




VEGF: The Angiogenic Switch in Health and Disease – How the Abbkine EliKine™ Human VEGF ELISA Kit (KTE6033) Delivers Unmatched Sensitivity for Biomarker Discovery and Drug Development
If you could track the molecular signals that dictate where and when new blood vessels form—a process fundamental to embryonic development, wound healing, and the relentless growth of tumors—you would find one master regulator at the center: Vascular Endothelial Growth Factor (VEGF). This potent cytokine, originally identified as a vascular permeability factor, is the principal conductor of angiogenesis, orchestrating endothelial cell proliferation, migration, and survival to build the vascular networks that supply oxygen and nutrients to tissues . Beyond its physiological roles, VEGF is a double-edged sword: its pathological overexpression fuels the chaotic, leaky vasculature of solid tumors, drives vision‑loss in diabetic retinopathy and age‑related macular degeneration, and exacerbates inflammation in rheumatoid arthritis . Consequently, quantifying VEGF protein levels with precision is not just an assay—it's a critical diagnostic and research imperative, enabling the stratification of cancer patients, monitoring anti‑angiogenic therapy response, and unraveling mechanisms in cardiovascular and ocular diseases. Yet, measuring VEGF in complex biological matrices like serum, plasma, or tumor supernatants poses significant challenges: the protein exists in multiple splice variants (e.g., VEGF121, VEGF165), circulates at low picogram‑per‑milliliter concentrations, and can be masked by binding proteins . The Abbkine EliKine™ Human VEGF ELISA Kit (KTE6033) rises to this challenge, offering a high‑sensitivity, sandwich‑format colorimetric assay specifically designed to detect human VEGF‑A (including the predominant VEGF165 isoform) with a detection limit of 16 pg/mL and a broad dynamic range of 31.25–2000 pg/mL . Whether you are profiling VEGF as a prognostic biomarker in cancer patient sera, screening anti‑angiogenic drug candidates in vitro, or investigating VEGF dynamics in stem‑cell‑derived organoids, this kit provides the specificity, reproducibility, and ease‑of‑use required to generate publication‑grade data that advances both basic science and translational medicine.
The VEGF Signaling Axis: From Physiological Vasculogenesis to Pathological Angiogenesis
Human VEGF‑A (UniProt P15692, gene ID 7422) is a 45‑kDa homodimeric glycoprotein belonging to the platelet‑derived growth factor (PDGF) superfamily, with its gene producing multiple isoforms through alternative splicing (VEGF121, VEGF145, VEGF165, VEGF189, VEGF206) . The VEGF165 isoform is the most abundant and biologically active in humans, exhibiting both diffusible and heparin‑binding properties . VEGF exerts its effects primarily by binding to two tyrosine kinase receptors on endothelial cells: VEGFR‑1 (Flt‑1), which modulates monocyte migration and vascular patterning, and VEGFR‑2 (KDR/Flk‑1), the key mediator of mitogenic, chemotactic, and permeability‑enhancing signals . Under normoxic conditions, VEGF expression is tightly regulated and maintains vascular quiescence; however, hypoxia—a hallmark of solid tumors and ischemic tissues—triggers a dramatic upregulation via hypoxia‑inducible factor‑1α (HIF‑1α) . This “angiogenic switch” turns VEGF into a potent driver of pathological neovascularization, promoting the formation of immature, hyper‑permeable vessels that facilitate tumor metastasis, edema in diabetic retinopathy, and pannus formation in rheumatoid arthritis . Notably, circulating VEGF levels correlate with tumor stage, metastatic burden, and poor prognosis in numerous cancers, including colorectal, breast, lung, and prostate malignancies . In ophthalmology, intraocular VEGF concentration is a direct therapeutic target, with anti‑VEGF biologics (bevacizumab, ranibizumab, aflibercept) revolutionizing the management of wet age‑related macular degeneration and diabetic macular edema . Thus, accurate, sensitive quantification of VEGF is indispensable for understanding disease mechanisms, identifying patient subsets for targeted therapy, and monitoring treatment efficacy.
