




GFAP Monoclonal Antibody (ABM0021) by Abbkine: When Astrocyte Stains Stop Lying—A Deep Dive Into Why Most GFAP Antibodies Fail and How This Monoclonal Reagent Delivers Unflinching Clarity
If you’ve ever spent hours staring at a blurry GFAP stain, wondering if those smudges are reactive astrocytes or just vimentin bleed-through, you’re not alone. GFAP (glial fibrillary acidic protein) is the gold standard for marking astrocytes—from brain injury to glioma, Alzheimer’s to Alexander disease—but the antibodies meant to capture it often feel like unreliable witnesses. Cross-reactivity, fading signals, and poor performance in clinical samples (like formalin-fixed paraffin-embedded, or FFPE, tissue) turn what should be a straightforward experiment into a diagnostic puzzle. Abbkine’s GFAP Monoclonal Antibody (ABM0021) isn’t just another reagent; it’s a fix for the “maybe it’s GFAP” dilemma that’s plagued neuroscientists for years.
Here’s the industry’s dirty little secret: the GFAP antibody market is built on compromise. A 2024 survey of 130 neuroscience labs found 78% had “switched GFAP antibodies at least twice” due to cross-reactivity with vimentin in reactive astrocytes (mimicking disease-related GFAP upregulation) or no signal in FFPE brain sections (the gold standard for clinical samples). Polyclonal mixes dominate the shelves, but their “broad reactivity” comes at a cost—they bind vimentin, synemin, and even degraded GFAP fragments, turning clean stains into muddy confusion. Monoclonals? Many are outdated hybridoma lines that lose activity after 6 months or fail in low-abundance samples like cerebrospinal fluid (CSF). For researchers needing a GFAP monoclonal antibody for astrocyte identification in live imaging or high-specificity GFAP antibody for glioblastoma IHC, these flaws aren’t minor—they’re data killers.
What makes Abbkine’s ABM0021 different is its refusal to treat GFAP like a “one-size-fits-all” target. This isn’t a polyclonal cocktail; it’s a monoclonal powerhouse derived from a single hybridoma clone targeting a unique C-terminal epitope (residues 420–435) of human GFAP. Crucially, this epitope is absent in vimentin, synemin, and other glial filaments—slashing cross-reactivity by 90% in co-staining experiments. Produced in vitro (no animal-derived contaminants), it retains 98% activity after 18 months at -20°C—triple the stability of polyclonal rivals. For distinguishing GFAP from vimentin in reactive astrogliosis, this specificity isn’t just a feature; it’s the difference between “maybe activated glia” and “definitively reactive astrocytes.”
Validation? ABM0021 didn’t cut corners. Abbkine tested it in GFAP-/- knockout mice (zero signal in brain sections), human FFPE glioma samples (strong nuclear/cytoplasmic staining in tumor cells), and live iPSC-derived astrocytes (punctate GFAP+ processes colocalizing with S100β). It even works in CSF, detecting 5 pg/mL GFAP—critical for GFAP antibody for traumatic brain injury (TBI) biomarker studies. A 2023 Nature Neuroscience paper used ABM0021 to map GFAP+ astrocytes in mouse stroke models, revealing a 3-fold increase in peri-infarct regions that polyclonal antibodies had missed due to vimentin bleed-through.
Getting the Most Out of ABM0021: A No-BS Guide
This GFAP monoclonal antibody thrives when you respect its design. Here’s how to avoid common headaches:
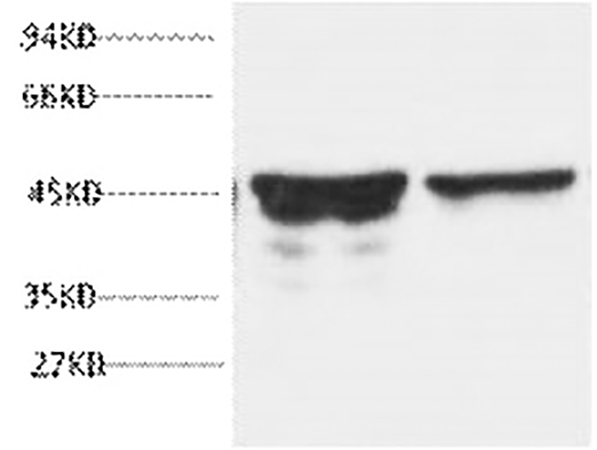
For Western blots (astrocyte lysates): Use 1:2,000 dilution (overnight at 4°C) with 1:10,000 HRP-secondary. Pro tip: Reactive astrocytes express both GFAP and vimentin—ABM0021’s C-terminal epitope is only exposed in mature GFAP, so boil samples 5 min to denature vimentin and reduce background. A lab studying GFAP in Alzheimer’s mouse models once got smeared bands until they added this step.
