




The Glycoform That Betrays the Tumor: Why AFP-L3 — Not Just Total AFP — Is the Hepatocellular Carcinoma Readout You Actually Need
Most people think of alpha-fetoprotein (AFP) as the hepatocellular carcinoma (HCC) marker — until they realize that "elevated AFP" is also the hallmark of cirrhotic regeneration, acute viral hepatitis flares, and even pregnancy. The consequence? A soft, blunt instrument: total AFP catches the big, late, explosive HCCs, but it misses the smaller, early lesions — and worse, it fires alarms on benign liver disease that wastes MRI capacity and terrifies patients for nothing. That's where AFP-L3 enters the room. AFP-L3 is not a separate gene product — it is the Lens culinaris agglutinin (LCA)-reactive glycoform of AFP, defined by aberrant α1,6-core fucosylation and branched N-glycans acquired in the Golgi of malignant hepatocytes. Because this specific fucose branching pattern reflects the dysregulated glycosylation machinery of HCC cells (driven by FUT8, GnT-IVa/GnT-V), AFP-L3 becomes a tumor-specific glyco-biomarker hiding inside a classic "benign" protein — and the Human Alpha-fetoprotein Lens culinaris agglutinin 3 (AFP-L3) ELISA Kit (KTE60958) from Abbkine is engineered to fish it out of the noise.
AFP-L3 in One Sentence: Same Protein, Wrong Sugar — Unless It's Cancer
Human AFP (UniProt P02771) is a ~70 kDa oncofetal glycoprotein with three N-glycosylation sites (Asn223, Asn282, and a minor at Asn109 in some isoforms). In benign regenerating hepatocytes, those glycans are mostly bi/tri-antennary with minimal core fucosylation — so they don't bind LCA (Lens culinaris agglutinin, a fucose/glucose-binding tetrameric lectin). Malignant hepatocytes, by contrast, crank up GnT-V (MGAT5) and core α1,6-fucosyltransferase (FUT8), producing tri/tetra-antennary, core-fucosed N-glycans that do carry the LCA-binding epitope.
Clinically, the field partitions AFP into three lectin subfractions:
• AFP-L1 — non-LCA-bound (benign), ~60–90% of total AFP in non-HCC liver disease
• AFP-L2 — LCA-bound but from yolk-sac / non-hepatocellular (rarely dominant)
• AFP-L3 — the LCA-reactive glycoform arising from HCC
The metric that changed practice is the AFP-L3 percentage:
AFP-L3% = (AFP-L3 / Total AFP) × 100
Multiple guidelines and retrospective cohort studies converge on a cutoff of ≥ 10% (some centres use ≥ 15%) as a strong HCC discriminator — and crucially, AFP-L3% adds independent predictive value even when total AFP is still in the "gray zone" of 5–200 ng/mL, the zone where most early HCCs live and where total AFP is least reliable.
How You Actually Measure AFP-L3: The Lectin-Capture Logic
Because AFP-L3 differs from total AFP only by carbohydrate decoration, you cannot simply use a second anti-AFP antibody and call it a day — a standard anti-AFP sandwich ELISA will catch all AFP regardless of sugar. The trick is to select for the glycoform first, which is why the most validated architectures use LCA immobilized on the plate to selectively capture the LCA-binding fraction, followed by a detectable anti-AFP antibody to quantitate it:
KTE60958 — Conceptual Workflow:
- LCA (Lens culinaris agglutinin) is immobilized on the microplate wells (the "selective hook").
- Sample (serum/plasma) is added → only LCA-reactive AFP (AFP-L3) binds. Non-reactive AFP-L1 flows past.
- After washing, a high-affinity anti-AFP detection antibody (enzyme- or biotin-HRP labeled) reports the captured AFP-L3.
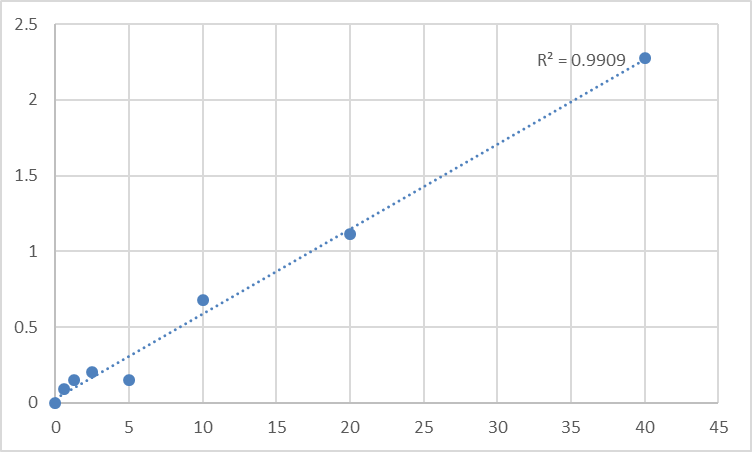
- TMB → stop → 450 nm read → interpolate from AFP-L3 standard curve (expressed in ng/mL).