Kit Principle: A Robust Sandwich ELISA Engineered for Complex Biological Samples
The Abbkine EliKine™ Human VEGF ELISA Kit employs a classical two‑site immunoenzymometric (sandwich) assay optimized for minimal hands‑on time and maximal reliability in diverse sample matrices . Step 1: A monoclonal anti‑human VEGF‑A antibody is pre‑coated onto the wells of a 96‑well microplate. Step 2: Standards (recombinant human VEGF‑A) or samples are added; any VEGF‑A present binds to the immobilized capture antibody during a 2‑hour incubation at room temperature. Step 3: After washing away unbound material, a biotin‑conjugated polyclonal anti‑human VEGF‑A detection antibody is added, forming an antibody‑antigen‑antibody “sandwich.” Step 4: Following another wash, proprietary EliKine™ Streptavidin‑Horseradish Peroxidase (HRP) conjugate is added, which binds with high affinity to the biotin on the detection antibody. Step 5: A TMB (3,3’,5,5’‑tetramethylbenzidine) substrate is introduced; HRP catalyzes its conversion to a blue chromogen, which turns yellow upon addition of stop solution (sulfuric acid). Step 6: Absorbance is measured at 450 nm (with 570 nm or 630 nm reference optional). The absorbance intensity is directly proportional to the amount of VEGF‑A captured in the initial step . Key performance specifications include:
• Detection range: 31.25–2000 pg/mL, covering physiological and pathological concentrations in human serum, plasma, and cell culture supernatants .
• Sensitivity (Limit of Detection): 16 pg/mL (calculated as mean blank + 2SD), enabling reliable detection of low‑abundance VEGF in early‑stage disease or unstimulated cell cultures .
• Specificity: The matched antibody pair shows no significant cross‑reactivity with human VEGF‑B, VEGF‑C, VEGF‑D, VEGF‑E, or other common cytokines, ensuring accurate quantification of VEGF‑A even in complex lysates .
• Precision: Intra‑assay and inter‑assay coefficients of variation (CV) are typically <10% and <12%, respectively, guaranteeing reproducible results across operators and plates .
• Sample compatibility: Validated for human serum, plasma (EDTA, heparin, citrate), cell culture supernatants, tissue homogenates, and other biological fluids; most samples require only simple dilution before assay .
• Standard traceability: The lyophilized recombinant VEGF‑A standard is traceable to NIBSC (National Institute for Biological Standards and Control) references, ensuring accuracy and comparability across laboratories .
The entire protocol can be completed in 3–5 hours with less than 2 hours of active hands‑on time, making it ideal for medium‑ to high‑throughput screens.
Five Transformative Applications of the Abbkine VEGF ELISA Kit in Cutting‑Edge Research
Research Area Specific Investigation How KTE6033 Provides the Answer
Oncology & Cancer Biomarker Discovery Correlating serum or plasma VEGF levels with tumor stage, metastasis, and overall survival in colorectal, breast, or non‑small‑cell lung cancer (NSCLC) patients. Quantify VEGF in pre‑treatment and post‑treatment serum samples to establish prognostic value and monitor response to anti‑VEGF therapies (e.g., bevacizumab) .
Ophthalmic Disease Research Measuring vitreous or aqueous humor VEGF concentrations in patients with diabetic retinopathy (DR) or wet age‑related macular degeneration (AMD) to guide anti‑VEGF injection schedules. Use the kit to track VEGF reduction after intravitreal anti‑VEGF drug administration, correlating cytokine levels with optical coherence tomography (OCT) findings and visual acuity .
Cardiovascular & Ischemic Disease Models Assessing VEGF upregulation in myocardial infarction or hind‑limb ischemia models to evaluate pro‑angiogenic gene or cell therapies. Quantify VEGF in tissue homogenates or plasma from animal models to confirm therapeutic VEGF induction and correlate with capillary density and functional recovery .
Drug Discovery & Anti‑Angiogenic Screening Evaluating the potency of novel small‑molecule VEGFR inhibitors or monoclonal antibodies in blocking VEGF‑induced endothelial cell proliferation. Measure residual VEGF in conditioned media of endothelial cells (HUVECs) treated with candidate drugs; generate IC50 curves for lead optimization .
Stem Cell & Organoid Research Optimizing differentiation protocols for endothelial cells or vascularized organoids by monitoring VEGF secretion as a marker of vascular commitment. Quantify VEGF in day‑by‑day culture supernatants to identify peaks of angiogenic activity and refine growth factor cocktails .
Streamlined Workflow: From Sample to Quantitative Data in One Afternoon
① Sample Preparation
• For serum/plasma, collect blood in EDTA tubes, centrifuge at 1,000–2,000 × g for 15 min within 30 min of collection; aliquot and store at –80°C.
• For cell culture supernatants, centrifuge at 500 × g for 5 min to remove cells and debris.