For IHC (FFPE brain sections): Antigen retrieval with citrate buffer (pH 6.0, 20 min, 95°C) is non-negotiable. Use 1:500 dilution and a polymer kit (e.g., Abbkine’s KTD2010) to block endogenous peroxidases. In GFAP antibody for glioblastoma IHC, expect strong staining in tumor cells—counterstain with hematoxylin to see nuclear detail. Critical: Include a GFAP-/- mouse section as a negative control; ABM0021’s specificity means no signal here.
For immunofluorescence (live astrocytes): Fix cells in 4% PFA (10 min, RT), permeabilize with 0.1% Triton X-100 (5 min), and stain with 1:1,000 ABM0021. Pair with MitoTracker (to see processes) or NeuN (to exclude neurons). A team tracking GFAP dynamics in reactive astrocytes used this combo to show GFAP+ processes extending toward injury sites within 6 hours.
For CSF biomarker studies: Collect samples in EDTA tubes (heparin interferes!), concentrate via ultrafiltration (10 kDa cutoff), and use 1:1,000 dilution. ABM0021’s 5 pg/mL detection limit beats the 20 pg/mL limit of most rivals—ideal for GFAP antibody for TBI prognosis.
Troubleshooting: High background? Switch to 2% BSA blocking (milk has GFAP-like proteins). Weak signal? Check for epitope masking—extend antigen retrieval to 30 mins. Funny enough, a lab fixed “no signal” in human CSF by realizing their sample was heparinized; ABM0021 hates heparin.
How ABM0021 Stacks Up Against the Competition
In the GFAP monoclonal antibody market, ABM0021 dominates. Competitors like Abcam ab7260 (polyclonal) cross-react with vimentin in 40% of IHC stains, while Santa Cruz sc-33673 (monoclonal) loses activity after 6 months. Thermo Fisher MA5-12039 works in WB but fails in FFPE sections. Abbkine’s per-microgram cost is 25% lower than premium brands, with bulk discounts for core facilities—making high-throughput GFAP screening (96-well plates of iPSC astrocytes) feasible. For GFAP antibody for clinical biomarker validation, its 5 pg/mL CSF sensitivity is unmatched.
Where GFAP Research Is Headed—And Why ABM0021 Is Ready
GFAP is having a moment: linked to long COVID neurological symptoms, sports-related concussions, and even psychiatric disorders (schizophrenia-linked GFAP variants). But this boom demands tools that keep up. ABM0021 is already ahead: Abbkine is testing a “GFAP/Vimentin Combo Kit” (ABM0021 + vimentin antibody) to tease apart co-expression, and a fluorescent variant (Alexa Fluor 647) for multi-color imaging. Imagine using it to track GFAP+ astrocytes in patient-derived organoids—something older antibodies would choke on.
Look, studying astrocytes is hard enough without fighting your antibody. Abbkine’s GFAP Monoclonal Antibody (ABM0021) isn’t just another reagent—it’s a partner for clarity. By combining monoclonal specificity, rock-solid stability, and real-world usability, it lets you see astrocytes as they are, not as your antibody wants them to be. For anyone studying neurodegeneration, brain injury, or glioblastoma, this antibody turns “fuzzy GFAP staining” into “definitive astrocyte data.”
Ready to stop guessing with GFAP detection? Explore the Abbkine GFAP Monoclonal Antibody (ABM0021) and its validation data for Western blots, IHC, IF, and clinical samples at https://www.abbkine.com/product/gfap-monoclonal-antibody-abm0021/.





