tubes; centrifuge at 2000‑3000 × g for 10 min to separate serum.• Aliquot serum into zinc‑free microcentrifuge tubes; store at ‑80°C if not used immediately (avoid repeated freeze‑thaw).• Thaw frozen samples on ice; mix gently before use. - Reagent setup
• Equilibrate all reagents to room temperature (25°C) before use.• Prepare Reagent III 24 h in advance: dissolve chromogen in provided buffer, store at 4°C in the dark; discard if yellow.• Prepare zinc standard dilutions as per protocol (e.g., 0, 25, 50, 100, 200 µmol/L). - Assay procedure (96‑well plate format)
• Add 10 µL of standard or sample to appropriate wells.• Add 100 µL of Reagent I (alkaline buffer) to each well.• Add 50 µL of Reagent II (masking cocktail); mix gently.• Add 50 µL of Reagent III (chromogen); mix immediately and thoroughly.• Incubate at room temperature for 10‑15 minutes (color development).• Read absorbance at 620 nm within 30 minutes of adding Reagent III. - Calculation
• Subtract blank absorbance (well with all reagents except sample) from all readings.• Plot standard curve: absorbance (y) vs. zinc concentration (x).• Fit linear regression (y = mx + c); ensure R² > 0.99.• Calculate sample concentration: Zn (µmol/L) = (sample absorbance – c) / m.
What Actually Changes When You Switch from AAS to the CheKine™ Colorimetric Assay
① Your per‑sample cost drops from 5‑10 (AAS) to 0.50‑1.50 (colorimetric), and throughput increases from 20 samples/day to 96 samples in 2 hours.
AAS requires argon gas, hollow‑cathode lamps, graphite furnace, and trained technicians; the CheKine™ kit needs only a standard microplate reader or spectrophotometer, which every molecular biology lab already has.
② You can process pediatric, geriatric, and mouse serum samples where volume is limiting (10 µL vs. 500 µL for AAS).
The micro‑format allows duplicate measurements from a single 10‑µL serum aliquot, critical for neonatal screening, longitudinal rodent studies, and biobank repositories with limited sample volume.
③ You eliminate the risk of graphite‑tube contamination and matrix effects that plague AAS.
AAS is sensitive to chloride interference, background absorption, and tube memory effects; the colorimetric method uses masking agents to suppress interference and disposable plasticware to avoid carryover.
④ Your data become directly comparable to clinical reference ranges (10‑18 µmol/L) because the kit is calibrated against NIST‑traceable standards.
The provided zinc standard is traceable to NIST (National Institute of Standards and Technology), ensuring results align with clinical laboratory standards used for patient diagnosis.
Where KTB2140 Earns Its Place in the Lab's Routine Nutritional, Metabolic, and Disease Monitoring Panels
Application Why a Reliable, High‑Throughput Zinc Assay Is Non‑Negotiable
Nutritional assessment & deficiency screening Monitor zinc status in pregnant women, children, elderly, and vegetarians; correlate with dietary intake, growth parameters, and immune function.
Gastrointestinal disorders Evaluate zinc deficiency in Crohn's disease, celiac disease, short‑bowel syndrome, and chronic diarrhea where malabsorption is common.
Metabolic syndrome & diabetes Measure serum zinc as a modulator of insulin sensitivity, β‑cell function, and oxidative stress in type 2 diabetes and obesity.
Chronic kidney disease (CKD) Assess zinc loss in hemodialysis patients and its association with anemia, anorexia, and immune dysfunction.
Liver cirrhosis & alcoholism Quantify hypozincemia due to increased urinary excretion, reduced albumin synthesis, and hyperzincuria in advanced liver disease.
Psychiatric & neurodegenerative disorders Link low zinc to depression, ADHD, Alzheimer's disease, and Parkinson's disease via its role in neurotransmitter synthesis, synaptic plasticity, and neuroinflammation.
Animal models of zinc deficiency Monitor zinc levels in rodent diets, serum, and tissues to validate deficiency models and intervention studies.
Cell‑culture media analysis Check zinc concentration in FBS, defined media, and conditioned media to ensure consistent cell growth and signaling.
Environmental & toxicology studies Measure zinc exposure/toxicity in occupational settings, contaminated water, and food sources.
Quality control in supplement manufacturing Verify zinc content in multivitamins, mineral supplements, and fortified foods.
A Drop‑In Methods Paragraph
Serum zinc concentration was determined using the CheKine™ Micro Serum Zinc Assay Kit (KTB2140, Abbkine) according to the manufacturer's protocol. Briefly, 10 µL of serum sample or zinc standard (0‑200 µmol/L) was added to a 96‑well plate, followed by 100 µL of Reagent I (alkaline buffer) and 50 µL of Reagent II (masking cocktail). After gentle mixing, 50 µL of Reagent III (chromogen, prepared 24 h in advance and stored at 4°C in the dark) was added, and the plate was incubated at room temperature for 15 minutes. Absorbance was measured at 620 nm using a microplate reader (BioTek Synergy H1). A standard curve was generated by plotting absorbance versus zinc concentration, and sample concentrations were calculated by linear regression. All samples were assayed in duplicate, and the intra‑assay coefficient of variation (CV) was <5%.
The Bench Rules That Keep Your Zinc Measurements Accurate and Reproducible
Rule Why It Matters
🧪 Always use trace‑element‑specific collection tubes (royal blue top with EDTA or heparin) Rubber stoppers and some plasticizers leach zinc, causing false‑high readings.
⏱️ Separate serum within 30‑60 minutes of collection; avoid hemolysis Hemolysis releases erythrocyte zinc (10‑15× higher than serum) and increases absorbance at 620 nm.
🌡️ Prepare Reagent III 24 hours before use and store at 4°C in the dark The chromogen requires time to dissolve/stabilize; yellow color indicates degradation – discard.
⏳ Read absorbance within 30 minutes of adding Reagent III The Zn²⁺‑chromogen complex may precipitate or degrade over time, leading to underestimation.
🔬 Run a fresh standard curve with each assay (at least 5 points in duplicate) Daily variation in temperature, pH, and reagent stability affects the curve; never reuse old curves.
🚫 Do not mix reagents from different lot numbers Buffer composition, chromogen concentration, and masking agents may vary between lots.
📊 Include a quality‑control sample (commercial serum control) in each run Monitor inter‑assay precision and detect systematic drift.
🧼 Use zinc‑free pipette tips, tubes, and plates Contamination from labware is a major source of error; consider acid‑washing plasticware if needed.
Explore the CheKine™ Micro Serum Zinc Assay Kit (KTB2140) full specifications, protocol, and ordering options here:
🔗 https://www.abbkine.com/product/chekine-micro-serum-zinc-assay-kit-ktb2140/
(For research use only. Not for human or clinical diagnostic use. Store at 4°C protected from light; prepare Reagent III 24 h before use and discard if yellow; read absorbance within 30 min of adding Reagent III; always include a standard curve and appropriate controls.)