• For tissue homogenates, homogenize tissue in cold PBS with protease inhibitors, centrifuge at 10,000 × g for 10 min at 4°C, and collect supernatant.
• Avoid repeated freeze‑thaw cycles (>3 cycles); dilute samples if expected concentrations exceed 2000 pg/mL using the provided assay buffer.
② Reagent & Standard Preparation
• Equilibrate all kit components to room temperature (18–25°C) for 30 min before use.
• Reconstitute the lyophilized VEGF‑A standard with the provided diluent to generate a 2000 pg/mL stock solution.
• Prepare a 7‑point standard curve via serial dilution (e.g., 1:2 dilutions) covering 31.25–2000 pg/mL.
• Prepare Working Detection Antibody and Streptavidin‑HRP Working Solution by diluting as instructed.
• Prepare 1× Wash Buffer by diluting the 20× concentrate with distilled water.
③ Assay Procedure
• Add 100 µL of standard or sample to appropriate wells (duplicate/triplicate recommended).
• Cover with plate sealer and incubate 2 hours at room temperature with gentle shaking.
• Aspirate and wash each well 4 times with 300 µL Wash Buffer (soak 30 sec per wash).
• Add 100 µL of Working Detection Antibody; incubate 1 hour at room temperature.
• Wash as in step 3.
• Add 100 µL of Streptavidin‑HRP Working Solution; incubate 45 minutes at room temperature.
• Wash as in step 3.
• Add 100 µL of TMB Substrate; incubate 15–30 minutes at room temperature in the dark.
• Add 50 µL of Stop Solution; read absorbance at 450 nm within 30 min.
④ Data Analysis
• Subtract the average absorbance of the blank (zero standard) from all readings.
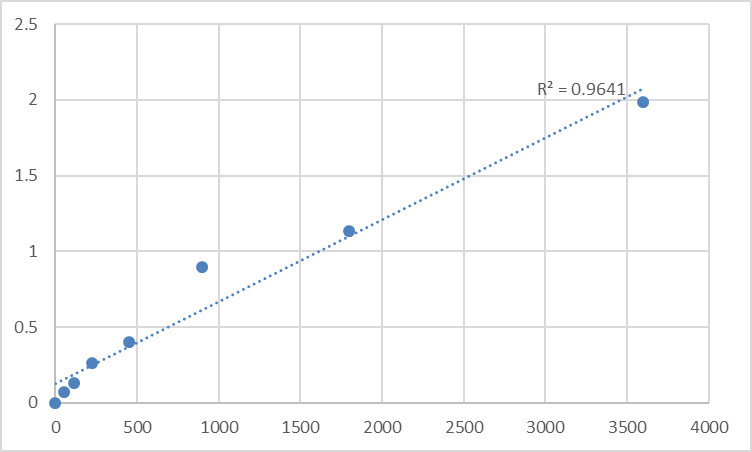
• Plot the standard curve (absorbance vs. concentration) using a 4‑parameter logistic (4PL) curve‑fit.
• Interpolate sample concentrations from the curve; multiply by dilution factor if applicable.
⑤ Quality Control
• Include a kit‑provided positive control and a pooled normal human serum in each run.
• Acceptable criteria: standard‑curve R² >0.99, CV of replicates <15%, spike‑recovery 80–120%.
Performance Benchmark: How the EliKine™ Kit Compares to Other VEGF Detection Platforms
Method Principle Sensitivity Time per 96 Samples Throughput Best Application
EliKine™ Sandwich ELISA (KTE6033) Colorimetric sandwich ELISA with biotin‑streptavidin amplification. High (16 pg/mL) 3–5 hours High (96‑well plate) Routine quantification in serum, plasma, cell supernatants; medium‑high throughput.
Electrochemiluminescence (MSD, Meso Scale Discovery) Electrochemiluminescent detection on carbon electrode arrays. Ultra‑High (<1 pg/mL) 2–3 hours + plate read High (multiplex up to 10‑plex) Ultra‑sensitive multiplex cytokine profiling in low‑volume samples (e.g., vitreous humor).
Luminex/xMAP Bead‑Based Assay Fluorescent‑coded microspheres with detection antibodies. Moderate‑High (5–10 pg/mL) 4–5 hours + bead acquisition High (multiplex up to 50‑plex) Multiplex cytokine screening in discovery‑phase studies.
Western Blot SDS‑PAGE separation, immunodetection with anti‑VEGF antibody. Low (ng range, semi‑quantitative) 1–2 days Low (10–20 samples/gel) Detecting VEGF isoforms (e.g., VEGF121 vs. VEGF165) and precursor processing.