- Total AFP is measured separately (same sample) → compute AFP-L3%.
This lectin-affinity capture → immuno-detection hybrid is the gold-standard principle behind the ECLIA/ELISA platforms that put AFP-L3 into Japanese and international HCC surveillance algorithms — and KTE60958 packages it as a ready-to-run, 96-well kit so your lab doesn't have to immobilize lectin or purify glycans by hand.
Performance Envelope You'll Cite (Representative for This Class)
Parameter Typical KTE60958-Class Spec
Target Human AFP-L3 (LCA-reactive glycoform of AFP)
Principle LCA lectin-capture + anti-AFP detection (sandwich-type)
Sample Types Serum, plasma (EDTA/citrate recommended)
Dynamic Range ~0.5–100 ng/mL (kit-specific; designed for clinical-range AFP-L3)
Sensitivity / LOD ≤ ~0.3–0.5 ng/mL
Intra-Assay CV < 8–10%
Inter-Assay CV < 10–12%
Required companion assay Total AFP ELISA (to calculate AFP-L3%)
Assay time ~2.5–4 hours
(As always, anchor exact range/LOD/recovery to your lot certificate and manual.)
Where AFP-L3 (and KTE60958) Actually Changes Patient Care & Research
- HCC Surveillance in High-Risk Cirrhosis (HBV/HCV/NASH)
The hardest question in liver clinics: who needs MRI/CT right now? Total AFP alone is too noisy. AFP-L3% ≥ 10% — even when total AFP is < 20 ng/mL — flags the "glyco-switch" of malignant hepatocytes. Running KTE60958 + total AFP ELISA on serial draws lets you build a kinetic AFP-L3% trend (rising % is worse than a static bump) and triage scans more intelligently.
- The "AFP Gray Zone" Problem (5–200 ng/mL)
This is where most early HCCs hide and where most false alarms waste resources. AFP-L3% is the differentiator: benign flare → AFP-L3% stays low; HCC → AFP-L3% rises. A plate-based ELISA lets you process cohort sera in batched sets, ideal for retrospective biobank studies validating imaging-free prescreen rules.
- Post-Ablation / Post-Resection Recurrence Monitoring
After curative-intent RFA or hepatectomy, rising AFP means recurrence — but what kind of recurrence? AFP-L3% rising again is a red flag for de novo or residual HCC rather than benign regenerating nodularity.
- Glycosylation Biology & FUT8/GnT-V Drug Targeting
If your lab works on hepatoma glycosylation, Golgi branching enzymes, or fucosylation inhibitors, AFP-L3 is the easiest circulating readout that proves your compound hit the right sugar-processing axis. An ELISA is far faster than DSA-FACE or LC-MS/MS glycopeptide mapping for routine PD.
- Comparative Biomarker Validation (PIVKA-II / DCP / AFP-L3 Triad)
The strongest HCC early-detection panels today combine des-gamma-carboxy prothrombin (DCP/PIVKA-II) + AFP-L3% + total AFP (and sometimes cfDNA methylation). KTE60958 gives you the third leg in a standardized plate format.
Sample Handling Rules That Decide Whether Your AFP-L3% Is Real
This is the section that saves you from a rejected figure:
• EDTA plasma preferred by many protocols (citrate acceptable; heparin can complicate lectin binding in some formats — check the manual).
• Process and freeze (-80°C) within 2 hours of draw; avoid >1 freeze–thaw (fucosylated glycoproteins can aggregate or degrade).
• Never run grossly hemolyzed serum without noting it — free hemoglobin can confound both lectin binding and HRP readout.
• Always run Total AFP on the same sample, same day if possible, and report AFP-L3 (ng/mL) AND AFP-L3%; reviewers and clinicians care about the percentage, not the raw ng/mL in isolation.
• Run a negative-control "non-HCC cirrhotic pool" on every plate to confirm your LCA capture isn't pulling L1 artifactually.
The Bottom Line
Total AFP tells you something is happening in the liver. AFP-L3 tells you whether that something is cancer. By exploiting the fact that HCC cells betray themselves with aberrant core fucosylation and branched N-glycans, the AFP-L3 assay converts a sugar pattern into a number — and the Human Alpha-fetoprotein Lens culinaris agglutinin 3 (AFP-L3) ELISA Kit (KTE60958) from Abbkine packages that logic as a lectin-capture → anti-AFP detection ELISA you can run on serum/plasma in a single morning. Paired with total AFP, it gives you the AFP-L3% that actually belongs in HCC surveillance, recurrence monitoring, and glycosylation-targeted therapy studies — not just as a clinical curiosity, but as a quantifiable, reproducible variable.
Product Reference: KTE60958 – Human Alpha-fetoprotein Lens culinaris agglutinin 3 (AFP-L3) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-alpha-fetoprotein-lens-culinaris-agglutiin-3-afp-l3-elisa-kit-kte60958/
(For Research Use Only; not for diagnostic procedures in humans.)