Quantitative PCR (qPCR) mRNA quantification of VEGF gene (VEGFA). N/A (measures mRNA, not protein) 3–4 hours Medium Assessing transcriptional regulation of VEGF; does not reflect secreted protein.
Immunohistochemistry (IHC) Tissue‑section staining with anti‑VEGF antibodies. Semi‑quantitative (H‑score) 1–2 days Low Spatial localization of VEGF in tumor microenvironment or retinal sections.
The EliKine™ kit offers an optimal balance of sensitivity, cost‑effectiveness, and workflow simplicity, making it the preferred choice for labs that require reliable, single‑plex VEGF‑A quantification without investing in expensive multiplex instrumentation. It is more quantitative and higher‑throughput than Western blot or IHC, more accessible than MSD/Luminex for single‑analyte studies, and provides direct protein measurement unlike PCR.
Troubleshooting Guide for Reliable VEGF Quantification
Issue Potential Cause Recommended Solution
High background across all wells Contaminated wash buffer (microbial growth); incomplete washing (residual HRP); non‑specific binding from samples with high lipid or hemoglobin content. Prepare fresh wash buffer with Milli‑Q water; ensure 30‑sec soak per wash; pre‑dilute lipemic or hemolyzed samples 1:2–1:5 in assay buffer.
Poor standard curve fit (R² <0.98) Improper serial dilution technique; standard not mixed thoroughly after reconstitution; incubation temperature inconsistent. Use calibrated pipettes and fresh tips for each dilution; vortex standard stock for 30 sec; perform all incubations in a temperature‑controlled incubator/shaker.
Low or undetectable signal in cell culture supernatants VEGF concentration below detection limit (unstimulated cells); protease degradation during sample handling; sample pH incompatible. Stimulate cells with hypoxia (1% O₂) or pro‑angiogenic factors (bFGF, PMA) for 24–48 h to induce VEGF; add protease inhibitors during collection; adjust sample pH to neutral.
High intra‑assay variation (CV >15%) Inconsistent pipetting of viscous samples (e.g., serum); bubble formation during reagent addition; edge effects in microplate. Use reverse pipetting for serum/plasma; tap plate gently after each addition; avoid using outer wells or pre‑condition plate with assay buffer for 1 min.
Signal saturation at high sample concentrations VEGF level exceeds upper limit of detection (2000 pg/mL)—common in tumor‑bearing mouse serum or concentrated tumor supernatants. Pre‑dilute samples 1:10–1:100 in assay buffer and re‑assay; validate dilution linearity via spike‑and‑recovery.
Discrepancy between duplicate wells Inadequate mixing of samples before loading; uneven washing (clogged washer manifolds); plate not sealed properly during incubation. Vortex samples briefly before loading; check washer nozzles for blockage; ensure plate sealer is firmly attached.
Best Practices for Publication‑Quality VEGF Data
Practice Rationale & Implementation
Standardize sample collection & processing For clinical serum/plasma, collect in EDTA tubes (inhibits clotting and preserves cytokines), process within 2 hours, aliquot, and store at –80°C. Avoid repeated freeze‑thaw cycles (>3).
Include appropriate controls in each run Always run a blank (zero standard), the kit‑provided positive control, and a pooled normal human serum/plasma as a negative control. For cell experiments, include unstimulated cell supernatant as baseline.
Validate dilution linearity & spike recovery for each sample type Perform a spike‑and‑recovery experiment by adding a known amount of recombinant VEGF‑A to a representative sample matrix (e.g., patient serum). Acceptable recovery is 80–120%.
Use a 4‑parameter logistic (4PL) curve fit for data analysis The 4PL model accurately captures the sigmoidal dose‑response of ELISA; avoid linear regression, which can distort values at the curve's extremes.
Benchmark against an orthogonal method periodically Compare ELISA results with a Luminex bead‑based assay or MSD electrochemiluminescence for a subset of samples to ensure correlation (expect R² >0.90).
Document kit lot number & storage conditions Record the kit lot number, expiration date, and storage temperature (2–8°C) in your lab notebook; this is essential for publication and ensures experimental reproducibility.
Randomize sample placement on plate To minimize positional bias, randomize samples across the plate rather than grouping all controls or treatments together.
From Bench to Bedside: Translational Applications of Precise VEGF Measurement
① Prognostic biomarker in oncology
The kit enables longitudinal monitoring of serum VEGF in cancer patients, correlating levels with tumor stage, metastatic burden, and overall survival, and predicting response to anti‑VEGF therapies like bevacizumab or tyrosine kinase inhibitors .
② Guidance for anti‑VEGF therapy in ophthalmology
Researchers and clinicians can quantify vitreous VEGF in diabetic retinopathy or wet AMD patients to tailor anti‑VEGF injection frequency, reduce treatment burden, and improve visual outcomes .
③ Evaluation of pro‑angiogenic therapies in ischemic diseases
Scientists can measure VEGF in plasma or tissue homogenates from myocardial infarction or critical limb ischemia models to assess the efficacy of gene therapy, stem cell therapy, or biomaterial‑based VEGF delivery .
④ Drug discovery and potency testing
Pharmaceutical and biotech labs use the kit as a high‑throughput pharmacodynamic readout to evaluate the neutralizing capacity of novel anti‑VEGF biologics, small‑molecule VEGFR inhibitors, or natural product extracts .
⑤ Stem cell and tissue engineering research
The assay is ideal for monitoring VEGF secretion during endothelial differentiation of induced pluripotent stem cells (iPSCs) or in vascularized organoid cultures, enabling optimization of differentiation protocols .
A Ready‑to‑Use Methods Section for Your Manuscript
VEGF‑A concentration was quantified using the EliKine™ Human VEGF ELISA Kit (Abbkine, KTE6033) according to the manufacturer's instructions. Briefly, serum samples (diluted 1:2 in assay buffer) or cell culture supernatants were added to anti‑VEGF‑A pre‑coated 96‑well plates and incubated for 2 h at room temperature with gentle shaking. After washing, biotinylated detection antibody was added for 1 h, followed by Streptavidin‑HRP conjugate for 45 min. TMB substrate was added for 20 min, the reaction stopped with sulfuric acid, and absorbance measured at 450 nm (reference 570 nm) on a microplate reader (Bio‑Rad iMark). A four‑parameter logistic (4PL) standard curve (31.25–2000 pg/mL) was used to interpolate sample concentrations. All samples were assayed in duplicate, and the mean intra‑assay coefficient of variation (CV) was <10%. VEGF‑A levels are expressed as pg/mL.
Why the Abbkine EliKine™ Human VEGF ELISA Kit (KTE6033) Is the Gold Standard for Angiogenesis Research
① Exceptional sensitivity and specificity – with a detection limit of 16 pg/mL and no cross‑reactivity with VEGF‑B/C/D/E isoforms, the kit reliably quantifies VEGF‑A even in basal‑level samples like normal serum or unstimulated cell media .
② Broad dynamic range – the 31.25–2000 pg/mL range accommodates both low physiological concentrations and the high VEGF levels found in tumor microenvironments or pathological sera, eliminating the need for sample re‑dilution .
③ Streamlined, time‑efficient protocol – the pre‑coated plate and ready‑to‑use reagents reduce hands‑on time to under 2 hours, with total assay completion in 3–5 hours, accelerating data generation for time‑sensitive experiments.
④ Superior reproducibility – intra‑assay CV <10% and inter‑assay CV <12% meet the stringent reproducibility standards required for publication in high‑impact journals (e.g., Cancer Research, Angiogenesis, Investigative Ophthalmology & Visual Science).
⑤ Cost‑effective without compromising quality – compared to multiplex platforms (MSD, Luminex), the kit provides affordable, single‑plex quantification ideal for labs focused on VEGF as a primary endpoint, without the need for expensive instrumentation.
⑥ Backed by Abbkine's technical support – each lot is rigorously quality‑controlled for sensitivity, specificity, and lot‑to‑lot consistency, and the company offers detailed troubleshooting guides and responsive customer service.
Ready to illuminate the angiogenic switch with confidence? The Abbkine EliKine™ Human VEGF ELISA Kit (KTE6033) delivers exceptional sensitivity, specificity, and reproducibility—whether you're profiling VEGF as a cancer biomarker, optimizing anti‑angiogenic drug screens, or unraveling vascular dynamics in disease models. With pre‑coated plates, NIBSC‑traceable standards, and results in one afternoon, it's the turnkey solution for precise VEGF‑A quantification.
🔗 Product reference: KTE6033 (Abbkine) – https://www.abbkine.com/product/elikine-human-vegf-elisa-kit-kte6033/
(For research use only. Not for diagnostic or therapeutic procedures. Store at 2–8°C protected from light; stable for 12 months.)





